
Abstract
Objective:
The purpose of this study is to evaluate the postoperative urinary complications and the optimal timing of foley catheter removal in patients who underwent free flap reconstructive surgery for head and neck pathology.
Methods:
A retrospective case-control study of head and neck patients who underwent free flap reconstructive surgery at a single institution between January 2009 and December 2021 was conducted. Patient risk factors for postoperative urinary retention (POUR) were analyzed. Fisher Exact and Wilcoxon Rank Sum tests were used to evaluate rates of foley replacement, straight catheterization, and catheter-associated urinary tract infection (CAUTI) and associated risk factors.
Results:
Two hundred and eleven patients were included in this study. Older age, lower BMI, lower intraoperative fluid volumes, and need for straight catheterization were statistically significant for POUR requiring foley replacement. Shorter total (P = .04) and postoperative (P = .01) foley duration showed statistical significance for POUR requiring straight catheterization. About 60% of patients who had straight catheterization required a foley replacement (P < .001). Only one patient (0.5%) developed a urinary tract infection (UTI).
Conclusion:
Foley catheter duration impacts the risk of POUR requiring straight catheterization and subsequently, foley replacement. Optimal timing for foley catheter removal in the postoperative period remains to be elucidated. Removal of catheters between 21 and 48 hours after surgery may decrease the risk of POUR without increasing the rate of CAUTI in patients with head and neck pathology undergoing free flap reconstructive surgery.
Keywords
Introduction
The incidence of postoperative urinary retention (POUR) varies widely in the literature, ranging from 5% to 70%, and occurs when there is an inability to activate micturition in the presence of a full bladder. 1 The etiology of POUR is theorized to be related to obstruction, denervation, or overdistention. 1 Age and male gender are risk factors for POUR with an estimated 4% increase in the risk of developing POUR with every year of age.2,3 Additional risk factors include diabetes mellitus, prostate enlargement, neurologic disease, prior pelvic surgery, and increased duration of surgery.1,3,4
POUR is a significant complication associated with an increased risk of urinary tract infections (UTI), complications from catheter use, prolonged hospital admission, need for home care, and acute kidney injury.2,3,5,6 Catheter-associated urinary tract infections (CAUTI) are preventable hospital-acquired infections and are associated with a 1 to 2 days increased hospital stay and increased healthcare costs. 7 As such, the Centers for Medicare and Medicaid Services (CMMS) declared in 2008 that the additional cost related to a CAUTI would no longer be reimbursed to hospitals. 8
The incidence of POUR is reported at increased rates in patients undergoing joint arthroplasty, anorectal procedures, and gynecological procedures, suggesting that the risk of postoperative urinary complications is dependent on the procedure.1,2,4 However, the literature relating to the incidence of, and factors for, POUR in head and neck reconstructive surgical patients is limited. A consensus review on the use of the Enhanced Recovery After Surgery (ERAS) pathway for head and neck oncologic surgery recommends foley catheter removal to be as soon as possible, ideally within 24 hours after surgery.9 -12 The rationale for removing foleys at this specific time frame was based on gynecologic, thoracic, and abdominal literature. In addition, the review did not identify specific factors that influence the rates of urinary retention or UTIs.
Given this gap in the literature, the purpose of this study was to analyze the incidence of POUR in patients undergoing free flap reconstruction for head and neck cancer. We seek to identify associated risk factors for developing POUR and evaluate the optimal timing for foley catheter removal.
Methods
A retrospective case-control study at a single institution between January 2009 and December 2021 was conducted after the Penn State University Institutional Review Board (IRB) determined the research to be exempt. Patients who underwent ablative surgery with a head and neck surgical oncologist in the Otolaryngology-Head and Neck Surgery Department and subsequent free flap reconstruction were included. Patients were identified using the International Classification of Disease, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes for free flap reconstructive procedures. Patients under the age of 18, receiving dialysis, self-catheterizing pre-operatively, or with indwelling catheters were excluded. Patients who returned to the operating room prior to initial foley removal were excluded. For patients who returned to the operating room after initial foley removal, only the initial procedure and postoperative period were included.
Patient demographics including medical comorbidities, social history, and past surgical history were collected. Relevant comorbidities considered in this study were diabetes mellitus (type 1 or type 2), benign prostatic hyperplasia (BPH), prostate cancer, and neurologic disease. Relevant past surgical history included any history of urologic and gynecologic surgery. Intraoperative data included total operative time (as defined by anesthesia start and end times) and volume of intraoperative fluids. Postoperative data included total foley duration, postoperative foley duration, need for straight catheterization, and need for foley replacement. Total foley duration was defined as the start of the operative case to initial foley removal. Postoperative foley duration was defined as the end of the operative case to initial foley removal.
In our study, POUR was defined as the inability to micturate and the need for a straight catheterization and/or foley replacement postoperatively. The need for straight catheterization was determined by time since foley removal, development of retention symptoms, and/or bladder distention identified on bladder scan. In our practice, if a patient has not voided 6 to 8 hours after foley removal, or develops symptoms of retention, a bladder scan will be performed. Patients with bladder distention will undergo straight catheterization. The cycle will then repeat and straight catheterization is usually performed twice before proceeding with foley replacement for persistent retention. The number of hours between foley removal and first straight catheterization (or between the first and second straight catheterization) was not reported due to variability in patient care.
The primary outcomes analyzed were the need for straight catheterization and the need for foley replacement. A secondary outcome included the incidence of CAUTIs. We evaluated the demographics, preoperative, intraoperative, and postoperative variables for associations with these outcomes.
Statistical Analysis
Univariable analysis was performed using Wilcoxon Rank Sum and Fisher Exact tests. Total foley duration and postoperative foley duration were dichotomized by the median and by 24 hours to assess for associations with straight catheterization and foley replacement. Multivariable logistic regression was performed to evaluate for a relationship between BMI and intraoperative fluid volumes. A P-value of <.05 was used to determine statistical significance.
Results
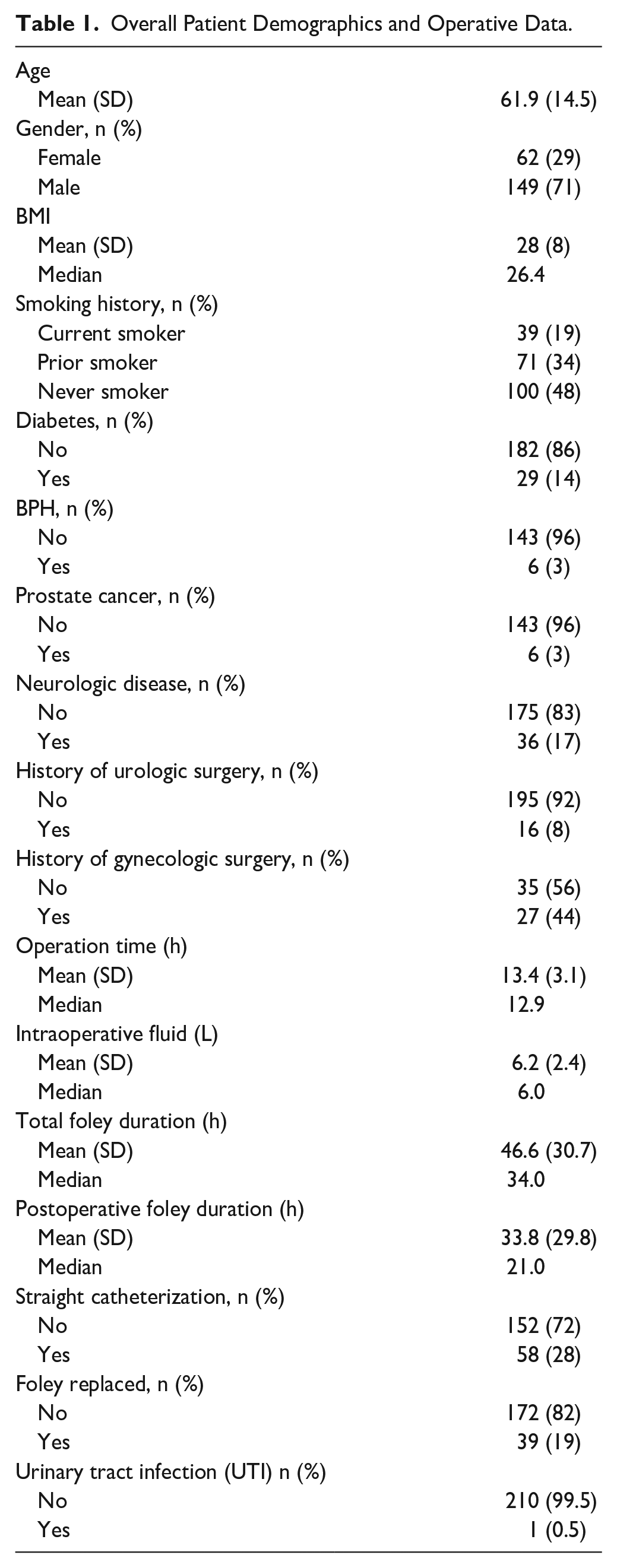
Overall patient demographics, intraoperative data, and postoperative data are shown in Table 1. Median operative time was 12.9 hours and median interoperative fluid volume was 6 l. Mean total foley duration was 44.6 ± 30.7 hours with a median of 34 hours. Mean postoperative foley duration was 33.8 ± 29.8 hours with a median of 21 hours. Overall, 58 patients (28%) required straight catheterization after foley removal, and 39 patients (19%) required foley replacement. Only 1 patient (0.5%) developed a CAUTI. This patient had a total foley duration of 4 days and required foley replacement for urinary retention. A total of 16 patients were put on alpha blockers (Tamsulosin or Doxazosin) postoperatively due to POUR. Of these 16 patients, 12 required foley replacement.
Overall Patient Demographics and Operative Data.
The analysis of patients who required straight catheterization secondary to POUR is shown in Table 2. Age, gender, BMI, smoking history, comorbidities, operation time, and intraoperative fluid volume did not influence POUR requiring the need for straight catheterization. Shorter total foley duration (median: 30.5 hours vs 34.5 hours, P = .04) and postoperative foley duration (median: 18.0 hours vs 23.5 hours, P = .01) were statistically significant for POUR requiring straight catheterization. Neither the dichotomized total foley duration nor dichotomized postoperative foley duration showed statistical significance. Of the 58 patients who required straight catheterization, 35 patients (60%) required a foley replacement (P < .0001).
Need for Straight Catheterization.
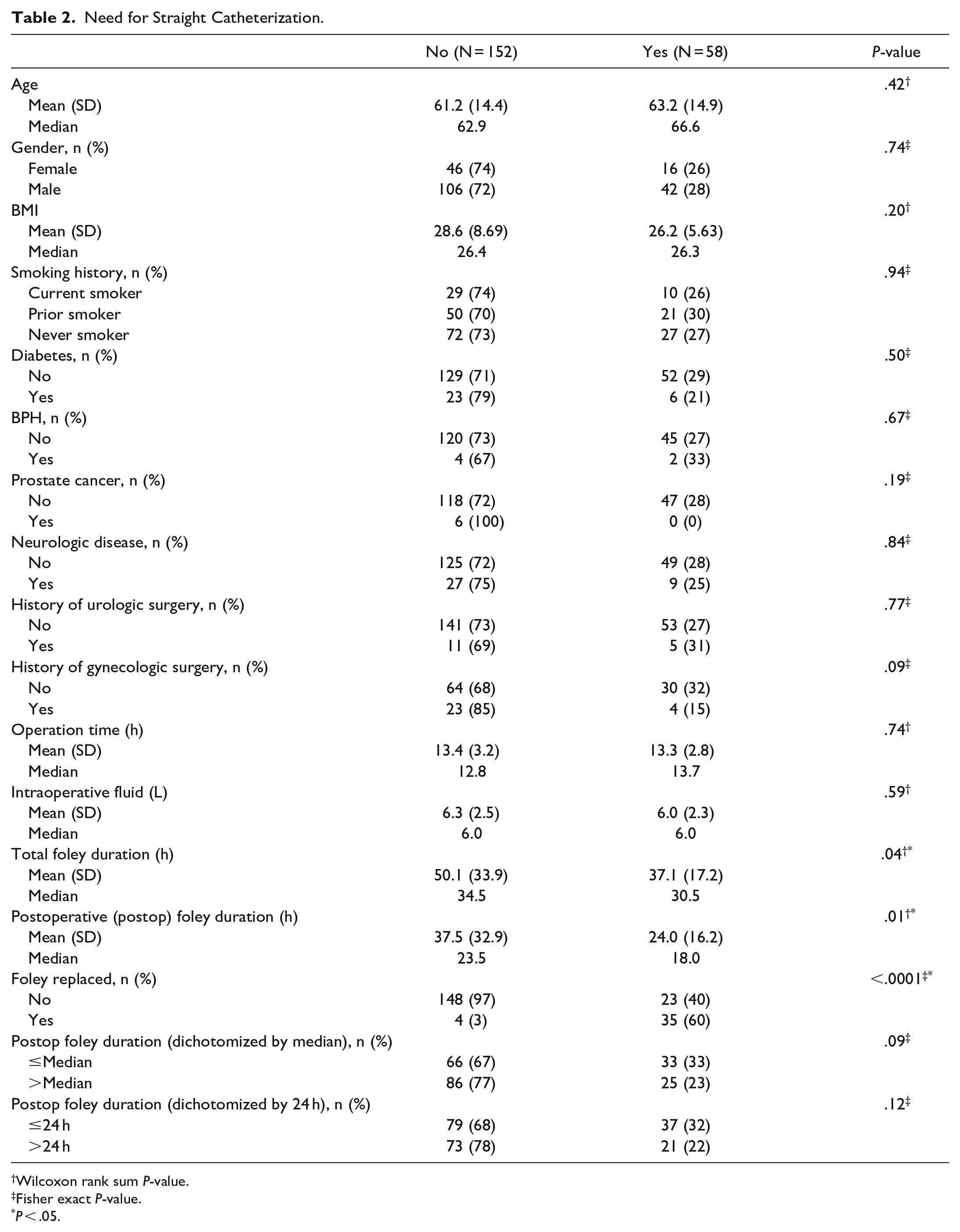
Wilcoxon rank sum P-value.
Fisher exact P-value.
P < .05.
The analysis of the patients who required foley catheter replacement secondary to POUR is shown in Table 3. Age, BMI, intraoperative fluid volumes, and straight catheterization showed statistical significance for POUR requiring foley replacement. Median age of patients who required foley replacement was higher than those who did not require replacement (69.5 years vs 62.0 years, P = .03). BMI was lower in patients who required foley replacement compared to those who did not require replacement (median: 24.6 vs 26.6, P = .03). The intraoperative fluid volume was lower in patients who required foley replacement compared to those who did not require replacement (median: 5.3 L vs 6 L, P = .03). Total foley duration in patients requiring foley replacement was not statistically significant (median: 32 hours vs 34 hours, P = .42). Postoperative foley duration in patients requiring foley replacement was not statistically significant (median: 20 hours vs 22 hours, P = .13). Of the 39 patients who had a foley replacement, 35 (90%) patients required a straight catheter prior to replacement (P < .0001).
Need for Foley Replacement.
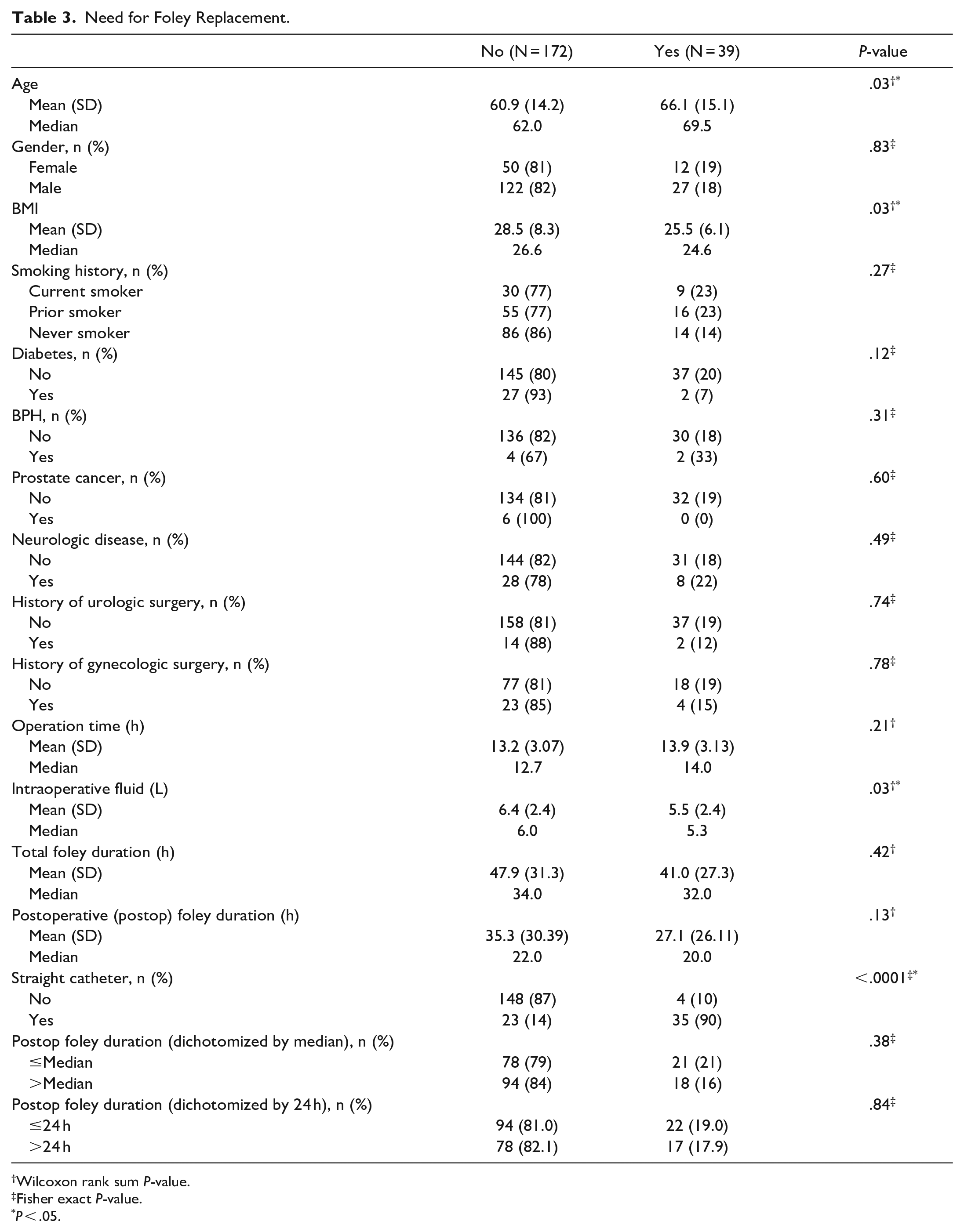
Wilcoxon rank sum P-value.
Fisher exact P-value.
P < .05.
The multivariate logistic regression showed that both BMI and intraoperative fluid volumes were statistically significant even after adjustments (Table 4).
Multivariate Logistic Regression.
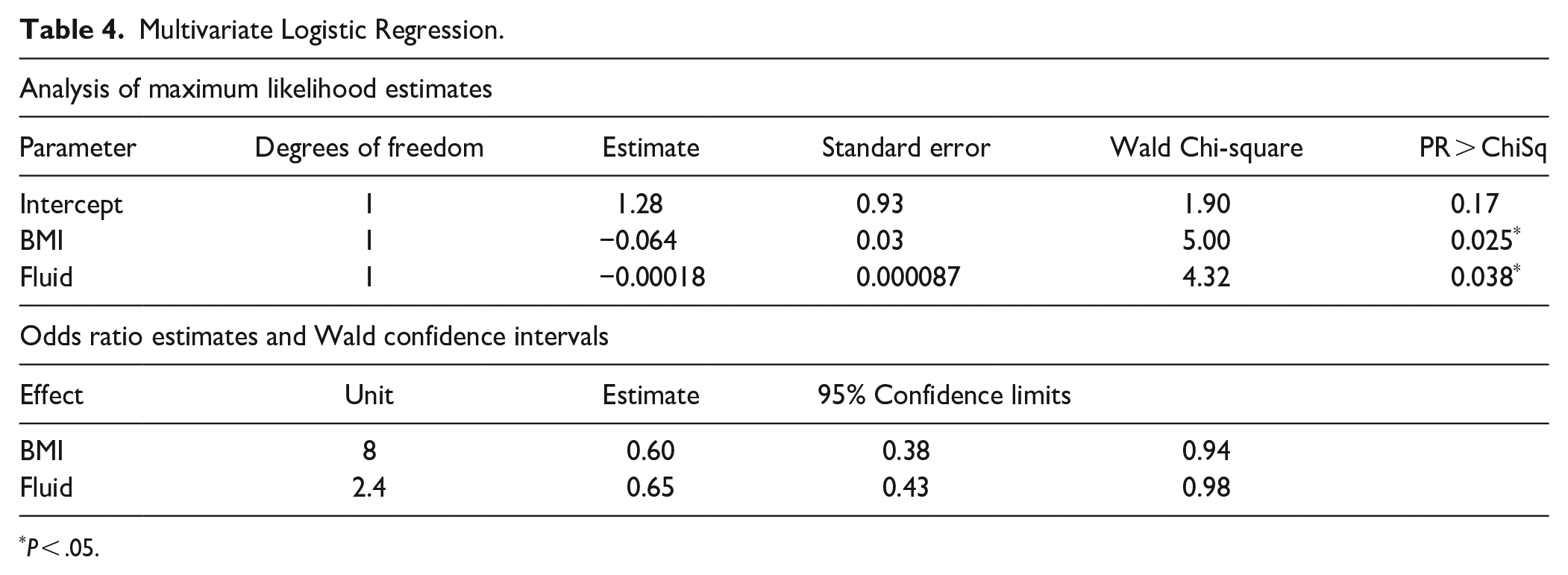
P < .05.
Additional parameters, such as smoking duration, alcohol use, and history of hypertension, were analyzed but were not statistically significant with regard to straight catheterization and foley replacement.
Discussion
POUR is a common urologic complication across many surgical specialties. While studies applying the ERAS pathway for head and neck oncologic surgeries exist, they do not focus on postoperative urinary complications.9,10,12 Low et al 9 was the only study that provided specific data on foley duration. The authors reported an average foley duration of 1.7 ± 1.5 days after surgery, with a majority of foley catheters removed on POD 1. Foley replacement for POUR occurred in 8% of patients. 9 Our study had a lower mean postoperative foley duration of (1.4 ± 1.2 days) and a higher rate of foley replacement at 19% (Table 1). However, our study could not be fully compared to Low et al 9 since the paper did not discuss the criteria for foley replacement, rate of UTIs, or if straight catheterization was required. To our knowledge, this is the first study in the literature specifically analyzing the optimal timing of foley removal and the factors influencing urinary complications after head and neck free flap reconstruction.
Risk factors for POUR requiring foley replacement in our study were older age, lower BMI, lower intraoperative fluid volumes, and need for straight catheterization (Table 3). The 4% rate of BPH in our study was much lower than the 50% to 75% rate reported in the literature for men greater than 50 years old. 13 This can be explained by severe underreporting and undiagnosed BPH in our patient population. Not all patients who required straight catheterization were put on alpha blockers postoperatively. While alpha blockers are part of the protocol for patients who require straight catheterization, there was patient variability and deviation from the protocol. Anesthesia itself can affect POUR. 1 Although we did not analyze the differences in anesthetics given, we confirmed with our anesthesiologists that, in general, there was little deviation from the anesthetic protocol for free flap patients. This protocol involved a combination of induction propofol, muscle paralytic, and gas anesthetic. While the literature supports older age as a risk factor for POUR, conclusions on BMI and intraoperative fluid volumes are varied.1,3,4,14 -19 Through a multivariate logistic regression model, we found lower BMI and lower intraoperative fluid volumes to be independent risk factors for POUR requiring foley replacement (Table 4). Studies have found an association between lower BMI and increased risk of POUR, but the mechanism behind this remains unclear.17 -19 Further investigation is needed regarding BMI as a risk factor for POUR in head and neck free flap reconstructions.
Studies have found intraoperative fluid volumes >750 ml to increase the risk of POUR.14 -16 However, patients in these studies did not have a foley catheter due to their much shorter procedure lengths (average 2 hours) and the etiology of POUR was related to bladder overdistention. Therefore, the results cannot be compared with our study.14 -16 Studies have found operative time and duration of anesthesia over 200 minutes to be risk factors for POUR in spinal and neurosurgical procedures.20,21 However, this is not comparable to our study, as operative duration was longer than 200 minutes in all cases. Literature regarding POUR after longer surgical cases, and analysis of intraoperative factors such as intraoperative fluid volumes, is sparse regardless of the surgical specialty. Our study suggests that larger volumes of intraoperative fluid may decrease the risk of POUR. However, strong conclusions cannot be drawn from this as we did not monitor postoperative fluid volume before and after foley removal. Further investigation into both intraoperative and postoperative fluid resuscitation and its effect on POUR is necessary.
Neither the total nor postoperative foley duration was a risk factor for POUR requiring foley replacement (Table 3). The dichotomized results were not statistically significant for foley replacement (Table 3). Based on this data, no conclusions could be made on an ideal timeframe for foley removal to decrease the risk of foley replacement. The results did not support or oppose the ERAS recommendations of foley removal within 24 hours after surgery. 12 However, what should be considered is the need for straight catheterization as a predictor (P < .0001, Table 3).
To minimize the risk of POUR requiring foley replacement, efforts should be made to reduce the risks for straight catheterization. As shown in Table 2, the only risk factors for POUR requiring straight catheterization were shorter total (P = .04) and postoperative (P = .01) foley durations. Patients who were straight catheterized had a median postoperative foley duration of 18 hours compared to 23.5 hours for patients who were not straight catheterized (P = .01, Table 2). Of the patients who had foley removal <24 hours, 32% required straight catheterization compared to 22% of patients who had foley removal >24 hours postoperatively. Similar results were found when analyzing by the median value of 21 hours postoperatively. Neither dichotomized results were not found to be significant to a P < .05 but trended toward significance, which may be limited by our sample size. Our data did not support the ERAS recommendations for foley catheter removal <24 hours after surgery. 12 This was an important finding since the ERAS recommendations for head and neck patients were based mostly on gynecologic literature as well as some thoracic and abdominal literature. 12 Our study suggests that postoperative care of urinary catheters in head and neck patients may differ from the care for patients undergoing other procedures. Additionally, there may be limitations on extrapolating data from gynecologic procedures onto urinary catheter care for head and neck surgeries. Based on our data, we suspect the optimal foley removal time to reduce the risk of requiring straight catheterization to be between 21 and 48 hours postoperatively. Further investigation with a larger cohort will assist in defining this timeframe.
If foley duration is prolonged, we risk increasing the rates of CAUTIs.1,22,23 In head and neck patients, CAUTIs have been associated with increased postoperative complications. 12 Despite our overall mean postoperative foley duration being >24 hours (33.8 hours, Table 1), our results did not show an increased rate of CAUTI (0.5%) (Table 1). This result was lower than the CAUTI rates reported in the literature for patients undergoing head and neck free flap reconstruction, which ranged from 1.2% to 6.2%.23,24 The one patient in our study who developed a CAUTI had an initial foley duration of 4 days to accurately monitor fluid balance. On day 4, the patient was discovered to have a CAUTI, which prompted foley removal.
Limitations
The results of this study were limited by the data available through retrospective chart review. For patients who had multiple surgeries, only the initial procedure was included. Medications (eg, anticholinergics, beta-blockers, sympathomimetics) may affect rates of POUR but were not specifically analyzed in our study.1,4 Postoperative fluid volumes were not collected nor analyzed but could be a factor that affects POUR. Additionally, other factors may have necessitated prolonged foley duration, such as prolonged ventilation or medical comorbidities requiring accurate monitoring of postoperative fluid balance. Older age was associated with POUR but subgroup analysis was not performed due to the small sample size. POUR can prolong the length of hospital stay, but this was not analyzed in this study since the focus was to evaluate factors that affect POUR. In addition, the data and its interpretation reflect the practices of a single institution. Further investigation into other factors that may contribute to the increased risk of POUR is warranted.
Conclusion
Standardized pathways, such as the ERAS pathway, have recommended early foley removal for preventing CAUTIs. However, earlier foley removal may be increasing the risk of POUR without having a significant effect on CAUTI in head and neck free flap reconstruction surgeries. Our data demonstrated a low incidence of CAUTI with an average postoperative foley duration exceeding 24 hours. While early catheter removal remains a key strategy in lowering CAUTIs, further studies should consider balancing the risk of CAUTI with the risk of POUR when considering foley removal. Given the differences in case length, intraoperative fluid resuscitation, and other parameters associated with head and neck reconstructive surgeries, different strategies relating to catheter management may need to be considered. Our study supports foley removal between 21 and 48 hours postoperatively to reduce POUR, but additional investigation with larger sample sizes will further define this. We do not suspect implementing a longer foley duration would negatively impact the rate of CAUTI in patients with head and neck pathology undergoing free flap reconstructive surgery.
Footnotes
Authors’ Note
Data in this article was presented as a poster at the AAO-HNS 2020 Virtual Annual Meeting, September 12-14, 2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.