
Abstract
Background
Considerable intermethod bias has been observed between cortisol immunoassays, with some also displaying a gender difference. Cortisol immunoassay performance is affected by serum matrix effects such as changes in steroid binding proteins and presence of interfering steroids which can be altered in various clinical settings. This study investigates cortisol immunoassay bias in pregnancy, renal failure and intensive care patients.
Methods
Serum remaining after routine analysis from pregnant patients, patients on the intensive care unit and patients with renal failure were obtained prior to disposal and used to create 20 anonymous samples per group. A male and female serum pool was prepared and spiked with cortisol. Samples were aliquoted and distributed to four hospitals for cortisol analysis by immunoassays from four different manufacturers. Cortisol was also measured by an isotope dilution-gas chromatography–mass spectrometry method for comparison of assay bias.
Results
Differences in cortisol immunoassay bias were observed across the different patient groups. A negative bias compared to pooled serum samples was observed for pregnancy serum, whilst a more positive bias was seen in renal failure and intensive care patients. Variation in bias was greatest in renal failure with the Roche E170 the most affected and the Abbott architect the least (interquartile ranges 44% and 14%, respectively).
Conclusions
Cortisol immunoassay bias may be affected by gender and differences in serum matrix from patients with various clinical conditions. Users of cortisol assays should be aware of differing matrix effects on their assay and the relevance of these for the interpretation of clinical results.
Introduction
National External Quality Assurance schemes demonstrate significant bias between cortisol immunoassays1,2 with a higher degree of interlaboratory variability apparent for pooled female samples largely due to the behaviour of the Roche Elecsys/E170 assay. 3 Whilst studies evaluating the cortisol response to adrenocorticotropic hormone (ACTH) stimulation have all demonstrated assay-dependent differences in the stimulated cortisol response,4–6 the findings on gender-related differences have been conflicting.5,6 Clark et al. 6 found that the response of serum cortisol to ACTH was gender-dependent although the extent of this varied between methods, whilst Klose et al. 5 did not observe any effect of gender. Previously, we were able to confirm that mean cortisol concentrations at baseline and post-ACTH did not differ between men and women using a gold standard gas chromatography–mass spectrometry (GC-MS) method. 4 However, gender-specific differences were found when cortisol was measured utilizing some immunoassays, with a clinically significant effect being found for the Roche E170 assay. This suggests that analytical factors specific to the immunoassays rather than genuine gender-related physiological differences are the cause of these observations. Differences in immunoassay bias relative to GC-MS have been reported between females taking or not taking oestrogen containing oral contraceptives (OCPs). 4 Matrix effects on cortisol immunoassay have also been demonstrated in patients in intensive care. Briegel et al. 7 demonstrated variation in cortisol immunoassay bias relative to GC-MS in patients with septic shock compared to those attending outpatients. Similarly, Barnes and Swaminathan 8 noted under-recovery of cortisol in a patient group with hypoalbuminaemia using the Bayer Advia Centaur assay.
It has long been recognized 9 that the specificity of a steroid immunoassay is determined not only by cross reactivity to steroids in serum but also the presence of steroid binding proteins and the affinity of the antibody used. There is increasing awareness that assay bias should be considered when interpreting cortisol measurements,4–6 but less information is available on the effect of variability in the serum matrix on cortisol measurement by immunoassay.
The aims of the current study were (1) to investigate measurement of cortisol by immunoassay in male and female serum and (2) to use relative bias as compared to GC-MS to investigate the effect of different serum matrices on immunoassay performance.
Methods
Sample preparation
Surplus serum was selected prior to routine disposal from specimens previously collected from adult patients attending the University Hospital of Wales. A total of 70 samples were prepared for analysis: five spiked samples from both a male and a female serum pool, and 20 each from pregnancy, renal failure and intensive care patients. All samples were mixed thoroughly after preparation, aliquoted and stored at −20℃ until analysis. All samples were anonymised prior to analysis.
Patient pools
Electronic patient records were searched for evidence of steroid use. Serum from any patient taking steroids was excluded from use in pooled samples. Two pools were created, one female and one male. For females, only samples where follicle stimulating hormone and luteinising hormone results were available were included. Pregnancy or oral contraceptive pill use were excluded by only including specimens with gonadotrophins within the range 1–10 U/L from women under 40 years of age, or a follicle stimulating hormone greater than 30 U/L in a woman over 50 years of age.
Each pooled sample was mixed by inversion for 30 min and split into five aliquots. Cortisol solution for spiking was prepared by dissolving Sigma hydrocortisone (H4001 1G, lot number 061M1142V) in methanol at a concentration of 0.1 mg/mL. This was diluted 1/10 with phosphate-buffered saline (PBS) to spike cortisol concentration in aliquots by 0, 100, 200 and 400 nmol/L. The final aliquot was spiked with cortisol by 800 nmol/L using 0.1 mg/mL in methanol, to ensure all spiking volumes were of 1% of pool volume or less. All volumes added were confirmed gravimetrically. Samples were then mixed by inversion for a further hour. Recoveries of cortisol by GC-MS in spiked patient pools were all within 6% of target, confirming accuracy of spike concentrations.
Pregnancy
Samples from second trimester Down’s syndrome screening were collected immediately prior to routine disposal. Samples were pooled pairwise to provide sufficient volume for the study. Twenty of these two patient pools were produced.
Intensive care
Samples from 20 patients in the intensive care unit (ICU) at the University Hospital of Wales, with albumin <20 g/L at the time of collection, were collected immediately prior to routine disposal. Ten male and 10 female patients were included. Due to reduced haematocrit, many samples were of sufficient volume without pooling; where this was not the case, multiple samples taken from the same patient within 48 h were pooled to provide sufficient volume. The patients’ notes were examined on the ward to ensure no patients were included who had recently received steroids.
Renal
Samples from patients who had a creatinine >300 µmol/L for at least three months were identified and collected immediately prior to routine disposal. Multiple samples from the same patient within 48 h were pooled as available; otherwise, samples were pooled pairwise as necessary for volume. The patients’ electronic records were examined for evidence of steroid use and samples from any patients on steroids excluded from use.
Welsh External Quality Assessment Scheme data
Bias information for each assay were taken from data provided by Welsh External Quality Assessment Scheme (WEQAS) for distributions 171, 172, 173, 176, 184 and 185. All samples included (n = 10) were single patient samples with no exogenous steroids.
Analytical methods
Total cortisol was measured by GC-MS at the WEQAS Reference Laboratory using a modified version of their GC-MS reference method. 10 The bracketed standard curve used in the reference method was replaced with a conventional six-point standard curve. Total cortisol was also measured by four automated immunoassays in four separate hospitals: Abbott Architect (Abbott Laboratories, Illinois), Beckman Access (Beckman Coulter, Brea, CA), Advia Centaur (Siemens AG, Erlangen, Germany) and the Modular Analytics E170 (Roche, Mannheim, Germany). All laboratories performing analysis were enrolled in the UK NEQAS scheme for cortisol and were performing within their method group at the time of analysis. Inter-assay coefficients of variation for quality control data around the time of analysis were 4.7%, 3.3% and 5.7% at cortisol concentrations of 107.6, 355.7 and 634.8 nmol/L for GC-MS; 10.8%, 5.8% and 4.5% at 66.5, 540.3 and 915.1 nmol/L for the Roche E170; 5.1%, 3.6% and 3.1% at 76.7, 327.7 and 720.8 nmol/L for the Abbott architect; 6.1% and 6.0% at 145.5 and 954.4 nmol/L for the Siemens Centaur and 6.7%, 5.6% and 3.9% at 119.4, 432.7 and 973.4 nmol/L for the Beckman Access, respectively.
Statistics
All statistical analysis was performed with IBM SPSS Statistics version 21. Assay-specific bias ratios were calculated by dividing the cortisol immunoassay result by the matched GC-MS result. Variance in bias relative to GC-MS across groups was compared with the Levene statistic for each assay. Due to differences in sample size and variance between groups, bias between all patient groups were compared for each method with the Kruskal–Wallis non-parametric test for independent samples. The sources of difference were determined post hoc with the Mann–Whitney U test.
Results
Patient pools
Recovery of cortisol in male and female pooled serum is shown in Figure 1. Increased inter-assay variation in cortisol recovery is seen in the female compared to the male pool. Average percentage recovery of cortisol in female and male serum was 126% and 109% for Roche E170, 87% and 110% for Abbott architect, 106% and 100% for Siemens Centaur and 93% and 99% for Beckman Access cortisol immunoassays, respectively. When actual measurements were compared to GC-MS, the closest agreement with GC-MS was found for the male pool using the Beckman Access immunoassay and the largest (positive) bias observed for the male pool using the Roche E170 method.
Percentage recovery of cortisol spiked into pools of (a) male and (b) female serum. ♦: GC-MS; ▪: Roche E170; ▴: Abbott architect; □: Siemens centaur; ○: Beckman access. Recoveries are calculated relative to cortisol measured in unspiked pool, as determined by each assay.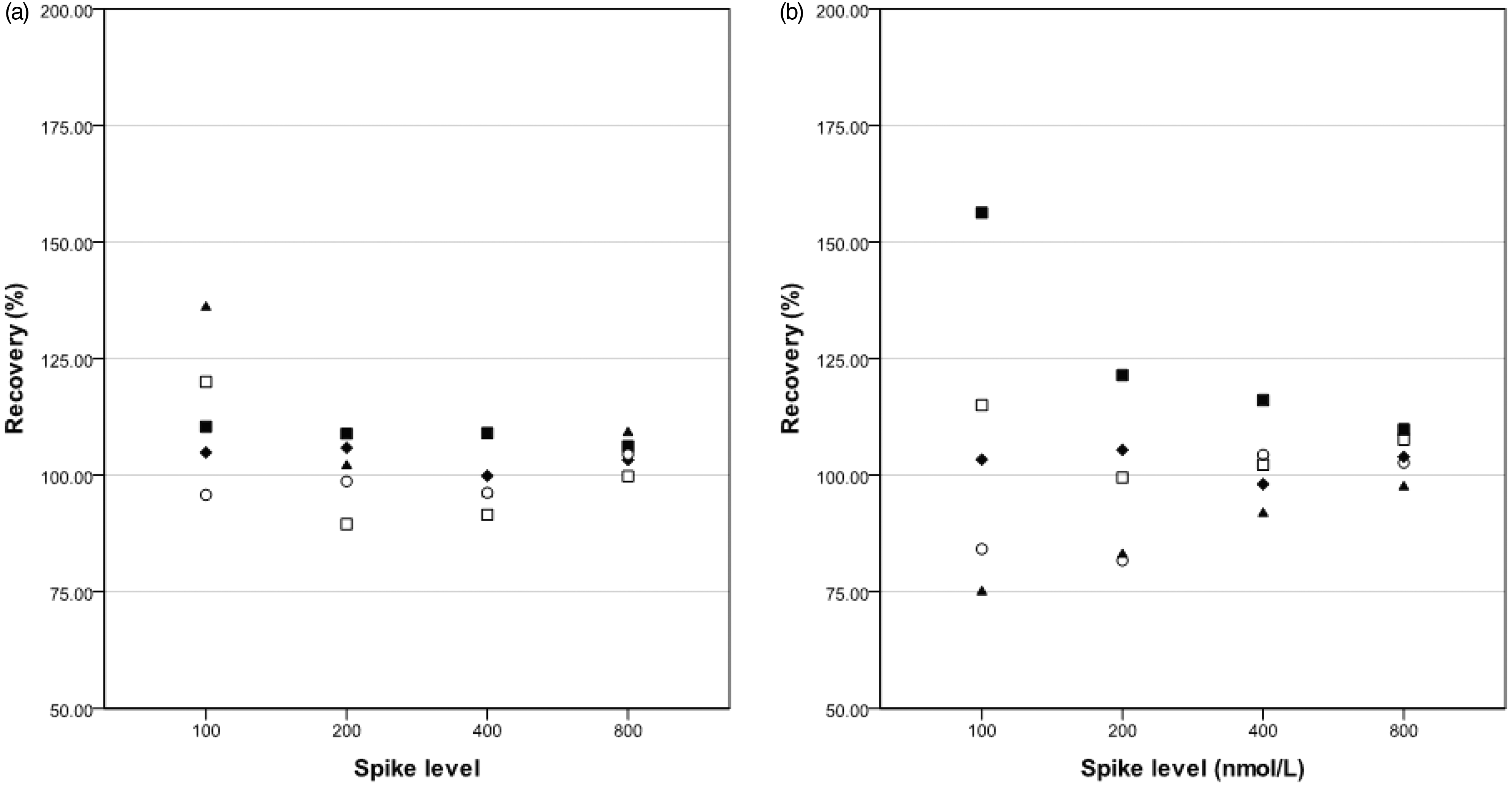
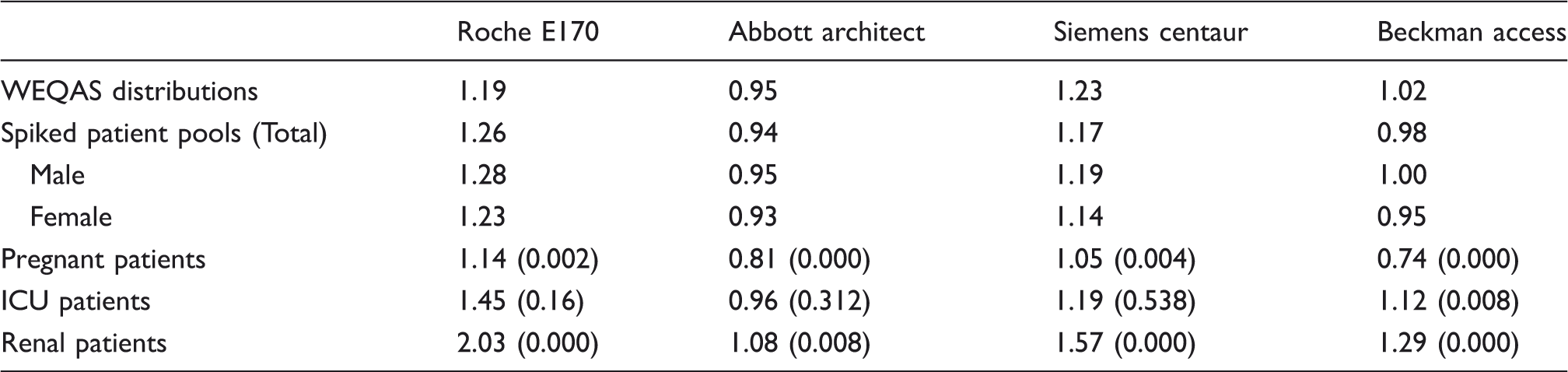
Mean bias ratios for cortisol immunoassays compared to GC-MS in different patient groups.
Patient serum samples
Differences in cortisol assay bias compared to GC-MS across the groups studied are shown in Figure 2 and Table 1. Pregnancy serum samples all showed a greater negative bias for all assays compared to pooled serum (Figure 2). This was particularly marked for the Beckman Access, which had either no bias or a slight positive bias in all groups except pregnancy, where a strong negative bias was seen. This bias in pregnant patients appeared to be greater at higher concentrations of cortisol for all assays except the Roche E170, which had a relatively constant bias (Figure 3).
Box and whisker plots of bias between immunoassay and GC-MS showing marked effect due to the clinical source of patients’ samples. Each plot shows a different assay: (a) Roche E170, (b) Abbott architect, (c) Siemens centaur and (d) Beckman access. Minor and major outliers as determined by SPSS displayed by ○ and *, respectively. One renal outlier for both (a) and (c) are not shown on plot for clarity (indicated by arrow, 389% for (a) and 456% for (c)). Difference plots (Bland–Altman) for (a) Roche E170, (b) Abbott architect, (c) Siemens centaur and (d) Beckman access versus GC-MS cortisol concentrations. ▪: spiked pools; ▴: second trimester of pregnancy; x: intensive care unit; ○: patients with end-stage renal disease. One intensive care patient not shown on plots for clarity (GC-MS 2379 nmol/L: Roche E170 +581 nmol/L, Abbott architect −672 nmol/L, Siemens centaur −469 nmol/L and Beckman access −389 nmol/L).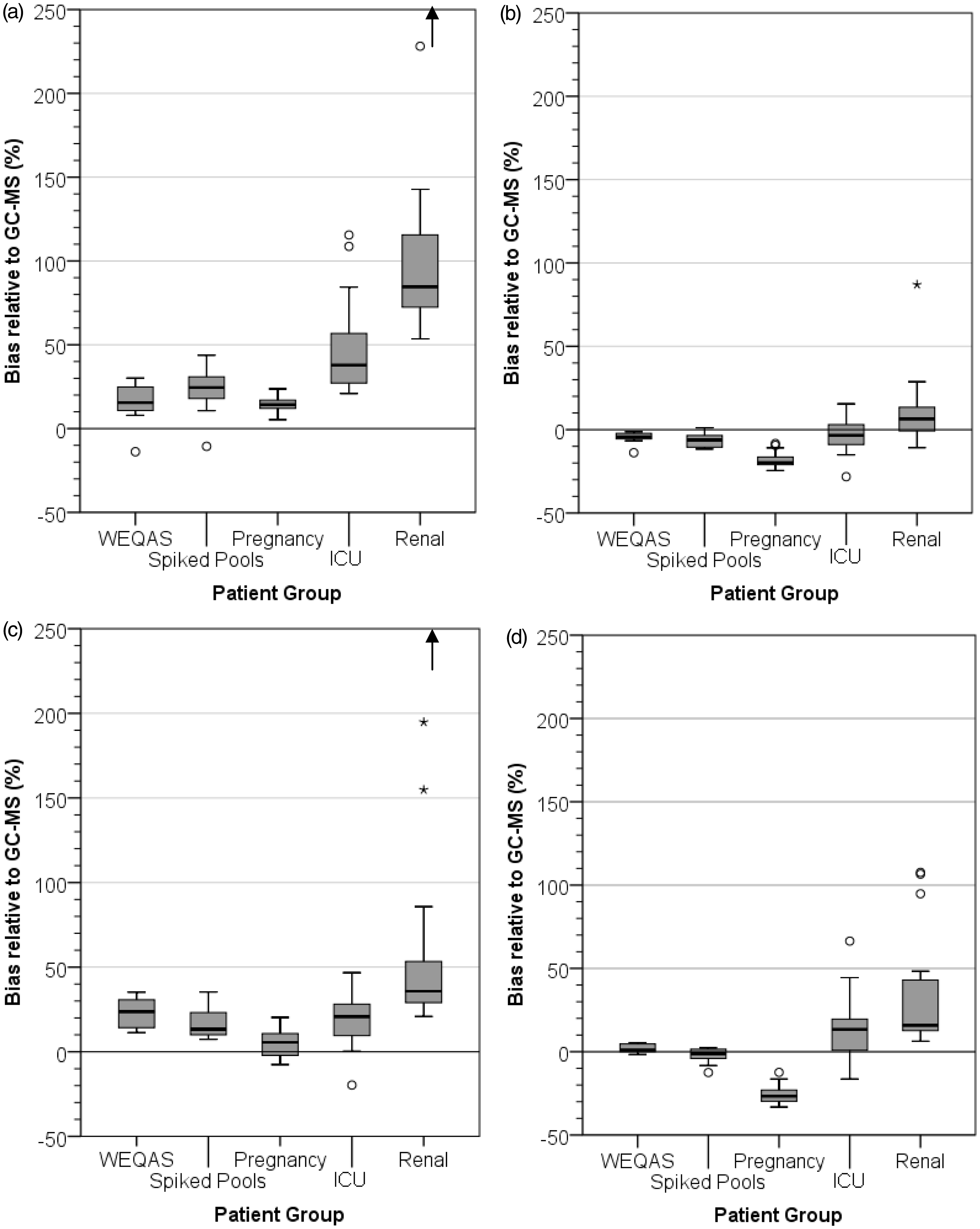
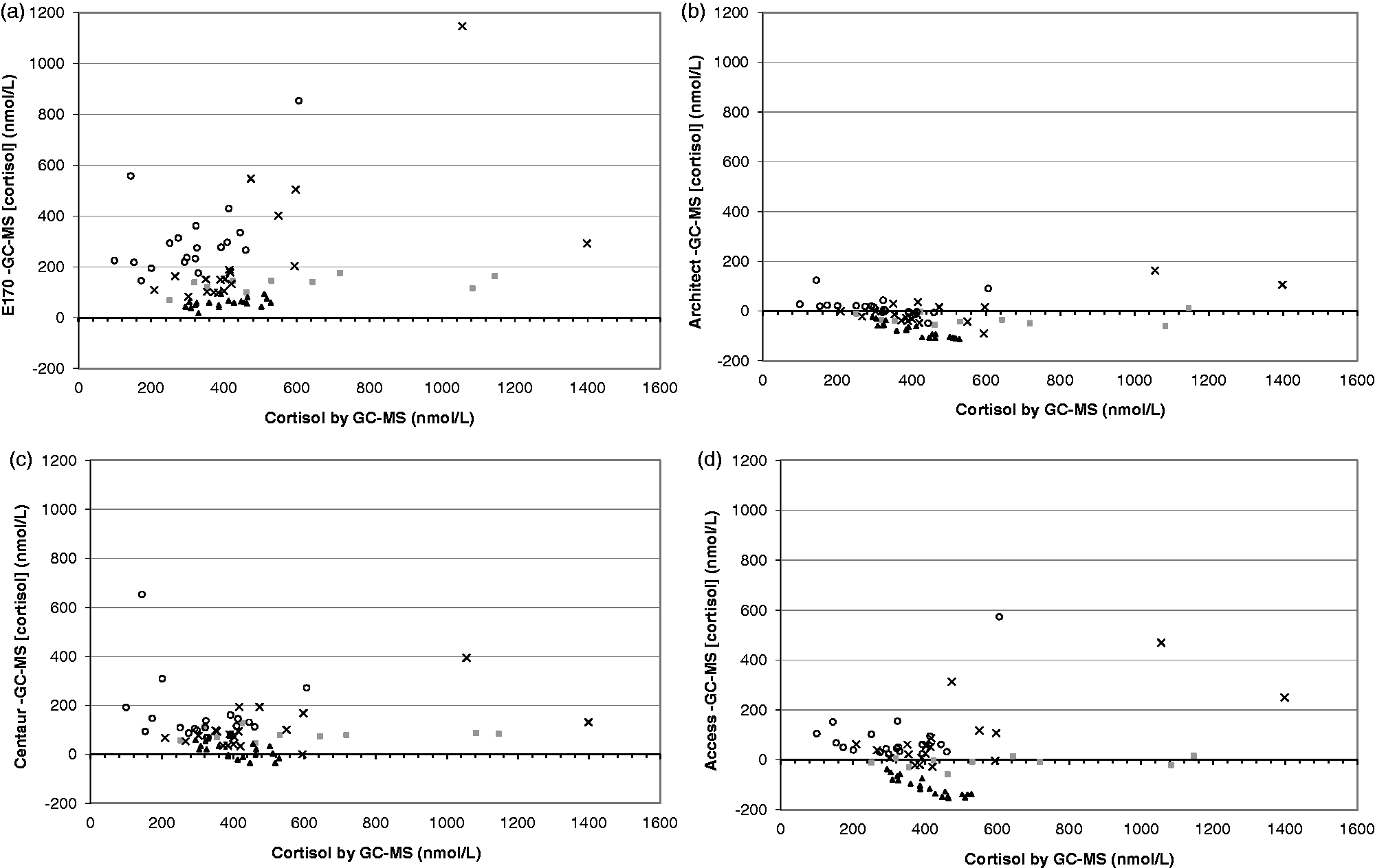
Variation in bias was greatest in serum from patients with end-stage renal disease, and to a lesser degree in the ICU patient serum, than in the relatively healthy patient groups (patient pools and pregnancy; also WEQAS distributions) for all assays (Figure 2). The proportional bias did not show a clear trend at different concentrations of cortisol for either ICU or renal patients (Figure 3). In general, assays over-recovered in these patient groups relative to GC-MS; the least affected by this was the Abbott architect, and the most affected was the Roche E170, although all assays appeared to show more variation, and greater positive bias, in renal patients compared to the pools or pregnant patients. Post hoc Mann–Whitney statistics did not indicate a significant difference in bias between the spiked pools and ICU groups for the Roche E170, Abbott architect and Siemens Centaur (p = 0.16, 0.31, 0.54, respectively).
Discussion
There is increasing recognition that interpretation of cortisol measurements requires knowledge of the assay bias4–6 and for some immunoassays there will be significant gender effects to consider as well.3–5 This study and others4–8 clearly demonstrate that physiological and pathological conditions which affect serum matrix can have an effect on cortisol assay bias. For all immunoassays studied, cortisol bias compared to the gold standard GC-MS was more negative in pregnant individuals than in non-pregnant healthy volunteers or pooled normal female serum. Previous studies4,6 have demonstrated a similar trend in the serum of women taking the OCP pill compared to other female volunteers. In pregnancy and women taking the OCP, this is likely to be an effect of increased concentrations of cortisol binding globulin (CBG). Cortisol immunoassays measure total cortisol (free cortisol and cortisol bound to CBG and albumin). To do this, the assay manufacturers must include a step to displace cortisol from its binding proteins. In most cases, this is commercially sensitive and not included in the assay information available for customers. Use of another steroid, a change in pH9 or use of a high affinity antibody to compete for binding is a speculative approach. Our results, however, may suggest that when CBG is increased the methods in use are not totally efficient. We speculate that the negative bias compared to normal female serum is due to some cortisol remaining CBG bound. Where cortisol binding proteins are decreased, e.g. in the hypoalbuminaemic ICU subjects included in this study this will result in a decrease in bound cortisol. This may also affect the efficiency of any cortisol displacement step included in the assay.
We have observed increased intermethod variation in the serum from both renal and ICU patients, compared to pooled serum samples. This is most significant for the Roche E170 method. We speculate that this is a function of the specificity of this immunoassay. During critical illness, cortisol production is increased, and cortisol breakdown is also reduced as a consequence of suppressed expression and activity of cortisol metabolizing enzymes. 11 Decreased clearance also occurs in patients with renal impairment. These changes in cortisol metabolism may lead to an accumulation of other steroids, which because of the similarities to the structure of cortisol are recognized by the immunoassay. Others have also observed differences in bias of the Roche E170 assay compared to GC-MS in the serum of sepsis patients compared to patients routinely attending outpatients. 7 Increased ‘apparent’ cortisol measurement has also been reported in patients with congenital adrenal hyperplasia using the Roche E170 method 12 which was attributed to recognition of other steroids which are increased in the serum of patients with this condition.
Comparison of cortisol immunoassay bias against GC-MS in this study compared to previous work 4 and cortisol spiking studies reported annually by UKNEQAS over time1,13 demonstrates that immunoassay bias is not constant over long periods. Laboratories will be familiar with changes in assay bias between lots of immunoassay reagents or following assay reformulations by the manufacturer. But clinicians may not be cognisant to this fact. Where specific cut-offs are used for interpretation of results, e.g. the short Synacthen test, this becomes a significant factor to consider.
Owen et al. 14 have recently described development of a cortisol assay suitable for clinical use using tandem mass spectrometry. This method offers improved specificity over immunoassays and overcomes the limitations reported here for immunoassays. However, tandem mass spectrometry technology is still relatively new to clinical biochemistry and for the time being is less robust than automated immunoassay. Accordingly, the use of tandem mass spectrometry is likely to be limited to laboratories with specialist expertise in this technology. Whilst the use of immunoassay to measure cortisol predominates, it is important that laboratories and clinicians interpreting cortisol results are aware that serum matrix as well as assay bias and gender must be considered. Specific knowledge concerning the behaviour of the cortisol immunoassay used by the laboratory is essential, as it is clear that for some immunoassays there is a significant difference between true and ‘apparent’ measured cortisol in some clinical settings.
Footnotes
Acknowledgements
The authors thank staff at WEQAS and Department of Medical Biochemistry and Immunology, University Hospital of Wales, for their assistance.
Declaration of conflicting interests
None.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
This study was approved as a service evaluation project by Cardiff and Vale University Health Board.
Guarantor
CE.
Contributorship
CE, NE-F and DAR conceived the study. AJD undertook laboratory studies with assistance from DHD and SMN. AJD analysed the data. KLM, AA and JHB supervised analysis in their laboratories, AJD and CE wrote the first draft of the manuscript. All authors contributed to the analysis and interpretation of data, drafting and revising the manuscript and approval of the final version.