
Abstract
Proteinuria is the cardinal sign of renal disease, therefore accurate identification of clinically significant proteinuria is essential to the diagnosis and management of kidney disease. Spot samples are now widely used, namely protein: creatinine ratio (uPCR) and albumin: creatinine ratio (uACR). In this article we review the evidence comparing uPCR and uACR including clinical, laboratory and financial arguments.
uPCR has a superior performance to uACR to predict 24-hour total proteinuria, the measurement on which the evidence for interventions in chronic kidney disease is based. Furthermore a retrospective study comparing uPCR and uACR as predictors of renal outcome found comparable performance to predict all-cause mortality, commencement of renal replacement therapy and doubling of serum creatinine. Only uPCR takes account of non-albumin proteinuria which has been shown to have prognostic significance. uACR was been thought to be superior at low levels (where there is less ‘noise’ from physiological urinary proteins), but uPCR has recently been shown to perform well at levels equivalent to <0.5 g/day (and even within the reference range) as a predictor of outcomes. uACR is measured using an immunoassay that may be technically superior, but is not without shortcomings (such as antigen excess) and is 2–10 times more expensive than uPCR.
The theories explaining the superiority of albumin are appealing. However, the available comparative data do not seem to support the theory. We cannot explain the disparity, but in science, if the data do not fit the existing theory, then maybe it's time for a new theory.
Introduction
Measures of albumin and protein excretion in the urine.
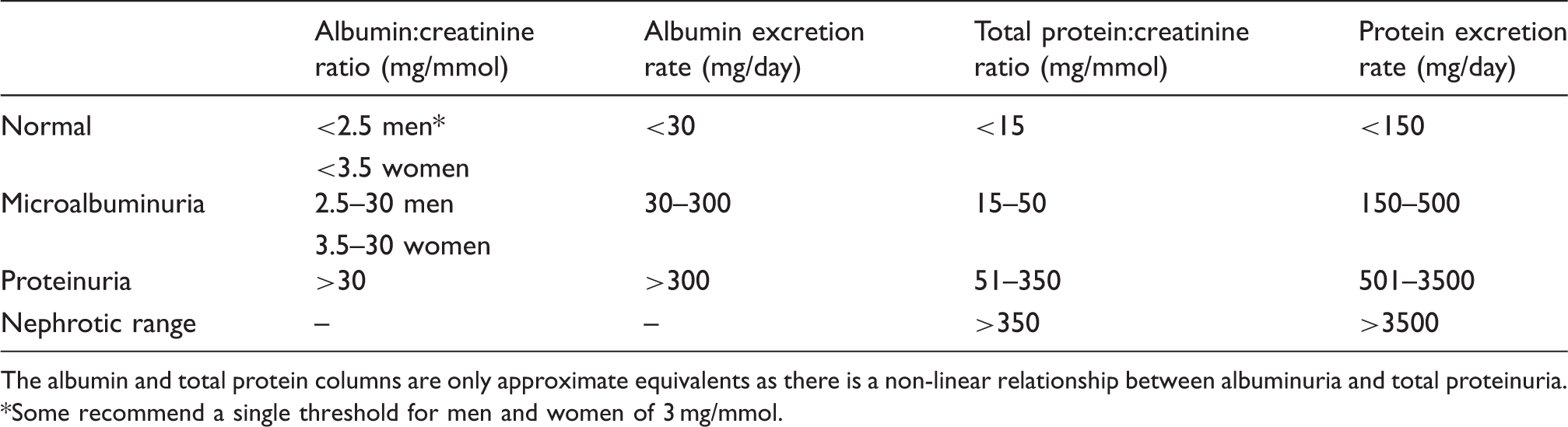
The albumin and total protein columns are only approximate equivalents as there is a non-linear relationship between albuminuria and total proteinuria.
Some recommend a single threshold for men and women of 3 mg/mmol.
The prevalence of chronic kidney disease (CKD) stages 3–5 is around 4.5–5.0% in the UK 11,12 (around 3 million patients). The UK Quality Outcomes Framework rewards primary care for annual quantification of proteinuria in approximately five million patients on CKD and diabetes registers combined, underlining the importance of recommending the optimal test.
However, the question remains, what should be measured in the spot urine sample: protein:creatinine ratio (uPCR) or albumin:creatinine ratio (uACR)? In this article, we review the evidence comparing uPCR and uACR, including clinical, laboratory and financial arguments.
Prediction of 24-h total proteinuria
The evidence for clinical interventions in non-diabetic CKD such as target blood pressure and renin–angiotensin system blockade is based on the measurement of 24-h total proteinuria. 13 Therefore, the spot measurement must have a good overall correlation with 24-h total proteinuria. Additionally, it should correctly identify patients excreting >0.5 g/day or >1 g/day of proteinuria as these are important diagnostic thresholds; for instance, >1 g/day is frequently an indication for renal biopsy. 14 In a secondary care cohort of 6842 patients with CKD and simultaneous spot measurements of urine total protein, albumin and creatinine, we found that uPCR had superior test performance to uACR to predict 24-h proteinuria. 15 uACR had a sensitivity of only 79.0%, compared to uPCR’s 93.9% sensitivity to predict 1 g/day of total proteinuria. To improve the sensitivity of uACR to a comparable level with uPCR, uACR’s cut point fell to 17.5 mg/mmol, with resultant fall in specificity to 69.8% (cf. uPCR 88.5%). Given that spot urine tests are used as a screening test by non-nephrologists, sensitivity is of prime importance. In the population-based Australian Diabetes and Obesity (AusDiab) study, uACR was also compared to uPCR, but without 24-h urine samples. Within the clinically relevant range of 0.5–3.0 g/day, uPCR and uACR have a non-linear relationship which means one value cannot be reliably extrapolated from the other. 16 They advocated using uPCR in patients with known or suspected renal disease.
Prediction of outcomes relevant to patients
It is perhaps not surprising that uPCR is superior to uACR at predicting 24-h total proteinuria. Far more important than this is the prediction of patient outcomes in CKD. There is increasing evidence demonstrating the importance of proteinuria as a predictor of adverse outcomes, whether measured by dipstick, uACR or uPCR. 2,17,18 However, there are no head to head prospective studies comparing uPCR and uACR as predictors of progressive renal disease, the need for renal replacement therapy (RRT) or death in patients with CKD. There are also surprisingly few retrospective comparisons. In a retrospective study of 5586 patients attending hospital renal clinics, we found that uPCR and uACR had comparable performance to predict doubling of serum creatinine, commencing RRT and all-cause mortality. 4
The issue of non-albumin proteinuria
In pathological states, total proteinuria is made up of:
low levels of physiological proteins (e.g. uromodulin) albumin (the predominant protein in most disease states) non-albumin proteins (comprising a wide range of proteins, of varying molecular weights) specific pathological proteins (e.g. immunoglobulin light chains)
The relative proportions of these proteins vary widely in pathological states (e.g. minimal change nephropathy where albuminuria predominates, versus tubulo-interstitial disease with a larger proportion of non-albumin proteinuria). 19 The non-albumin proteins are less well defined than albumin. However, there is evidence of the their pathophysiological importance: one study showed that high molecular weight proteinuria was a superior predictor of renal progression than intermediate weight, low molecular weight and even total proteinuria. 20 This may be as a result of increased tubular toxicity, though an alternative hypothesis is that this finding is simply a consequence of loss of glomerular size selectivity. Importantly uPCR takes account of these proteins while uACR only measures albumin.
In our retrospective secondary care cohort, we examined the outcomes of patients with high levels of non-albumin proteinuria who would not have been identified as having significant proteinuria using uACR alone. 21 We showed that those with high non-albumin proteinuria were older, with poorer kidney function and had worse outcomes than those with heavy albuminuria (in terms of progressive renal decline measured by doubling of serum creatinine, commencement of RRT and all-cause mortality). When these factors were entered into a multi-variate model some of the excess risk was truncated, but they remained a high-risk group that would be identified using uPCR, but not with uACR, which failed to identify 16% of patients with proteinuria >1 g/day. The AusDIAB study of the general population used a lower threshold for proteinuria (≤0.2 mg/mg equating to 0.2 g/day) and also found that uACR failed to detect 8% of patients with proteinuria.
The issue of microalbuminuria
Microalbuminuria is a term used to refer to low level urinary albumin loss (uACR around 3–30 mg/mmol; see Table 1). One of the arguments often given in favour of uACR is that it has superior sensitivity at microalbuminuria levels. The theoretical paradigm underpinning this is that by using uACR one can measure albumin as a marker of risk (i.e. the signal), without measuring physiological proteins (i.e. noise), thus increasing sensitivity by minimizing the noise-signal ratio. This assumes that the quantity of non-albumin proteinuria adds no additional information to albumin, and that the quantity of physiological proteinuria is irrelevant to risk. Surprisingly, this paradigm has only recently been tested in head to head comparisons. 4,21
Our study showed that uPCR had comparable performance to uACR at microalbuminuria levels. 4 Risk associated with albuminuria is raised even at levels lower than microalbuminuria. 2 However, even when our reference group was divided in two, and the lower half used as the reference group in survival modelling, the utility of uPCR persisted showing that low levels of uPCR are also clinically useful. These unexpected findings need to be confirmed by others, but challenge the paradigm above.
Even if our findings are not found to be generalizable, there is a second issue with arguments based on the importance of microalbuminuria: there is little evidence for effective interventions in non-diabetic patients with low level proteinuria. Therefore, one of the WHO screening requirements is not met by uACR: the availability of an effective intervention for the identified condition. 22 There is robust evidence for the use of renin–angiotensin system blockade for the treatment of microalbuminuria in diabetes, but in non-diabetic CKD meta-analyses identified 0.5 g/day of total proteinuria as the threshold for deriving benefit 5 and >1 g/day of total proteinuria as the threshold above which systolic blood pressure targets should be reduced from <140 mmHg to <130 mmHg. 23 uPCR performs extremely well to identify this moderate level of proteinuria with no extra benefit gained from the use of uACR.
Even in diabetic nephropathy, the evidence for superiority of uACR is built on shaky foundations. Early studies promoting the concept of microalbuminuria did not examine the utility of uPCR levels below the laboratory reference range for predicting outcomes. 24,25 Nevertheless, and in contrast to non-diabetic CKD, most intervention studies in diabetic kidney disease used albuminuria, so uACR remains the test of choice for that group.
Issues relating to laboratory assays
Total proteinuria is generally measured by physico-chemical techniques such as colorimetric or turbidimetric assays, in order to measure the variety of proteins present in urine. Urine albumin is measured by immunoassays, using specific antibodies directed against albumin, and theoretically measure a single entity with greater accuracy and precision. For this reason, they are considered to be technically superior. However, urine albumin assays are not without their shortcomings. At high urine protein concentrations, the albumin antibodies can be overwhelmed leading to falsely low results, a phenomenon known as ‘antigen excess’. There can also be cross contamination from serum samples using auto analyser methods.
Urine is a hostile and highly variable biochemical environment with a wide range of pH, osmotic concentration, exposure to differential reabsorption and proteolysis. Consequentially, there are a wide variety of albumin species and fragments within urine, which make assay standardization a challenge. Significant intra- and inter-laboratory assay differences also persist and have hindered standardization efforts to date. 26 Differences between urine albumin assays are clinically significant: in the AusDiab study, immunonephelometry and high-performance liquid chromatography (HPLC) techniques were compared. HPLC detects both immunoreactive and non-immunoreactive albumin. They found a four-fold increase in the prevalence of albuminuria using HPLC compared to immunonephelometry, but the implications are unclear as the prognostic impact of these different moieties is not well defined. 27 There is no similar attempt to standardize total protein assays underway.
What guidelines recommend
Unsurprisingly, given the poor evidence base, there is considerable debate about the optimal measure of proteinuria with strong advocates of uPCR for non-diabetic kidney disease 28 and equally strong advocates for uACR for all. 29 This difference of opinion is reflected in national guideline recommendations with the Scottish Intercollegiate Guidelines Network (SIGN) and the Welsh National Services Framework recommending uPCR for non-diabetic kidney disease 7,30 and the National Institute for Health and Clinical Excellence (NICE) and the US National Kidney Foundation Kidney Disease Outcome Quality Initiative (NKF/KDOQI) favouring uACR for all patients, with NKF/KDOQI adding the caveat that if the uACR is >500 mg/g (∼57 mg/mmol), uPCR can be substituted. 8,9
Cost
The final consideration after that of clinical efficacy and laboratory performance must be cost. Exact pricing varies but albumin immunoassays are more expensive than total protein assays, with the cost of consumables being two to 10 times more for uACR. Even a small price differential per unit cost has ramifications when millions of samples are processed annually. In the current economic climate, with the mantra ‘do more with less’ it is incumbent upon advocates of more expensive tests to put forward convincing evidence of superiority in order to justify excess cost. There are no adequate health economic studies based on head to head comparisons of uACR and uPCR. NICE attempted an economic analysis based on the very limited information available. 8 They noted that uACR would need to be more sensitive than uPCR in order to justify its additional cost. We demonstrated that uPCR performed at least as well as uACR at predicting outcomes. We are unaware of any head to head studies demonstrating superiority of uACR to predict patient-relevant outcomes.
Conclusion
Many authors and guideline groups assert that uACR is superior to uPCR for predicting risk in CKD. However, this is based on assumptions, theoretical constructs and extrapolations: assuming that non-albumin proteins add no value to risk prediction; the theoretical construct that the signal-noise ratio of albumin is superior to total protein; and the extrapolation that better laboratory assay performance will lead to better clinical utility.
Much of the evidence directly comparing uPCR to uACR comes from our retrospective studies, and that should be a reason for caution in interpretation. We would encourage others to investigate this topic prospectively in large populations. Nevertheless, conventionally one does not introduce a new test until it has been proven to be superior to the existing test, and to have superior cost-effectiveness. Neither has been demonstrated for uACR. In fact, available evidence shows that uACR is less sensitive at predicting proteinuria, is no more effective at predicting patient-relevant outcomes, fails to detect a significant minority of proteinuric patients and is more costly.
The theories explaining the superiority of albumin are appealing. However, the available comparative data do not seem to support the theory. We cannot explain the disparity, but in science, if the data do not fit the existing theory, then maybe it is time for a new theory.
Footnotes
Acknowledgments
We would like to thank Dr Denis O’Reilly for his input regarding laboratory costs.
Declaration of conflicting interests
MSMcG was a member of the SIGN CKD guideline writing group and co-author of the Renal Association CKD guideline.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Guarantor
SM and MSMcG are co-guarantors.
Contributorship
The article was prepared at the invitation of the Clinical Sciences Reviews Committee of the Association for Clinical Biochemistry. SM wrote the original and re-draft of the review. MSMcG commented on each draft.