
Abstract
Background
A single bout of strenuous running exercise results in perturbations to numerous biomarkers. An understanding of these is important when analysing samples from individuals who have recently performed such exercise.
Methods
A literature search was undertaken using the search terms, exercise, marathon and delayed onset of muscle soreness. The search was then refined using the terms for key biomarkers known to be altered by exercise.
Results
The magnitude of changes to biomarkers is proportional to the severity of the running bout. Familiar, moderate intensity running exercise produces brief transient changes in common biomarkers such as lactate, whereas more severe bouts of running exercise, such as marathons and ultra-marathon events can produce changes to biomarkers that are normally associated with pathology of the muscles, liver and heart. Examples being changes to concentrations and/or activity of myoglobin, leucocytes, creatine kinase, bilirubin, cardiac troponins, lactate dehydrogenase, alanine aminotransferase and aspartate aminotransferase. While persisting for longer, these changes are also transient and full recovery occurs within days, without any apparent long-term adverse consequences. Additionally, unfamiliar exercise involving forceful eccentric muscle contractions, such as running downhill, can cause increases in creatine kinase and delayed onset of muscle soreness that peaks 36–72 h after the exercise bout.
Conclusions
Strenuous running exercise can produce changes to biomarkers that are normally associated with disease and injury, but these do not necessarily reflect chronic pathology.
Introduction
During a bout of running exercise, numerous acute transient responses occur to enable the body to cope with the metabolic and physiological demands of the exercise currently being undertaken. These include increases in the rate and depth of breathing, cardiac output, the prioritization of blood flow to the exercising muscles and changes to the circulating concentrations of various hormones. The magnitudes of these transient responses are proportional to the intensity of the exercise being undertaken: with light and moderate intensity exercise eliciting modest responses, while more strenuous exercise bouts elicit responses of a greater magnitude.
In addition to the aforementioned responses, prolonged strenuous running can produce changes to the concentrations and/or activity of other biomarkers that reflect the physiological stresses being encountered during the exercise bout. Indeed, very severe bouts of exercise of an unfamiliarly high intensity or long duration have the potential to produce exceptional changes in biomarkers that are commonly associated with injury and pathology.
What determines the magnitude of the physiological stress encountered by the exerciser and the resultant acute responses is a combination of the severity of the exercise and the physiological demands of the exercise relative to the fitness of the individual. For example, running 5 km in 30 min would constitute a relatively light bout of exercise for a fit endurance runner for whom the demands of the exercise would be well within their capacity, invoke relatively moderate responses and represent little physiological stress. Whereas for a less fit individual, attempting to run 5 km in 30 min may be very close to their maximum capacity and would thereby constitute a very strenuous exercise bout that elicited maximal responses and placed more substantial physical stress on their body. The practical and clinical implications of this are that the same bout of exercise may produce very different magnitudes of responses and changes to various biomarkers in individuals of differing levels of fitness, and what constitutes severe or strenuous exercise will differ from one person to another. This means that for an unfit individual, changes to some biomarkers may be evident after lesser bouts of running exercise, whereas for a regular, well-trained runner, the elevation of biomarkers associated with injury or pathology are only likely to be evident following more severe bouts of exercise, such as running a marathon (42.2 km) or undertaking events of an even longer duration such as iron-man triathlons (3.86 km swim, 180.25 km bicycle ride and 42.2 km run) or ultra-distance races lasting many hours or days. However, since well-trained endurance athletes exhibit an enhanced metabolic capacity (VO2 max), augmented capacity to secrete certain hormones, and are capable of and more likely to undertake more severe and more prolonged bouts of exercise, it is possible that the changes to some biomarkers may be greater in athletes when undertaking extreme exercise scenarios than in non-athletes completing lesser exercise bouts. Hence, when recording the recent history of an individual in the context of interpreting clinical data, simply recording the fact that they had recently exercised may not provide adequate information, whereas recording its type, intensity, duration, and whether it was something that they undertook on a regular basis or was unfamiliar or more severe than usual would provide a fuller context in which to interpret the results.
The aim of this review is therefore to identify the acute and transient exercise-induced changes to biomarkers that occur during and/or following strenuous running exercise. It will commence with a brief overview of acute changes to plasma volume, electrolytes, catecholamines and other hormones, glucose, lactate and lipids. It will then proceed to consider changes to biomarkers that are more commonly associated with injury and pathology, and may be evident following extreme and/or unfamiliar bouts of running, but may or may not indicate injury or other pathology. It will also consider the acute changes that are associated with an acute risk of a cardiac event either during or immediately following an exercise bout. Some examples from multi-day events are included in the review, since while it is acknowledged that by the end of such events the observed changes in biomarkers are likely to reflect a combination of both acute responses to that day’s exercise and adaptations to exercise completed in the previous days of the event; the reported changes are an indication of the transient consequences of unfamiliarly strenuous exercise rather than being a representation of the athlete’s ‘rested’ state or normal training condition. It is not intended for this review to cover the more publicized long-term chronic adaptations to exercise and its specific health benefits, as these comprise the long-term adaptations to repeated bouts of exercise and are extensively reviewed elsewhere.1,2 The review also primarily focuses on running, since while there are studies on cyclists, it would appear that the repetitive impact of the foot striking the ground when running results in additional stresses that are not evident in comparable cycling events. Issues concerning the collection, storage, preparation and analyses of biological samples from which the discussed biomarkers are measured are reviewed elsewhere, along with advice on ensuring the validity, reliability and comparability of results. 3
Changes to: plasma volume, electrolytes, catecholamines and other hormones, glucose, lactate, lipids and haematology
Plasma volume
A bout of strenuous exercise has the potential to induce both rapid short-term and long-term changes to plasma volume, with these changes affecting haematocrit, blood viscosity and the concentration of circulating biomarkers. Short-term responses include a fluid shift out of the intravascular space (haemoconcentration) that may be evident for several hours post-exercise. The reduction in plasma volume will also be affected by the balance between fluid absorbed from ingested drinks and fluid lost through sweating. Sweating rates are affected by: (i) the intensity and duration of the exercise, and hence the amount of metabolic heat generated, and (ii) the capacity to lose excess heat via other processes. For example, sweating rates will be greater on hot days when heat loss via radiation, conduction and convection are minimal, and as a consequence, heat loss via the evaporation of sweat provides the only effective means by which heat can be lost to the environment. As a result, dehydration is more likely to occur within a bout of exercise, undertaken in warm environments when rates of sweating can reach 1–3 L/h and exceed the rate of fluid replenishment. 4 However, in most circumstances, appropriate fluid replenishment will ensure that this can be almost entirely restored within an hour. 5 The risk of dehydration is exacerbated if the environment is humid, since this curtails evaporation rates, and given that it is the evaporative process that cools the body, rather than the process of sweating per se, sweating rates will be higher in humid conditions to compensate for the poor rates of evaporation. Hence, there is a risk of dehydration in more moderate temperatures if the humidity is high. In the context of marathon running, studies have reported that immediately post-marathon, plasma volume may be reduced from pre-marathon volumes by 12.1% (25–75 percentile range = 14.3–2.9%). 5 Likewise at the end of a 100-km ultra-marathon, plasma volumes were reported to be reduced by (mean ± SEM) 3.2 ± 0.3% of pre-race volumes. 6
Following a strenuous exercise bout, there may be an increase in plasma volume that results in a haemodilution (autohaemodilution) as the plasma volume increases to above the initial pre-exercise values.7–9 One study reported that, 22 h post-marathon, plasma volume was greater by a mean of + 10.6% (25–75 percentile range = +7.1 to +11.5%). 5 During even longer events such as a multi-day 1600-km footrace, plasma volume has also been reported to increase above pre-event volumes by (mean ± SD) +13.4 ± 4.3% on day 4; +21.6 ± 19.2% on day 11 and +12.6 ± 9.8% post-race. 10
Electrolytes
Electrolyte homeostasis is well maintained during moderate bouts of exercise and is unlikely to be altered significantly unless the exercise bout is repeated in a warm environment on frequent occasions without adequate replenishment. However, during prolonged bouts of exercise, it is possible for individuals to consume excessive amounts of water as they endeavour to maintain their hydration status, and as a consequence become hyponatremic. This is uncommon in events such as marathons, where sodium concentrations appear to be well maintained: mean = 143 mmol/L (range 137–147 mmol/L) immediately post-marathon, 11 and even in iron-man triathlons, it appears uncommon with few participants (0.6%) recording serum sodium concentrations below 135 mmol/L. 12 Unsurprisingly, hyponatremia does appear to be more prevalent in longer events such as triple iron-man triathlons (11.4 km swim, 540 km cycle and 126.6 km run), with one such study reporting that 26% of the competitors had developed exercise-associated hyponatremia (plasma [Na+] between 129 and 134 mmol/L). 13 However, it does not appear to be inevitable as other studies have reported virtually no change in the electrolyte concentrations of eight of the nine runners in a 1600 km multi-day race lasting approximately 16 days. 10 In this event, serum sodium concentrations were (mean ± SD): 141 ± 4 mmol/L on day 4; 137 ± 3 mmol/L on day 11 and 141 ± 2 mmol/L post-race. Similarly, a relatively low prevalence of hyponatremia (serum [Na+] 130–134 mmol/L) was recorded in 4% of participants in an ultra-endurance mountain running race, yet somewhat confoundingly hypernatremia (serum [Na+] 146–148 mmol/L) was reported in 3% of subjects, and such findings indicate the need for further research. 14 Changes to potassium concentrations are less commonly reported and do not appear to be substantially altered by most exercise bouts, including marathons. 11
Catecholamines and other hormones
A bout of exercise has the potential to alter the circulating concentrations of many hormones. Some hormones display rapid responses upon the onset of the exercise, while others exhibit delayed responses that are dependent upon the exercise exceeding a duration threshold. 15 The catecholamines adrenaline and noradrenaline are examples of hormones that display a rapid response that is in proportion to the exercise intensity. Low-intensity exercise produces little or no increase, while strenuous exercise intensities can increase plasma adrenaline from pre-exercise concentrations of around 400–800 pmol/L to >3500 pmol/L post-exercise, and noradrenaline from pre-exercise concentrations of around 1700–2800 pmol/L to >20,000 pmol/L post-exercise.16,17 These increases facilitate the body’s capacity to respond to the demands of the exercise by promoting cardiac output and the delivery of fuel substrates to the muscle, including the promotion of glucose release from the liver, and trained athletes have a greater capacity to secrete adrenaline than untrained individuals. 15 However, since catecholamines have a short half-life, circulating concentrations normally return to close to resting concentrations within 5–10 min of exercise cessation and are not likely therefore to be substantially elevated in samples taken after this time. 16
Numerous other hormones display acute changes as a consequence of a bout of exercise, the details of which can be found in the review by Viru. 15 In summary, they include: cortisol, which increases during or after high intensity short-duration exercise, and during exercise of a lesser intensity if it exceeds 2–3 h; ß-endorphin, which displays similar responses to cortisol; testosterone, which has been reported to increase with high-intensity exercise, but may decrease if the exercise is very prolonged; insulin, which decreases during exercise (with the uptake of blood glucose into the muscle continuing through non-insulin dependent processes) but increases post-exercise to facilitate muscle glycogen replenishment and training adaptations; progesterone, estradiol and thyroid hormones, for which the results are variable and equivocal; and anti-diuretic hormone and the rennin-angiotensin-aldosterone complex, the responses of which are dependent upon the fluid and electrolyte status of the body during the exercise bout.
Glucose
During most exercise scenarios of a moderate exercise intensity, healthy individuals maintain their blood glucose concentrations at around 4.5–5.0 mmol/L. This is achieved through the precise balance between the rate of glucose appearance in the blood from the liver and digestive tract (Ra), and its peripheral uptake or disappearance by insulin-dependent tissues (predominantly skeletal muscle) (Rd). 18 However, during exercise of a relatively high intensity, blood glucose concentrations can become slightly elevated, and conversely if the exercise is very prolonged, glucose concentration may decline to below resting concentrations, the reasons for which are described below.
The relative contribution of fuel sources (fats and carbohydrates in the form of glucose and glycogen) during a bout of exercise is primarily determined by the exercise intensity. Low-intensity exercise such as walking has a greater reliance upon fat as an energy source, whereas higher intensity exercise, such as running, not only elevates the overall rate of energy expenditure but also requires a greater proportion of that energy to be derived from carbohydrate sources. Continuous exercise of low to moderate intensity (30–60% VO2max) lasting up to 90 min utilizes a combination of fats and glucose, and during the exercise blood glucose usually remains within a very narrow range, rarely exceeding 6.5 mmol/L or declining to <3 mmol/L. 19 This is achieved through the blood glucose that is being taken up by the active muscle being matched by the release of glucose from the liver and/or exogenous sources such as sports drinks. However, if the exercise is more strenuous and at a greater exercise intensity, the presence of elevated concentrations of catecholamine hormones will promote the release of additional glucose from the liver, and as a consequence, blood glucose concentrations may increase to around 5–6 mmol/L. 20
Paradoxically, if the exercise is prolonged (>90 min), plasma or blood glucose concentrations can begin to decline as glucose, muscle glycogen and liver glycogen stores become depleted. In susceptible individuals, this may result in frank hypoglycaemia (a blood glucose concentration of <2.5 mmol/L). 21 Cases of hypoglycaemia are therefore more prevalent in longer duration events, and/or in situations where the individuals have been consuming a low carbohydrate diet.
Endurance training can modify the utilization of fuel sources, with endurance runners and cyclists being capable of deriving more of their energy needs from fat than untrained individuals. Hence they are able to better conserve the limited carbohydrate stores when undertaking prolonged exercise bouts and are less likely to become glycogen depleted,22,23 although this can still occur in bouts of very prolonged strenuous exercise such as marathon running.
Lactate
While the increase in blood lactate concentration is perhaps the most widely known biochemical response to an acute bout of intense exercise, elevated blood lactate concentrations are short-lived and are therefore unlikely to affect the assessment of samples being analysed in a clinical setting. At rest, lactate concentrations are typically around 0.5–1.5 mmol/L but can increase to >20 mmol/L during maximal, high-intensity exercise lasting between 5 and 10 min. Peak blood lactate concentrations occur 3–5 min post-exercise, as during this time lactate will continue to diffuse out of the muscle where it was generated and into the blood. Following this, muscle and blood lactate concentrations decline exponentially and return to close to basal (resting) concentrations within 60 min of completing the exercise bout. 24
The concentration of blood lactate during and following an exercise bout is determined by the exercise intensity, as this is the key determinant of the relative contribution of the different metabolic pathways and fuel sources. Hence the highest blood lactate concentrations are recorded after sustained high-intensity exercise involving a maximal effort over 5–10 min and not in longer duration exercise such as marathon running, which is of necessity a lower intensity (slower running speed) exercise. Indeed plasma lactate concentrations immediately post-marathon are likely to be <3 mmol/L. 25
Additionally, it is worth noting that the role of lactate as the main cause of local muscle fatigue has been questioned and largely repudiated by exercise physiologists in the last two decades. 26 However, while this is recognized, the measurement of lactate continues in exercise physiology assessments as it remains a useful indicator of fitness and reflects the underlying metabolic processes. But as indicated above, unless a blood sample was collected within an hour of an exercise bout, lactate concentrations should not be elevated above the normal resting range.
Lipids
While regular exercise has been demonstrated to produce favourable blood lipid profiles that are associated with a reduced risk of cardiovascular disease, 27 a single bout of exercise is unlikely to produce significant acute changes, 28 unless it is strenuous and prolonged (>60 min duration). 29
For example, a 3-h bout of cycling exercise has been demonstrated to increase plasma free fatty acid (FFA) concentrations from around 0.25 mmol/L at rest to approximately 1 mmol/L when no carbohydrate was ingested during the exercise and to around 0.6 mmol/L in trials that included carbohydrate ingestion. 30 Likewise, in the later stages of long duration events such as marathons, FFAs may become elevated to 1.6 ± 0.5 mmol/L 31 : a response that reflects the reliance on this fuel source as muscle glycogen stores become depleted. Accompanying the elevation of circulating FFAs is a concomitant increase in blood glycerol concentrations from around 0.1 mmol/L to 0.3–0.9 mmol/L, which reflects the increased rate of whole-body lipolysis.17,30 Following their elevation during a marathon, FFA concentrations are reported to return to baseline within a week. 31
Other reported plasma lipid changes associated with marathon running include: HDL-c being elevated from pre-marathon concentrations (mean ± SEM) of 0.77 ± 0.04 mmol/L to post-marathon concentrations of 0.84 ± 0.10 mmol/L immediately post-marathon and remaining elevated for approximately three days 31 ; and LDL-c being slightly reduced from pre-marathon concentrations of 2.5 ± 0.2 mmol/L to post-marathon concentrations of 2.3 ± 0.1 mmol/L and remaining at these reduced concentrations for three days. 31 Total cholesterol concentration has been reported to increase slightly from (mean ± SEM) 4.8 ± 0.2 mmol/L to approximately 4.9 mmol/L during a marathon but then decline to around 4.5–4.7 mmol/L for the three days after, before returning to pre-marathon concentrations within a week.31,32 Triglycerides are reported to be virtually unaltered during a marathon, with pre-marathon and immediately post-marathon concentrations being (mean ± SEM) 1.22 ± 0.05 mmol/L and 1.26 ± 0.05 mmol/L respectively, but they have been reported to decline in the subsequent day to 0.9 ± 0.09 mmol/L, returning to pre-marathon concentrations within a week31,32: ultra-endurance events elicit similar changes. 33
Exercise haemorheology, haematocrit, red blood cells, white blood cells, platelets and related haematology
Changes to lymphocytes, erythrocytes, platelets and associated haematological biomarkers.
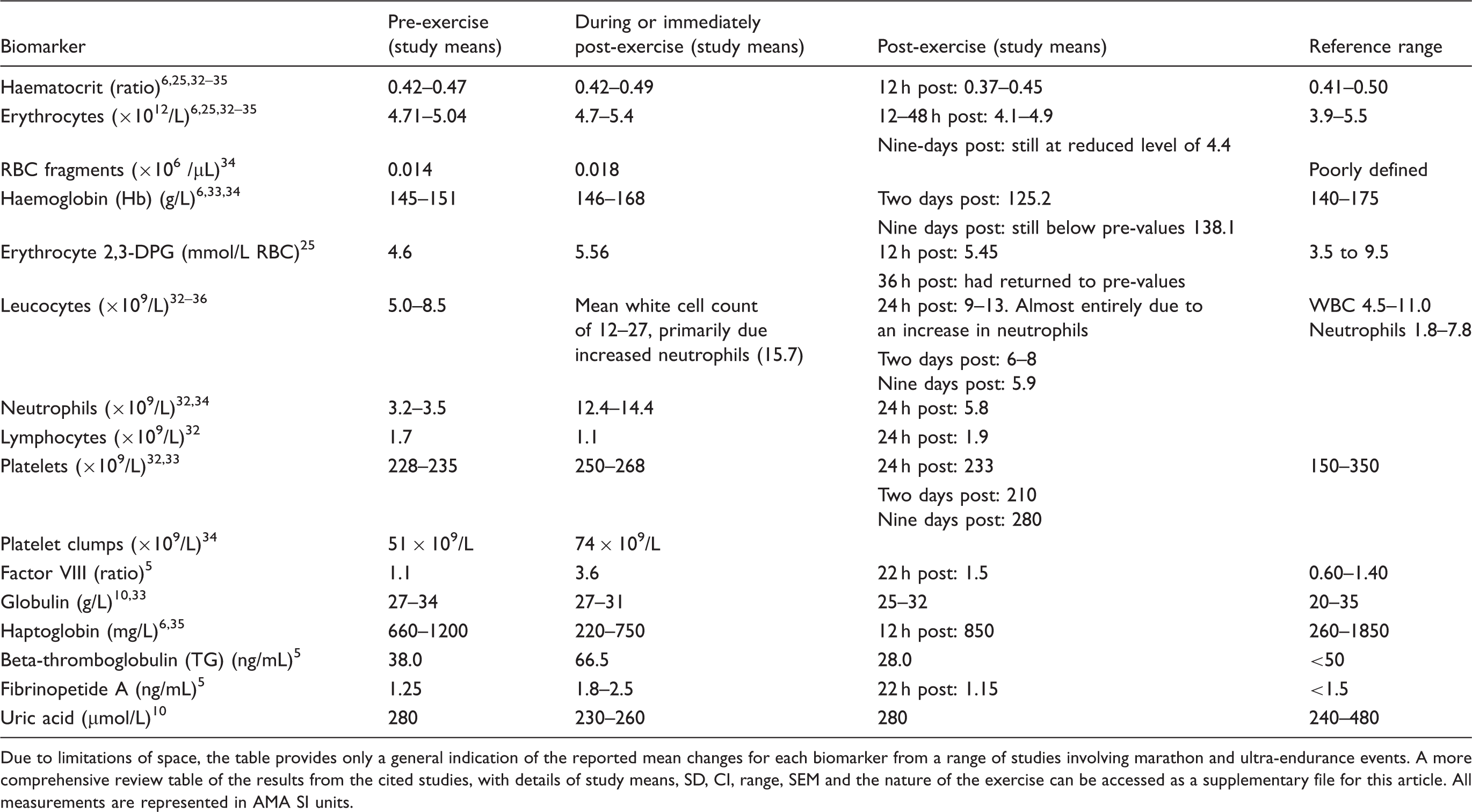
Due to limitations of space, the table provides only a general indication of the reported mean changes for each biomarker from a range of studies involving marathon and ultra-endurance events. A more comprehensive review table of the results from the cited studies, with details of study means, SD, CI, range, SEM and the nature of the exercise can be accessed as a supplementary file for this article. All measurements are represented in AMA SI units.
The acute effects of exercise upon haematocrit and blood viscosity are also unclear, with studies reporting conflicting results that may be due to differences in the mode, intensity and duration of the exercise, as well as differences in the subject population, 37 and even within an activity such as marathon running there are variable results.25,32 Where increases in blood viscosity are reported, the explanations for this acute increase include a combination of: fluid shifts; dehydration; 5–10% increases in plasma viscosity due to increased plasma proteins; the release of sequestered red blood cells (RBC) from the spleen; and decreases to the deformability and increases in the aggregation of the RBC. 37 It has been suggested that this increase in viscosity may facilitate aerobic exercise performance as it promotes nitric oxide production, which leads to vasodilation and improved oxygen delivery to the muscles. 37 By way of explaining the blood viscosity and aerobic performance paradox, it is also suggested that the lower pre-exercise blood viscosity of trained athletes ensures a greater viscosity increase upon the onset of an exercise bout, which thereby maximizes the effectiveness of the acute response. 37 So in terms of exercise haemorheology, the relationships between haematocrit, blood viscosity and performance are complex and further details can be pursued elsewhere.37,38
A specific haematological issue associated with running is foot strike haemolysis, which is when prolonged running on hard surfaces causes damage to the red blood cells and may occasionally reduce RBC concentrations either following a single prolonged bout of running or many cumulative bouts. 39 As a consequence of the destruction of RBC, there may be an associated increase in immature RBCs and reticulocytes, which can result in values outside the reference range.34,40
White blood cells and platelet counts are also reported to be elevated after prolonged strenuous exercise, such as marathon running32,36: with the authors suggesting that this may be ‘indicative of demargination of neutrophils or inflammation secondary to tissue destruction (e.g. rhabdomyolysis)’. 34 Lymphocyte concentration has been reported to double during exercise, 41 with each of the subpopulations contributing to the change. These results concur with other studies in which neutrophil concentration has been reported to double during strenuous exercise and remain elevated for at least 24 h. 42 However, if the exercise is prolonged and intense and/or repeated too frequently, the concentration can fall to below pre-exercise concentrations. This phenomenon has been frequently reported following strenuous exercise and excessive overtraining and is believed to be associated with some highly trained athletes becoming vulnerable to upper respiratory tract infections and other infectious diseases. 43
Increased platelet activation, perhaps resulting from oxidative stress and the release of catecholamines, is common immediately following a marathon event, and circulating platelet clumps have been observed. This raises concerns over the possible triggering of haemostasis in extreme bouts of exercise. 34 So, while regular physical activity produces a clear and unequivocal reduction in the long-term relative risk of cardiac events, in the acute phase (during and immediately after a bout of exercise) there is a small increase in the risk of a cardiac event. This is described as exercise’s ‘two edged sword’, 44 although on balance the chronic reductions in risk can be demonstrated to be far more substantial than the transient acute increases, which can on occasions attract considerable media coverage.
Other reported haematological and biochemical responses include those from a study on a six-day ultra-marathon event in which the following changes were observed (mean ± SD): decreased serum iron (µmol/L), from pre-race 17.3 ± 6.2 to post-race 6.0 ± 1.5; elevated serum ferritin (ng/L) from pre-race 117 ± 111 to post-race 246 ± 114; reduced percent transferrin saturation (%) from pre-race 47 ± 22 to post-race 12 ± 3; and fluctuations in serum haptoglobin (g/L) from pre-race 1.06 ± 0.21, which declined on day 1 to 0.61 ± 0.21, but became elevated after day 1 and was 2.06 ± 0.50 post-race; all of which are consistent with an acute phase response similar to that which occurs in a number of inflammatory disease states or acute tissue injury. 45 Results from a 24-h ultra-marathon also indicated elevated ferritin (mean ± SD), pre-race 64 ± 28 µg/L, increasing to 117 ± 53 µg/L immediately post-race, returning to 70 ± 45 µg/L two days post-race, but increasing again by day 9 post-race 103 ± 42 µg/L. 33 Likewise, percentage transferrin saturation fluctuated from 17.7 ± 8.0 pre-race to 31.1 ± 13.3 immediately post-race, 19.3 ± 11.6 2 days post-race and 29.2 ± 11.7 9 days post-race. 33
Cytokines and C-reactive protein
Other inflammatory markers, such as commonly measured cytokines, have also been shown to dramatically increase during and after strenuous exercise, notably Interleukin-6 (IL-6) which can be elevated 20-fold and even as high as 100-fold in the plasma to around 110 pg/mL.41,46,47 The precise role of IL-6 remains uncertain, although it has been suggested to be anti-inflammatory. 46 Other inflammatory cytokines such as IL-1β and tumour necrosis factor-α (TNF-α) may also be elevated for several days following strenuous prolonged exercise.41,47 However, chronic adaptations to exercise training appear to suppress TNF-α elevation, which may be a factor in the health benefits of regular physical activity. 46
C-reactive protein (CRP) has been reported to be elevated after: a marathon 48 ; 160-km triathlon when pre-race 14 ± 7 mg/L concentrations were unaltered immediately post-race, but elevated to 50 ± 4 mg/L 24 h post-race 49 ; and a six-day ultra-marathon (mean ± SD) pre-race (mg/dL) 0.19 ± 0.14, post-race 1.84 ± 0.88, with a peak on day 2 of 3.75 ± 1.70, 45 but not in other studies on simulated downhill running. 50 Chronically, exercise training may reduce the concentration of CRP, an adaptation that may be important in the context of reducing the risk of diseases such as type 2 diabetes.46,51
Changes to biomarkers associated with injury and pathology
Creatine kinase and myoglobin – biomarkers of muscle injury
Changes to creatine kinase, myoglobin and associated biomarkers of muscle injury.
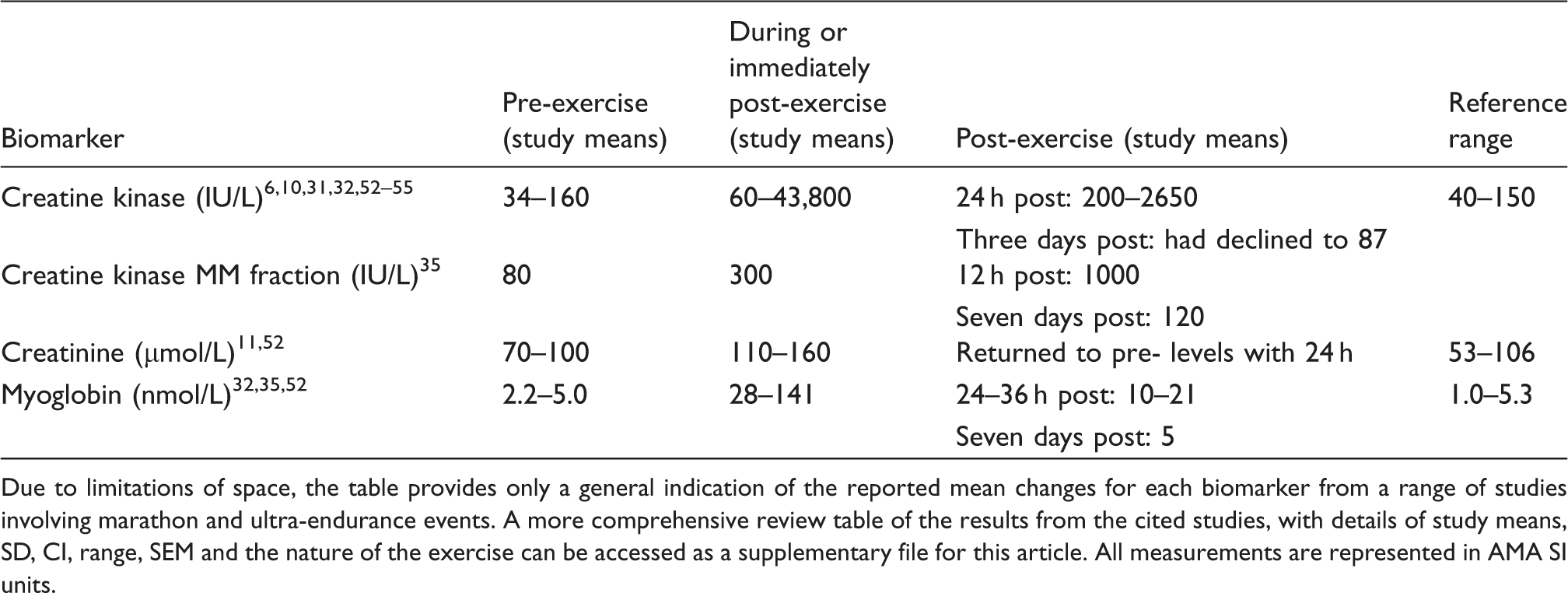
Due to limitations of space, the table provides only a general indication of the reported mean changes for each biomarker from a range of studies involving marathon and ultra-endurance events. A more comprehensive review table of the results from the cited studies, with details of study means, SD, CI, range, SEM and the nature of the exercise can be accessed as a supplementary file for this article. All measurements are represented in AMA SI units.
An interesting characteristic of DOMS is that after the initial bout of exercise, adaptations occur to provide some protection against the future occurrence of DOMS and reduce its severity. In practice, this means that if the same bout of exercise is undertaken a week or so later, any subsequent DOMS will be of lesser severity than that experienced after the first exercise bout, and if the exercise bout is repeated often enough, DOMS will no longer occur. This protection can last from a few weeks to several months.62,63
In the context of severe exercise bouts such as marathons and ultra-marathons, some studies have reported that over half of the participants have elevated creatine kinase, 52 which can exceed 2400 IU/L. In these studies, serum CK is reported to peak 24 h after the marathon, remaining 15-fold above baseline and not returning to pre-event concentrations for over a week. 31 Even higher values have been reported in an ultra-marathon (161-km footrace), in which 6% of the subjects recorded values >100,000 IU/L, 53 and similar results were reported for a 264-km footrace. 54 In these contexts, the elevated CK indicates exertional rhabdomyolysis and reflects the muscle damage caused by the severe exercise bout. 58
Elevations in myoglobin are also evident following a marathon and indicate that running has the potential to cause rhabdomyolysis, muscle cell leakage and haemolysis with >90% of the assessed subjects in a marathon and half-marathon having significantly elevated serum myoglobin immediately and 1 h post-race. 52
Biomarkers associated with liver injury
Changes to biomarkers associated with liver and/or muscle damage.
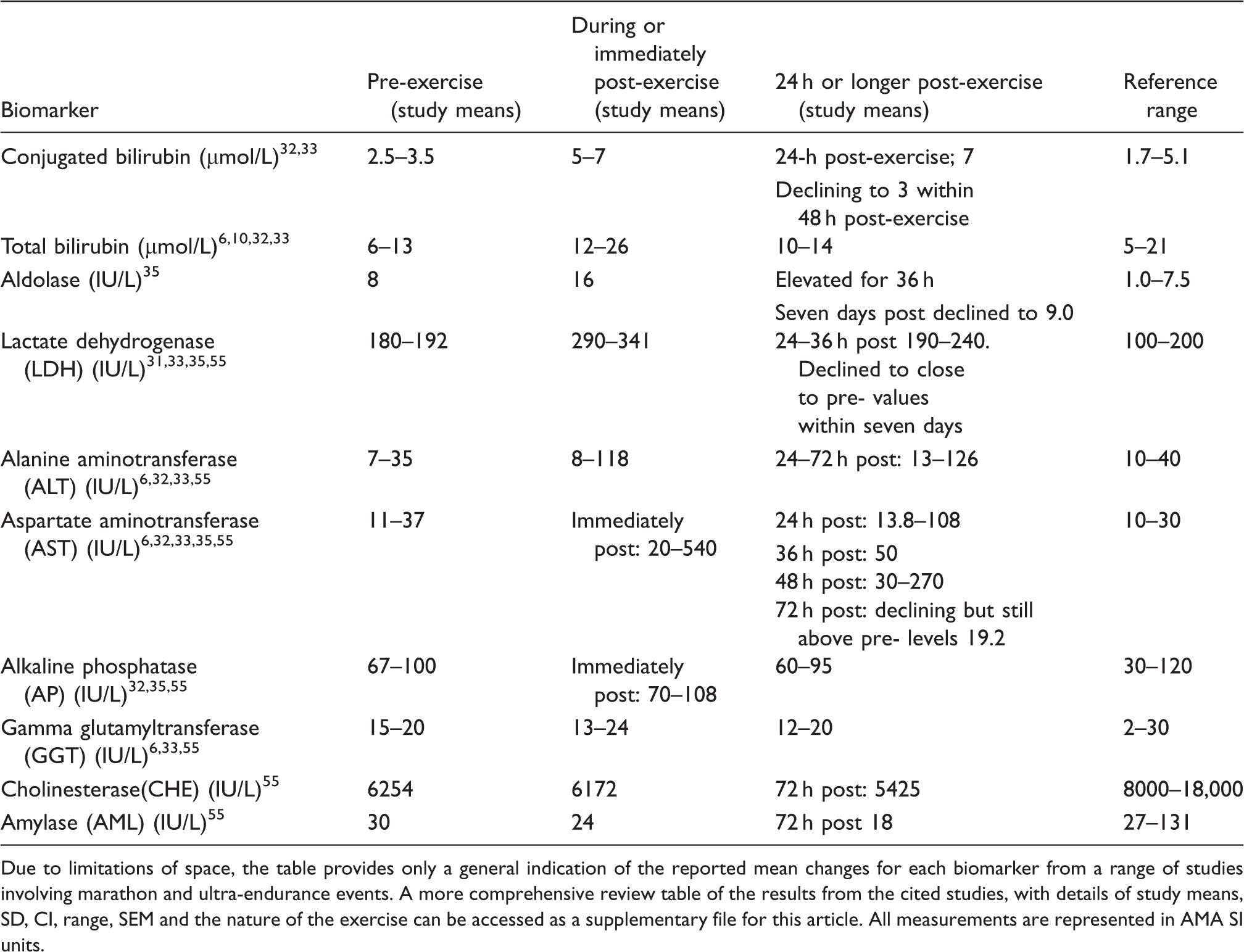
Due to limitations of space, the table provides only a general indication of the reported mean changes for each biomarker from a range of studies involving marathon and ultra-endurance events. A more comprehensive review table of the results from the cited studies, with details of study means, SD, CI, range, SEM and the nature of the exercise can be accessed as a supplementary file for this article. All measurements are represented in AMA SI units.
Biomarkers of cardiac pathology
Changes to biomarkers associated with cardiac injury.
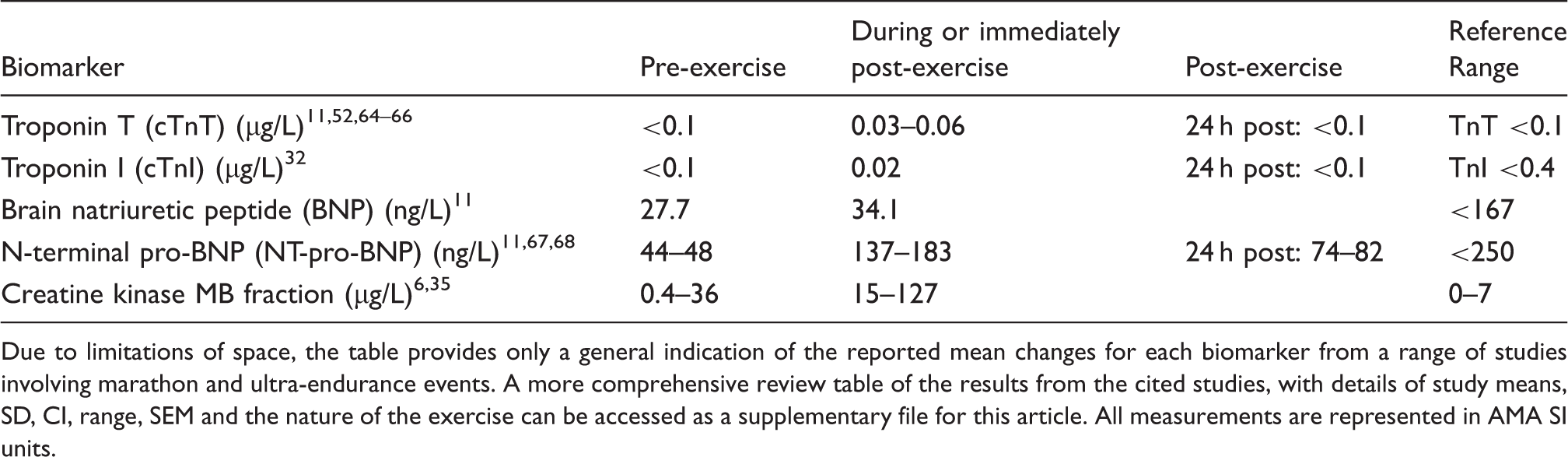
Due to limitations of space, the table provides only a general indication of the reported mean changes for each biomarker from a range of studies involving marathon and ultra-endurance events. A more comprehensive review table of the results from the cited studies, with details of study means, SD, CI, range, SEM and the nature of the exercise can be accessed as a supplementary file for this article. All measurements are represented in AMA SI units.
Brain natriuretic peptide (BNP), pro-BNP and N-terminal pro-BNP (NT-pro-BNP) are markers of cardiac stress. 11 N-terminal pro-BNP is the inactive fragment that is generated when it is cleaved from the larger pro-BNP molecule during the production of the active BNP hormone. Notably, NT-pro-BNP has a longer half-life than BNP, which facilitates its use as a clinical marker of cardiac dysfunction. In the context of marathon running studies, N-terminal pro-BNP (NT-pro-BNP) is reported to be elevated, post-marathon, with mean post-marathon concentrations of 183 and 137 ng/L.11,67 In one study, the authors also reported that 38 of their 46 subjects recorded concentrations that were comparable with those indicating cardiac events and disease. 67 In this study, these concentrations declined in two-thirds of the measured runners within 3 h of completing the marathon, and in both studies, 24 h post-marathon they had declined further.11,67 Likewise, elevations (27.3–310 ng/L) of NT-pro-BNP have also been reported in multi-day (4800 km) cycling races but in common with other studies the concentrations rapidly returned to below detection concentrations post-race. 68 In one study that reported post-marathon BNP concentrations as well as NT-pro-BNP, 11 the mean of the BNP concentrations had only risen by around 20% and this was not statistically significant, unlike the mean of the corresponding NT-pro-BNP concentration which had increased by more than 300% from the pre-marathon concentration. Similarly, one study that measured pro-BNP following repeated bouts of severe prolonged running, reported that while some runners displayed elevated concentrations of pro-BNP, >100 ng/L above pre-exercise concentrations (>200% increase), these did not exceed the clinical cut off (>125 ng/L) for congestive heart failure patients, and had returned to pre-exercise concentrations within 24 h of the last exercise bout. 72 The authors’ overall conclusion from this was that despite the temporary elevations in these biomarkers, the exercise was having minimal clinical impact.
Acute exercise cardiovascular risks
The increased risk of a cardiovascular event during and immediately following exercise is believed to be associated with the presence of underlying atherosclerosis, elevations in blood pressure and stress on the artery walls causing the disruption of plaques in the affected areas. 75 Other possible contributing factors to cardiovascular events during or immediately post-exercise include haematological changes, such as platelet activation arising from increased shear stress, 76 oxidative injury or release of catecholamines, especially in sedentary individuals.76–79 An increase in platelet function, coupled with the potential for splenic release of sequestered platelets and a relative increase in platelet counts due to acute dehydration may result in a net increased risk of platelet mediated thrombosis during and immediately following exercise.77–83 Particularly if combined with increased oxidative stress and triggering of plasma coagulation,84,85 these factors contribute to an increased burden of cardiovascular complications and sudden death during and immediately after exercise.86,87 Contextually, fibrinolytic system activation is observed after acute submaximal aerobic exercise in sedentary but otherwise healthy participants, 87 whereas platelets from trained athletes are less responsive to chemical stimulation, and there is evidence to suggest that greater and more strenuous bouts of exercise are necessary to induce the same level of pro-thrombotic response seen in sedentary individuals. These changes may reflect adaptation and contribute to the long-term beneficial effects of exercise against thrombotic risk and cardiovascular outcome in physically active individuals. 88
Conclusion
Strenuous and unfamiliar exercise can produce changes to biomarkers that are normally associated with pathology of several tissues including skeletal muscle, the liver and the heart. For example, the concentrations and/or activities of myoglobin, leukocytes, creatine kinase, bilirubin, cardiac troponins, lactate dehydrogenase, alanine aminotransferase, AST and NT-pro-BNP are all substantially altered in response to a bout of severe prolonged exercise. However, such changes are transient and full recovery (i.e. a return to pre-exercise baseline concentrations) occurs within days, without any apparent long-term adverse consequences. It is also evident that the magnitudes of these responses are extremely variable between individuals – see Supplementary files for additional details of standard deviations etc., from the cited studies.
Unfamiliar amounts of downhill running or resistance training can also increase creatine kinase and cause delayed onset of muscle soreness that peaks 36–72 h after the exercise bout. Other changes to factors such as RBC count, HCt, Hb and plasma volume are also transient and commonly remain within the reference range. Similarly, electrolyte and glucose concentrations are well maintained and the incidence of hypoglycaemia and hyponatremia are rare, even in very severe bouts of prolonged exercise. A knowledge of these exercise-induced changes to biomarkers that are commonly associated with pathologies will facilitate a greater understanding and appropriate interpretation of laboratory results from individuals who have recently undertaken strenuous exercise, and for whom the elevated concentrations and/or activities of these biomarkers may not necessarily indicate the presence of chronic pathology.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not required.
Guarantor
SB.
Contributorship
All authors contributed to all stages of the preparation of this review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.