
Abstract
Background
Testosterone measurement by liquid chromatography tandem mass spectrometry (LC-MS/MS) is well accepted as the preferred technique for the analysis of testosterone. Variation is seen between assays and this may be due to differences in calibration as commercial calibrators for this assay are not readily available. We investigated the effects calibration in routine clinical LC-MS/MS assays.
Methods
All LC-MS/MS users that were registered with the UKNEQAS external quality assurance scheme for testosterone were invited to take part in the study. A set of seven serum samples and serum-based calibrators were sent to all laboratories that expressed an interest. The laboratories were instructed to analyse all samples using there own calibrators and return the results and a method questionnaire for analysis.
Results
Fifteen laboratories took part in the study. There was no consensus on supplier of testosterone or matrix for the preparation of calibrators and all were prepared in-house. Also, a wide variety of mass spectrometers, internal standards, chromatography conditions and sample extractions were used. The variation in results did not improve when the results were corrected with a common calibrator.
Conclusions
The variation in results obtained could not be attributed to variations in calibrators. The differences in methodologies between laboratories must be the reason for this variation.
Testosterone measurement by liquid chromatography tandem mass spectrometry (LC-MS/MS) is now accepted as the preferred technique for the analysis of serum testosterone in both men and particularly women. Despite this, variation can be seen between LC-MS/MS assays on external quality assessment schemes and is most likely to be due to method differences between laboratories. 1 One possible area of inconsistency among routine LC-MS/MS assays is the lack of commercially available calibrators. This has previously been shown to have a large effect on LC-MS/MS vitamin D assays. 2,3 We investigated the effects of calibration on the results achieved by routine clinical LC-MS/MS assays.
All LC-MS/MS users registered in the UKNEQAS external quality assurance scheme were invited to take part in the study. Of approximately 16 users, 15 took part. A set of 21 samples were prepared for analysis. Seven were serum samples from normal volunteers which had been mixed to give different concentrations in the male and female ranges, seven were calibrators prepared from female serum and spiked with testosterone (Sigma, Poole, UK, 0.5–51 nmol/L) and seven were aqueous calibrators (phosphate-buffered saline; PBS containing 0.1% [weight/volume] bovine serum albumin; BSA 0–53.1 nmol/L). The participants were asked to analyse all samples in singleton using their routine assay and calibrators and return all testosterone concentrations and detector responses (testosterone area or height/internal standard area or height). The participants were also asked to complete a questionnaire on their method and calibration parameters. The results for the seven serum samples were recalculated using the assigned serum and aqueous calibrator concentrations and detector responses identified in the participants laboratories. This corrected results for a common calibrator. As the participants were also asked to provide their calibration parameters, such as weighting or origin inclusion, these were used during the correction to ensure it was performed with the specific parameters for each laboratory. The method used to assign the target concentrations to the serum and aqueous calibrators was adapted from Gallagher et al. 4 This method uses an extraction with methyl tertiary butyl ether and D2 internal standard (QMx, Thaxted, UK). Chromatography was performed on a Synergi Hydro-RP 50 × 3 mm column (Phenomenex, Macclesfield, UK) with isocratic elution using 70% organic mobile phase. This method had previously shown to have a minimal ion suppression profile and gave excellent agreement with a reference method. 5 The primary transitions monitored in electrospray ionization positive mode were m/z 289.2 > 96.9, 291.2 > 98.9, for testosterone and D2 testosterone, respectively.
In the 15 laboratories participating there were seven different types of sample extraction used, twelve types of LC column, nine different mass spectrometers and three types of internal standard.
Wide variations in concentrations were seen for the seven serum samples when analysed by all laboratories using their in-house calibrators. The coefficient of variation for the samples was 93% for the lowest sample which had a mean concentration of 0.61 nmol/L despite this concentration being within the working range of all these assays. As shown in Figure 1a, the variability of results obtained for the three samples in the female range is in general much greater than in the male range (Figure 1b). This variability does not improve after correcting the serum samples for differences in calibrator. In the male samples, the variability is smaller than in the female range but these also do not improve after correcting for the calibrator. This suggests that it is differences in methodologies that are causing this variation. The coefficients of variation are reduced when correcting using the aqueous calibrators in the males and female ranges. The CVs were 99%, 13% and 24% before correction in women, 92%, 13% and 13% postcorrection. In men the CVs were 13%, 10%, 15% and 11% precorrection and 5%, 9%, 8% and 8% postcorrection. This suggests that matrix effects could be a significant component to the variability seen. This theory is supported by the wide variety of chromatography columns and conditions employed. If matrix effects are occurring in an assay and aqueous calibrators are employed, this may result in inaccurate estimation of testosterone in matrixed samples.
The spread of results obtained for seven serum samples when analysed using each laboratory's in-house calibration (e.g. 1) and after correction for calibration differences (e.g. 1c). The results from the female and male ranges following correction with serum calibrators are shown in (a) and (b) respectively. Panels c and d show the results for the same samples before and after correction with aqueous calibrators in female and male samples respectively. The numbers across the top of the charts show the coefficient of variation for the results from each sample before and after correction.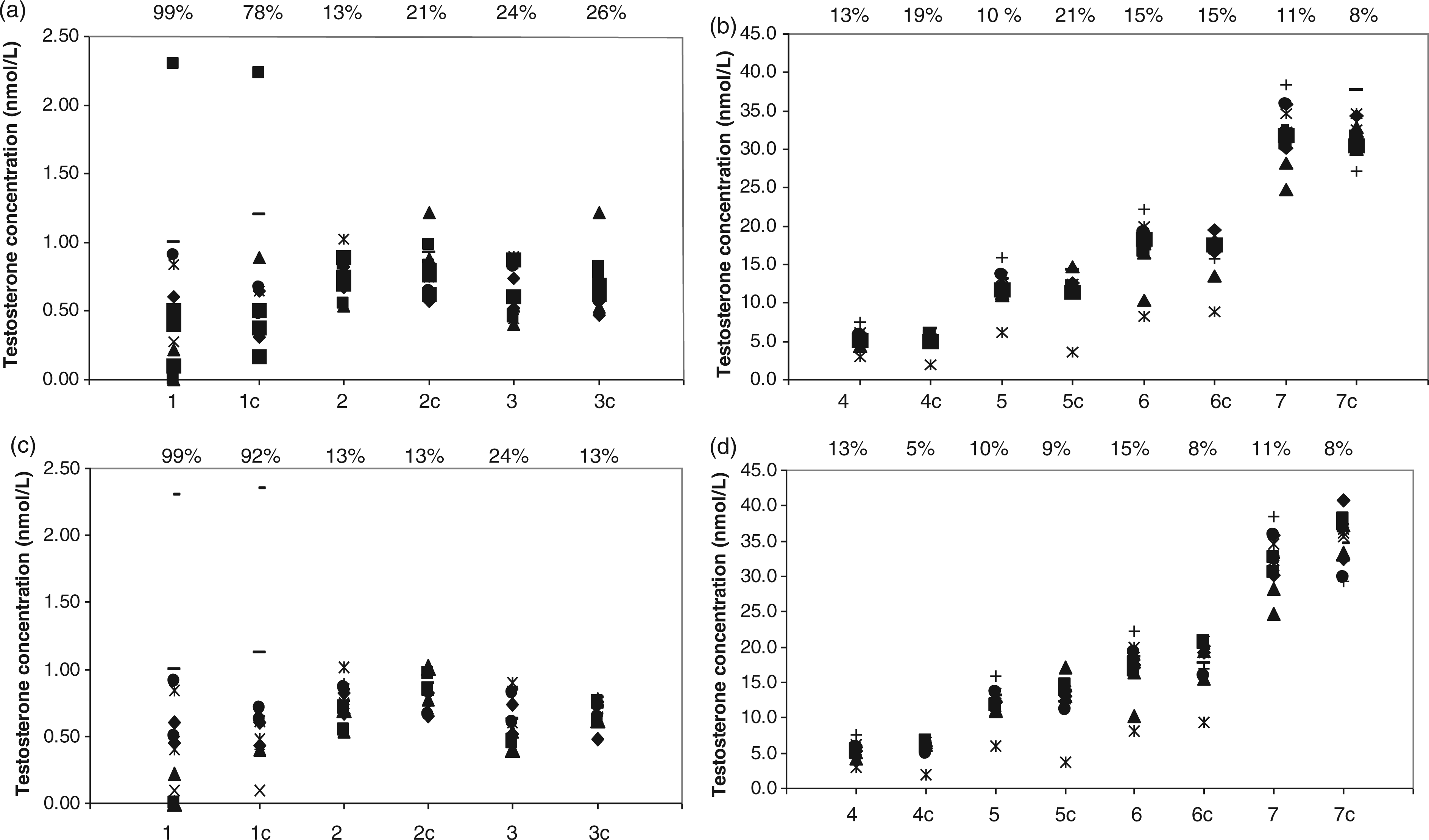
We found that calibrators are not responsible for the variation seen in routine clinical LC-MS/MS testosterone assays; however there are ongoing efforts to standardize testosterone calibration. 6 This is different from what has previously found for vitamin D 2,3 and is likely due to the wider heterogeneity of testosterone assays. Potential contributors include chromatography column and conditions; local experience when evaluating several LC columns has shown ion suppression to vary between 10% and 100% for the same injected sample extract during postcolumn infusion experiments. We have also demonstrated that the choice of internal standard can also contribute to differences in results (in press). 7 Thorough method validation including comparison to a reference method would help to harmonize testosterone results for LC-MS/MS users.
Footnotes
Acknowledgments
The authors would like to acknowledge Finlay MacKenzie UKNEQAS and all laboratories for facilitating and taking part in this study.
Declaration of conflicting interests
None.
Funding
None.
Ethical approval
None.
Guarantor
BK.
Contributorship
BL and LO researched the literature and conceived the study. PM was involved in preparation and distribution of materials and data collection. LO performed the data analysis and wrote the manuscript. PM reviewed and edited the manuscript.