An accurate estimation of serum bicarbonate concentration (HCO) is essential to the diagnosis and treatment of acid-base disorders and electrolyte disturbances. We noted significant discrepancies between HCO concentration measured by the Olympus AU2700 analyser and total serum carbon dioxide (TCO2) concentration derived from a Radiometer blood gas analyser on several patient samples. This was reported to the manufacturer which led to a recall of certain reagent lot numbers. We hypothesised the mechanism for this interference to be elevated levels of lactate dehyrogenase (LD).
Methods
We investigated the effect of increasing LD concentration on HCO with the reagent lot that was recalled and compared this with a subsequent reagent lot that was known to be unaffected on an Olympus AU2700.
Results
The experimental data confirmed a positive interference in the Olympus AU2700 HCO assay using older reagent lot numbers. The false positive HCO interference was significant (>10% change) when the LD concentration exceeded 845 U/L.
Conclusions
Very high levels of LD concentrations were the cause of interference in the Olympus AU2700 HCO enzymatic assay. Laboratorians should be aware that very high levels of LD may be a potential interference in some enzymatic HCO assays.
The measurement of serum bicarbonate concentration (HCO) is important in the evaluation of both acid–base status and electrolyte balance. Total carbon dioxide (TCO2) content is a measure of carbon dioxide (CO2) existing in several states: CO2 in a physical solution is loosely bound to proteins, or exists as bicarbonate (HCO) or carbonate (CO) anions, and carbonic acid (H2CO3).1 Measurement of TCO2 as part of the electrolyte profile is useful in evaluating HCO concentration.
The clinical biochemist on call received a call from an intensivist regarding the validity of a HCO result, 16 mmol/L reported from the laboratory. The patient was a 72-year-old woman who presented with multiorgan failure secondary to severe alcoholic pancreatitis and worsening metabolic acidosis. At the same time a point-of-care (POCT) (Radiometer 700FLEX, Radiometer, Copenhagen, Denmark) calculated HCO result was 6 mmol/L. The POCT result was more reflective of the patient clinical status and in line with the pH of 7.06. Subsequent samples from this patient also generated significantly different results between the laboratory and the POCT analysers. When these samples were analysed on an Olympus AU680 (Beckman-Coulter, Sydney, Australia) analyser that uses the same reagents, the positive interference was replicated, mirroring the Olympus AU2700 (Beckman-Coulter, Sydney, Australia) results, confirming the interference was specific to the Olympus reagent. Previously falsely elevated TCO2 has been reported to be caused by iodine interference.2 To our knowledge this patient had no iodine treatment of any kind. It was noted that her initial lactate dehydrogenase (LD) was 4490 U/L which reached a peak of 14,200 U/L within 24 hours of admission to the hospital. This gradually decreased to 650 U/L within seven days when the patient deceased.
Since this encounter, a laboratory change process was implemented, re-analysing any sample with elevated LD (>2000 U/L) on the Olympus analysers for HCO on an alternative analyser/method (OPTI CCA (Osmetech, Roswell, GA, USA) or Siemens RapidLab 1265 (Siemens Healthcare Diagnostics, Tarrytown, NY, USA) blood gas analysers). During this process several other samples with positive HCO interference on the Olympus analysers were detected and confirmed. Internal Quality control and patient means did not shift and no issues with external quality assurance material were encountered during this period. Since all of these samples with positive interference had high LD concentrations this prompted us to investigate the effect of elevated LD on HCO results. These findings were immediately conveyed to the manufacturer.
Method
Bicarbonate concentration [HCO] can be directly measured or derived from calculations using the Henderson–Hasselbalch equation. Bicarbonate ions make up ∼95% of the total carbon dioxide of the plasma and hence both of them have been used interchangeably.1 Laboratories use auto-analysers for measuring TCO2 content. At present, most methods for direct measurement of TCO2 utilize enzymatic reactions. The Olympus AU2700 utilizes the following enzymatic method:
The oxidation of NADH results in a decrease in absorbance of the reaction mixture measured bichromatically at 380/410 nm proportional to the bicarbonate content of the sample.
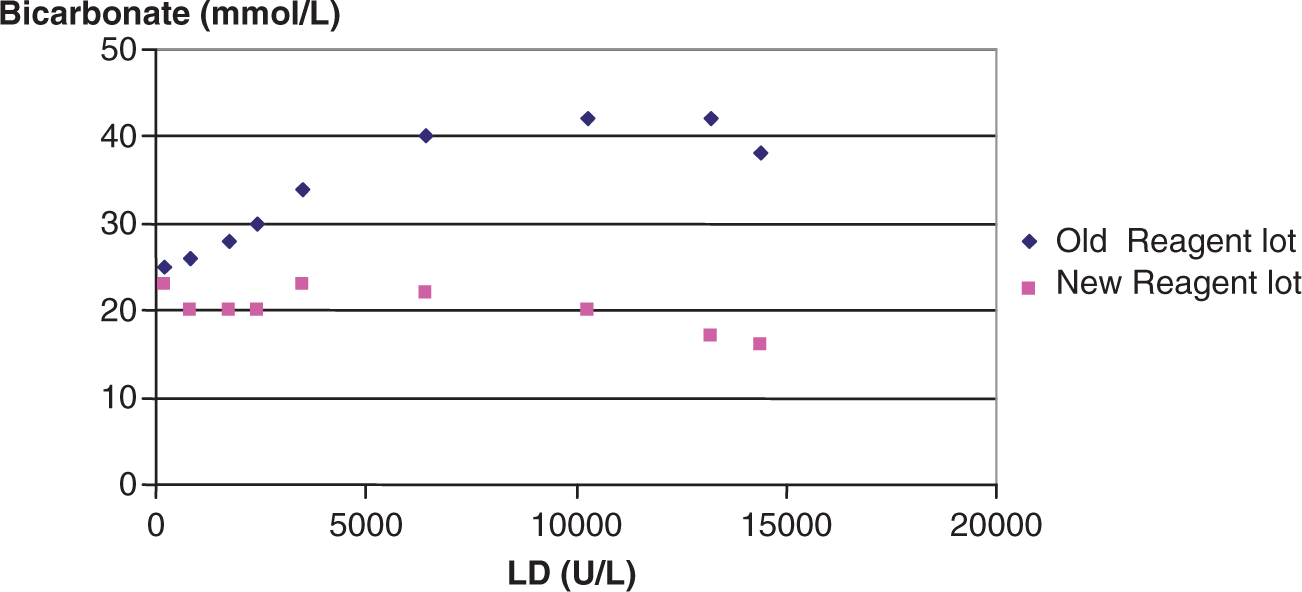
To investigate if the increasing LD concentration was the cause of the elevated HCO results, two serum pools were prepared. One pool had high LD concentration (14,100 U/L) and the other pool had normal LD concentration (184 U/L). Serial dilutions were prepared of the high LD pool with the normal LD pool. HCO levels were measured on these samples on an Olympus AU2700 analyser using a reagent lot that was recalled as well as a subsequent new reagent lot that is known to be unaffected. The results are shown in Figure 1.
Effect of increasing lactate dehydrogenase concentration on the HCO results with old and new HCO reagent lot numbers on the Olympus AU2700 method.
Results and discussion
The experimental data confirmed a positive interference in the Olympus AU2700 HCO assay using older reagent lot numbers. The false-positive HCO interference was significant (>10% change) when the LD concentration exceeded 845 U/L. Similar interference in the enzymatic HCO assay by pyruvate and LD has been described in horses.3 In the presence of NADH, pyruvate is reduced to lactate in a reaction catalysed by LD generating NAD. Pyruvate in the sample may be endogenous produced in vivo or produced by decarboxylation of oxaloacetate to pyruvate.4 Increased LD would accentuate the decarboxylation of oxaloacetate to pyruvate.
In the enzymatic HCO assay reaction, consumption of NADH decreases ultraviolet absorption in proportion to enzyme activity. Most enzymatic methods to measure HCO utilize the LD inhibitor, oxamate to inhibit the consumption of NADH by pyruvate. Oxamate competitively inhibits LD through the formation of a ternary enzyme-NADH-oxamate complex. However, in extreme cases, serum LD activity may be high enough to overwhelm the oxamate inhibitory activity with the resultant consumption of NADH and falsely increase HCO concentration.
We hypothesize the above as the mechanism for the positive interference seen in this the patient samples in this study. Although we are unable to confirm whether oxamate is used and at what concentration in the Olympus reagents, it is possible that the reagent lots that were affected may not have had an LD inhibitor that was of sufficient concentration to completely inhibit the LD activity. It is feasible that these samples contained increased endogenous pyruvate concentrations.
A falsely high HCO due to unsuspected artefact can lead to masking of clinically significant acidosis which may lead to significant delays in investigating the cause of acidosis and potentially unfavourable patient outcomes. Laboratorians should be aware that very high levels of LD may be a potential interference in some enzymatic HCO assays. Laboratories experiencing similar problems with HCO should perform independent studies to determine it is due to elevated LD and from there on implement appropriate process to minimize erroneous results being reported. In our case, the interference in the Olympus HCO assay by elevated LD was specific to a particular reagent lot numbers and the reagents in current use are not affected. The prompt communication with the manufacturer led to a prompt resolution, affected reagent lot numbers were recalled and new reagent formulation provided to eliminate any such interference.
Footnotes
Acknowledgements
We would like to acknowledge Vicki Underwood and Romina Straccia for collection and storage of high LD samples.
Declaration of Conflicting Interests
None.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Guarantor
MS.
Contributorship
All authors contributed to the design of the experiments. LB performed the LD analyses. MS wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
References
1.
ChittammaAVanavananS (2008) Comparative study of calculated and measured total carbon dioxide. Clin Chem Lab Med, 46: 15–7.
2.
Abdel-WarethLOLirenmanDSHalsteadACMcLellandDCarletonBC (1995) Spurious rise in total carbon dioxide and chloride with negative anion gap after cystogram. Pediatr Nephrol, 9: 348–50.
3.
CollinsNDLeRoyBEVapL (1998) Artifactually increased serum bicarbonate values in two horses and a calf with severe rhabdomyolysis. Vet Clin Pathol, 27: 85–90.
4.
PeledN (1981) An enzymic bicarbonate reagent that is free of pyruvate interference. Clin Chem, 27: 199–200.