
Abstract
Background
A research on novel cardiovascular risk factors is mainly focused on patients with clinically verified coronary artery disease (CAD), while less is known about their presence in symptomatic patients, but without angiographically proven occlusion of coronary arteries. The aim of this study was to compare plasma low-density lipoprotein (LDL) and high-density lipoprotein (HDL) size and subclasses in stable angina patients with and without significant obstructive CAD.
Methods
LDL and HDL subclasses were analysed in 100 stable angina patients with ≥50% of obstruction and 40 patients with less than 50% of luminal narrowing, as assessed by coronary angiography.
Results
Patients with <50% of obstruction had reduced mean HDL size and higher proportion of small HDL particles (P < 0.05). HDL size and proportion of small HDL particles were significant and independent predictors of obstructive CAD (P < 0.05, respectively).
Conclusions
Stable angina patients with <50% of coronary obstruction have more favourable HDL subclasses distribution than patients with significant coronary stenosis.
Introduction
Majority of studies on novel cardiovascular risk factors have been focused on patients with clinically significant coronary artery disease (CAD). Less is known about the presence and interrelationship of risk factors in symptomatic patients, but without angiographic evidences of significant coronary occlusion. 1 Screening for the presence of small, dense low-density lipoprotein (LDL) and high-density lipoprotein (HDL) particles and identification of factors which affect their excessive production could have beneficial effects on reducing the risk for future cardiovascular events. 2 Yet, clinical significance of LDL and HDL particles heterogeneity in patients with stable angina, but without coronary occlusion remains to be established.
The aim of this study was to compare plasma LDL and HDL size and subclasses in stable angina patients with and without angiographically verified coronary obstruction. In addition, we sought to examine whether potential differences in lipoprotein subclasses distributions could be related to the progression of the disease.
Patients and methods
This study included 140 patients with stable angina pectoris referred for elective coronary angiography at the Institute of Cardiovascular Diseases, Clinical Centre of Serbia in Belgrade. Stable angina was defined by its clinical presentation of chest pain or discomfort that typically occurs with activity or emotional stress and relieves by organic nitrates administration or rest. Exclusion criteria were acute myocardial infarction within three months prior to analyses, presence of infection, diabetes, renal and hepatic disorders, or use of lipid-lowering drugs. Two experienced cardiologists, unaware of patients’ clinical history and biochemical results visually reviewed all angiographic images to assess the extent of CAD. Significant lesions with ≥50% of luminal narrowing were found in 100 patients, while rest of 40 patients had less of 50% of obstruction. Informed consent was obtained from each participant. The study was executed according to the Helsinki Declaration and approved by the institutional review committee (Reference No. 2251/1).
Plasma LDL and HDL subclasses profiles were assessed using a method of polyacrylamide gradient gel electrophoresis. 3 Estimated diameter of the major peak in the LDL and HDL regions of densitometric scan was referred to as LDL and HDL particle size and relative content of each subclass was estimated by determining the areas under the peaks. The inter-assay coefficients of variations (CV) for LDL and HDL sizes were 1.8–2.2% and the method was highly correlated with the original procedure (Y-intercept: 1.14 ± 0.76, slope: 0.96 ± 0.03, r2 = 0.992). 3 Apolipoprotein E (apoE) phenotyping was performed by isoelectric focusing of delipidated serum followed by immunobloting. Visceral adiposity index (VAI) was calculated as previously proposed. 4 Concentrations of other analysed parameters were assayed by routine laboratory methods.
Continuous variables are presented as mean and standard deviations and analysed by the Student’s t test; or as median and interquartile range and analysed by the Mann–Whitney U test. Categorical variables are presented as relative frequencies and compared by the Chi-square test. Univariate and multivariate logistic regression analysis were used to examine the associations of HDL size and relative proportion of small HDL particles with obstructive CAD. Differences with P < 0.05 were considered to be statistically significant.
Results
Clinical and laboratory characteristics of study participants according to the results of coronary angiography.
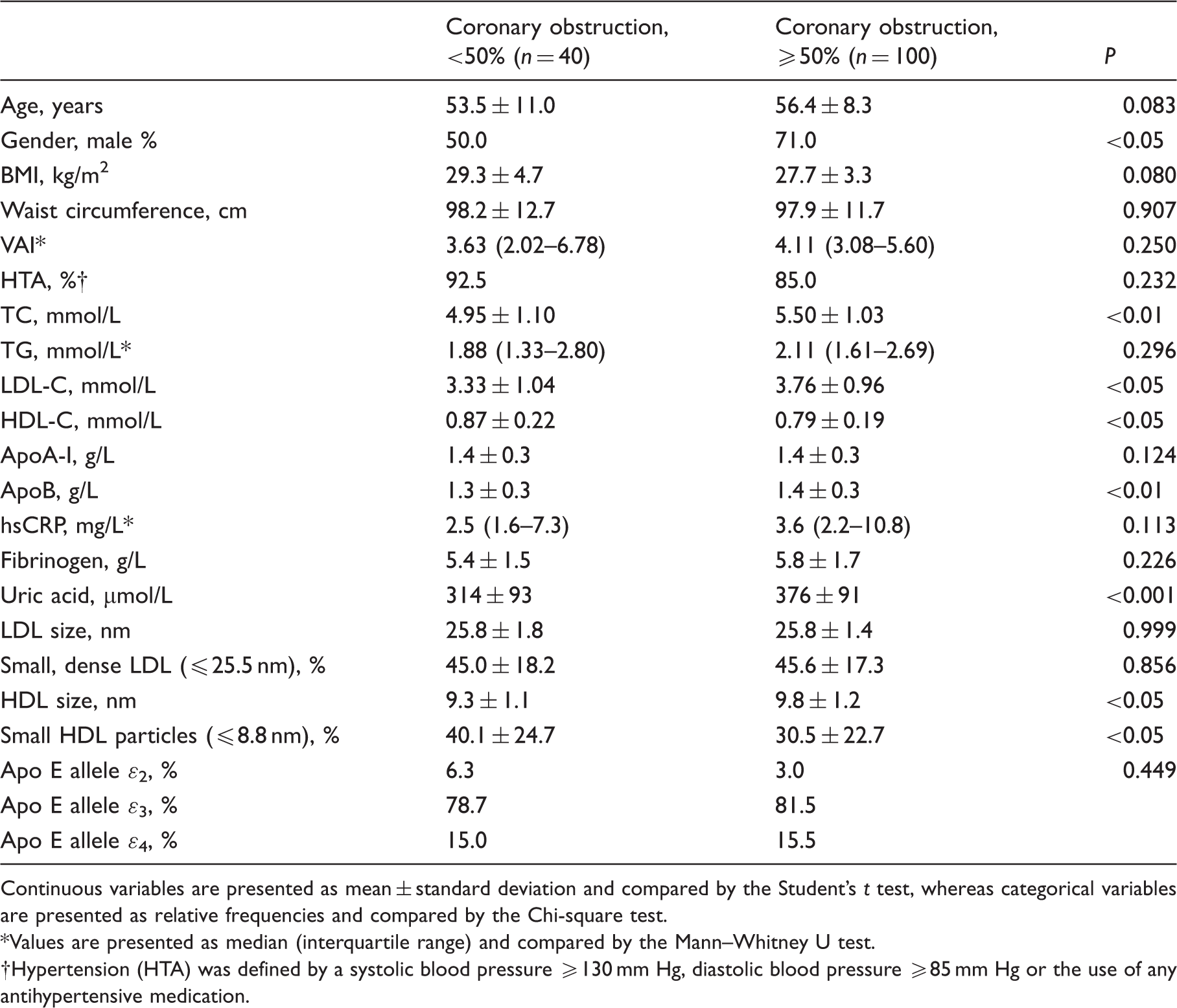
Continuous variables are presented as mean ± standard deviation and compared by the Student’s t test, whereas categorical variables are presented as relative frequencies and compared by the Chi-square test.
Values are presented as median (interquartile range) and compared by the Mann–Whitney U test.
Hypertension (HTA) was defined by a systolic blood pressure ≥130 mm Hg, diastolic blood pressure ≥85 mm Hg or the use of any antihypertensive medication.
Further analysis was focused on patients with HDL size ≤8.8 nm (16 patients with <50% and 23 patients with ≥50% of coronary obstruction). Even though both newly formed groups were homogenous by age, gender, BMI and waist circumference (data not shown), patients with ≥50% of coronary occlusion had greater VAI [5.27 (3.40–9.65) vs. 4.17 (2.15–6.09); P < 0.05] and TG [2.60 (1.94–3.12) vs. 1.86 (1.34–2.50) mmol/L; P < 0.05], while lower HDL-C [0.72 ± 0.16 vs. 0.87 ± 0.22 mmol/L; P < 0.05] and apoA-I [1.3 ± 0.2 vs. 1.5 ± 0.2 g/L; P < 0.01] levels. In occlusive CAD group, distribution of LDL subclasses was shifted in favour of small, dense particles (≤25.5 nm), due to the reduction in relative proportion of LDL I [38.2 ± 14.6 vs. 50.8 ± 11.0%; P < 0.01] and increase of LDL IV [25.9 ± 11.3 vs. 17.1 ± 8.1%; P < 0.01] subclasses.
Logistic regression analysis for associations of HDL size and relative proportion of small HDL particles with obstructive CAD.
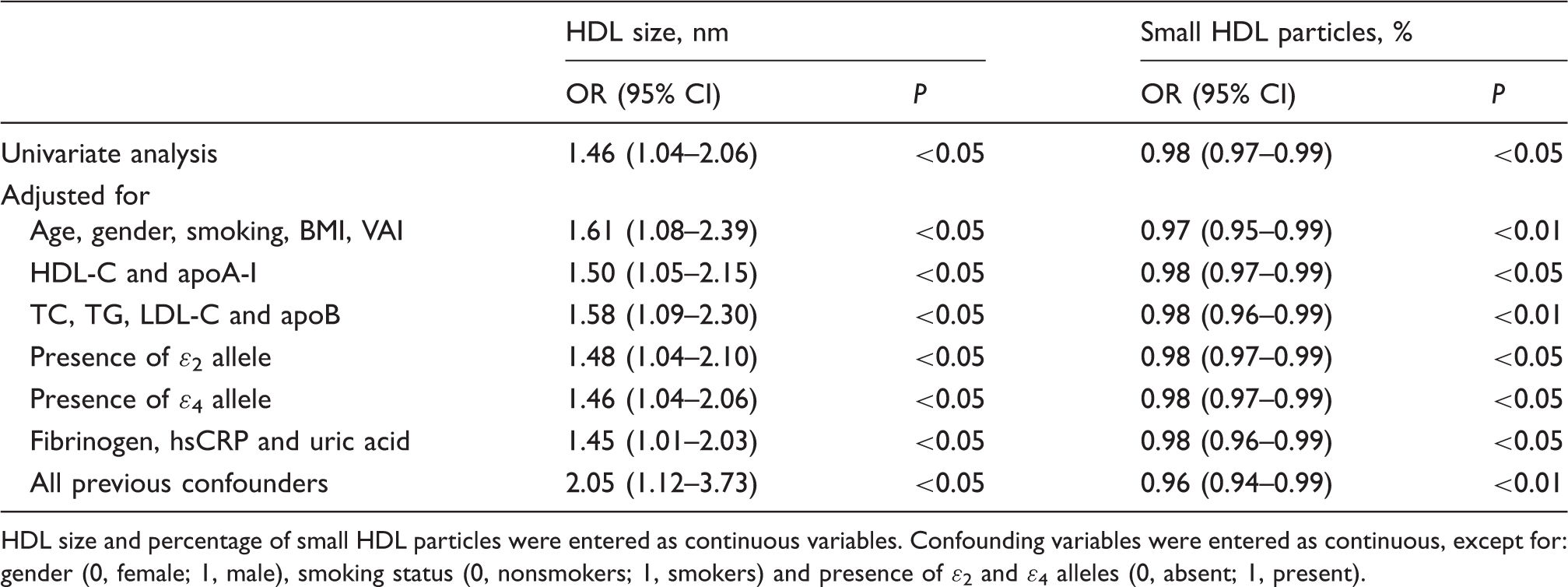
HDL size and percentage of small HDL particles were entered as continuous variables. Confounding variables were entered as continuous, except for: gender (0, female; 1, male), smoking status (0, nonsmokers; 1, smokers) and presence of ɛ2 and ɛ4 alleles (0, absent; 1, present).
Discussion
In the present study we have demonstrated that stable angina patients without angiographically documented coronary occlusion have different HDL particles distribution than the patients with significant luminal narrowing.
Alber et al. 1 reported that HDL-C was independently associated with prevalence and severity of CAD. It is now appreciated that plasma HDL-C level cannot reflect HDL particles diversity or capture their functional variations. 5 Accordingly, it has been postulated that small HDLs generally have stronger cardioprotective properties than their larger counterparts. 5 Our findings of higher HDL-C, reduced HDL size and increased prevalence of small HDL particles in the group with <50% of coronary obstruction (Table 1) are in agreement with this explanation. However, it has been noticed that small HDL particles can be highly vulnerable to possible detrimental effects of dyslipidemia, enhanced oxidative stress and inflammation, which could decrease their anti-atherogenic capacity. 5 In the current study, smaller HDL size was accompanied with significantly higher TG and VAI in patients with significant stenosis. Therefore, we could speculate that prominent hypertriglyceridemia and possible insulin resistance in this category of patients could compromise HDL’s atheroprotective function. Such particles are likely to have diminished ability to prevent lipid accumulation and formation of plaque, 5 which could be partly reflected as enhanced proportion of small, dense LDL particles in these patients. Indeed, smaller HDL size and a preponderance of small particles were associated with reduced risk for severe luminal narrowing and consequently, obstructive CAD development (Table 2). Observed independent associations suggest the existence of intrinsic mechanisms through which HDL particles per se contribute to preservation of normal arterial lumen, regardless of other cardiovascular risk factors.
Relatively small sample size might restrict a reliability of our conclusions. Also, we could not explore a causal relationship between HDL particles distribution and progression of luminal stenosis in later life. Future prospective studies are needed to evaluate presented observations.
In conclusion, our results demonstrated differences in HDL subclasses distribution in stable angina patients with and without angiographically verified obstructive CAD, with a shift towards smaller particles in the non-obstructive group. Our results indicate that the observed difference might be accounted for reduced risk of CAD progression towards obstructive disease.
Footnotes
Acknowledgements
The authors express appreciation to the patients who participated in this study and stuff at Clinic for Cardiovascular Diseases, Clinical Centre of Serbia for help in obtaining and processing samples.
Declaration of conflicting interests
None of the authors have any competing interests.
Funding
This work was supported by a grant from the Ministry of Education, Science and Technological Development, Republic of Serbia (Project No. 175035) and by the European Cooperation in Science and Technology (COST) BM0904 Action.
Ethical approval
The ethics committee of Faculty of Pharmacy, University of Belgrade approved this study (Ethical approval number 2251/1).
Guarantor
AZ.
Contributorship
VSK, ZJI and SS conceived and designed the study. DKO and LM were involved in protocol development, patient recruitment and data acquisition. AZ and JV performed analysis of lipoprotein subclasses and wrote the first draft of the manuscript. VSK and ZJI edited the manuscript. AT and VSK performed apoE phenotyping. NBS and SS participated in statistical data analysis.