
Abstract
Vascular sequelae following (SARS-CoV-2 coronavirus disease) (COVID)-19 infection are considered as “Long Covid (LC)” disease, when occurring 12 weeks after the original infection. The paucity of specific data can be obviated by translating pathophysiological elements from the original Severe Acute Respiratory Syndrome-Corona Virus (SARS-CoV-2) infection (In a microcirculatory system, a first “endotheliitis,” is often followed by production of “Neutrophil Extracellular Trap,” and can evolve into a more complex leukocytoklastic-like and hyperimmune vasculitis. In medium/large-sized vessels, this corresponds to endothelial dysfunction, leading to an accelerated progression of pre-existing atherosclerotic plaques through an increased deposition of platelets, circulating inflammatory cells and proteins. Associated dysregulated immune and pro-coagulant conditions can directly cause thrombo-embolic arterial or venous complications. In order to implement appropriate treatment, physicians need to consider vascular pathologies observed after SARS-Cov-2 infections as possible “LC” disease.
Introduction
Considering the extended studies about (Severe Acute Respiratory Syndrome-Corona Virus, SARS-CoV-2, disease) (COVID)-19 infection and its chronic complications, the present commentary draws attention to the vascular aspects “Long COVID” (LC), which, although infrequent, must not be unrecognized. Due to the scarcity of clinical and laboratory evidence available, we approached this topic by translating well-known elements from the original disease.
Long COVID (defined as occurring 12 weeks after the original infection) is characterized by symptoms lasting for many months in subjects who have had a severe, moderate, or mild form of COVID-19.1-4
The most common symptoms are persistent fatigue, shortness of breath, tachycardia and palpitations, anosmia, muscle weakness, brain fog, headache, vomiting and nausea, fever, and skin rash.3,5
The persistence of COVID-19 symptoms has been reported in several studies. The persistent symptoms have been frequently reported. 6 Huang and coworkers 6 evaluated 1733 patients (nearly half were men) in Wuhan, China. With a median follow-up of 186 days, 76% of the patients reported at least one persistent symptom, especially in women. The most reported symptoms were muscle weakness and fatigue (63%), followed by sleep difficulty (26%), and anxiety/depression (23%). 6
As highlighted by the consensus document published by the American College of Cardiology in patients with COVID-19 myocarditis, the most common symptoms are fever, dyspnea, cough, and chest pain. 7 Other symptoms include different types of chest discomfort, post-exertional fatigue, palpitations, and syncope. 7 Although symptoms may resolve within 3 months after the initial diagnosis, sometimes the persistence of symptoms can last >12 months. 7
According to previous descriptions, disorders related to almost any organ system can occur in individuals with post-COVID-19 syndrome, making symptom classification a challenging task in clinical practice. 8 However, neurological and/or neuropsychological deficits such as memory loss, “brain fog,” fatigue, dizziness, headache, or generalized pain are frequent complaints. 8 Interestingly, damage to the central or peripheral nervous system can only rarely be objectified or, if present, is attributable to a distinct neurological disease rather than the post-COVID-19 syndrome. 9 Fleischer and coworkers 9 found evidence of significant psychiatric comorbidities and high levels of somatization, indicating the possibility that psychosomatic mechanisms such as somatosensory amplification may play a substantial role in the pathogenesis of the post-COVID-19 syndrome. 9
Long COVID progression is related to different risk factors such as aging, asthma, obesity, poor pre-pandemic general health, and female sex. In fact, the young and/or women show higher risk to develop LC than men, but the risk level becomes similar around 60 years old.5,10 Formally, the COVID-19 sequelae can be distinguished in “prolonged post-acute COVID-19 pathologies,” if observed between the 4th and 12th week from the initial viral infection healing.10,11 Non-specific bridge symptoms can be common with other viral infections, such as mild discomfort, weakness, headache, pain in the joints, while other specific signs, inherent to a previous SARS-CoV-2 disease include cough, exertional dyspnea, chest pain, dysgeusia, and anosmia.
A recent population study found that individuals infected with SARS-CoV-2 Omicron (B.1.1.529) variant had a similar risk of post-COVID complaints (fatigue, cough, heart palpitations, shortness of breath, and anxiety/depression) as individuals infected with Delta (B.1.617.2), from 14 to up to 126 days after testing positive, both in the acute (14 to 29 days), sub-acute (30 to 89 days), and chronic post-COVID (≥90 days) phases. However, at ≥90 days after testing positive, individuals infected with Omicron had a lower risk of having any complaint (43 (95% confidence interval (CI) 14–72) fewer per 10,000), as well as a lower risk of musculoskeletal pain (23 (95% CI = 2–43) fewer per 10,000) than individuals infected with Delta. The authors suggested that the acute and sub-acute burden of post-COVID complaints on health services is similar for Omicron and Delta. 12
Several works have focused on the importance of myocardial damage and the close relationship with the LC syndrome; in contrast, the evidence on vascular damage present during LC is still scarce.7,13,14
The aim of the present commentary is to consider vascular damage during LC and to design a pathway that from pathophysiological aspects leads to the clinic. This should facilitate the diagnosis and management of vascular LC.
Basal Pathophysiological Elements
Inflammatory Status
Severe Acute Respiratory Syndrome-Corona Virus infection causes both endothelial damage and an inflammatory response characterized by immune cells activation leading to high expression of pro-inflammatory cytokines, such as interleukin-1b (IL-1 b), interleukin-6 (IL-6), and tumour necrosis factor (TNF)-alpha; in severe COVID-19 cases, an over-reaction of the innate immune response, with massive release of pro-inflammatory cytokines (cytokine storm) is observed.
15
(Figure 1). Diagram describing the pathway from acute COVID-19 infection to microvascular thrombosis and risk of worsening of atherosclerosis.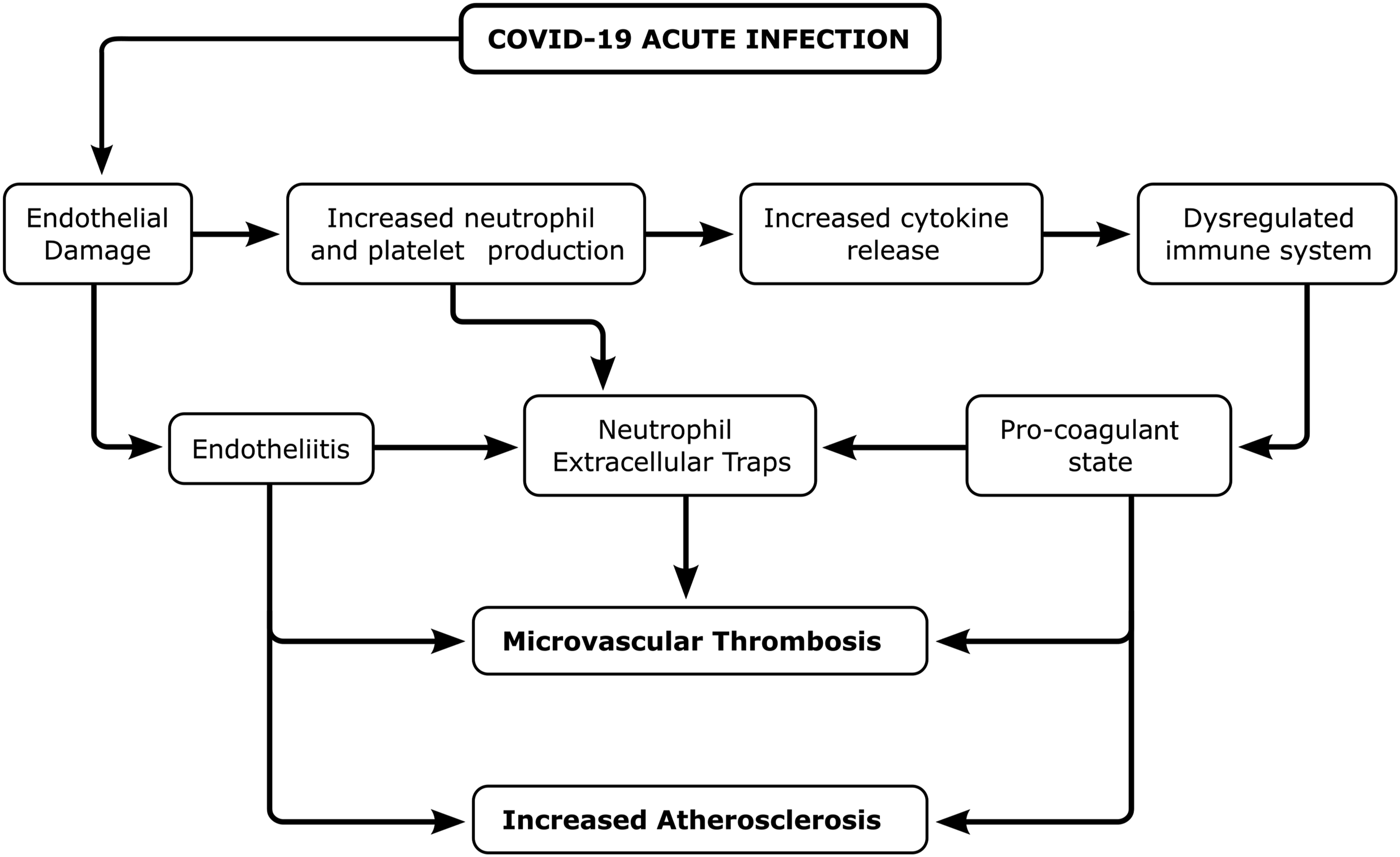
Cytokine storm is also associated with the activation of coagulation pathways during the response to infection, with an imbalance between pro- and anti-coagulant factors, micro thrombotic events, disseminated intravascular coagulation, and multiorgan failure.16,17 An excessive acute response or the persistence of the systemic inflammation, linked to several cardiovascular, metabolic, and neurodegenerative diseases, pathologies of the musculoskeletal system, cancers, and depression, could be also responsible for the symptoms of LC and the consequent organ damage.17-19
Endothelial Damage
Cardiovascular complications are common in patients with LC, due to alterations in the vascular environment, promotion of adhesion and blood pro-coagulation.19,20
Several studies have reported the onset of vasculitis syndromes in COVID-19 patients, with histologic evidence also in the liver, lung, skin, or kidney.19,21 The main pathophysiologic observations can be detected in small/medium sized arteries, and is initially characterized by an acute endotheliitis, evolving into a hypersensitive acute vasculitis. 22
Specifically, binding between angiotensin converting enzyme 2 (ACE2), expressed in vascular endothelial cells, and SARS-CoV-2 spike protein during infection provokes the activation of inflammatory pathway that promotes micro- and macrovascular endothelial dysfunction and damage. 23
Another possible mechanism that can link SARS-CoV-2 to inflammation of the endothelium is the release of type I interferons (IFN) caused by the involvement of cyclic guanosine monophosphate–adenosine monophosphate synthase (GMP-AMP), (cGAS)-stimulator of interferon genes (STING) inflammatory pathway, determined by mitochondrial dysfunction.23,24 Different studies showed that SARS-CoV-2 impairs mitochondrial function in several cell types.24,25 As far as endothelial cells are concerned, the activation of the cGAS/STING pathway is determined by the mitochondrial DNA, the small, circular mitochondrial own genome present in multiple copies per cell.24,25 Due to their endosymbiotic origin from ancestral bacteria, mitochondria possess an own genome, which resembles bacterial DNA in many features, such as the presence of hypomethylated C-phosphate-G regions. For this reason, mitochondrial DNA (mtDNA) can be sensed as a “foreign” molecule by receptors that normally detect viral or bacterial DNA, such as toll-like receptor-9 (TLR-9), NLR family pyrin domain containing 3 (NLRP3) inflammasome and cyclic GMP-AMP synthase (cGAS).26-28 It has been demonstrated that endothelial cells infected by SARS-CoV-2 produce high levels of type I IFNs. Mechanistically, this phenomenon is caused by the release of endogenous mtDNA from dysfunctional mitochondria, where it is normally present, in the cytosol, where it can be recognized by cGAS as a “misplaced” DNA molecule. Then cGAS activates STING, which, in turn, leads to the transcription of type I IFN genes. 29
Pro-Coagulant Status
This multifactorial pathological condition has been associated with alteration of the coagulation cascade, higher complement level, plasminogen activating factor I, and von Willebrand factor, leading to increased tissue factor expression in response to inflammatory cytokines, microvascular dysfunction, and promoting thrombotic events occluding vessels locally.22,23,30-33
About the COVID-19-induced micro-vascular lesions, we retrieved some fundamental pathophysiological data. Firstly, a widespread presence of ACE2 endothelial receptors favors direct virion penetration inside the vascular endothelium during the COVID-19 viremic phase, causing an “endotheliopathy,” that is expressed by an accelerated necroptosis, or increased endothelial dysfunction.34,35 Apoptosis and necroptosis are major mechanisms of cell death that typically result in opposing immune responses. Apoptotic death usually leads to immunologically silent responses, whereas necroptotic death releases molecules that promote inflammation, a process referred to as necroinflammation. 36 Thus, the accelerated necroptosis of infected endothelial cells can cause the release of Damage Associated Molecular Patterns (DAMPs, such as high mobility group box-1 protein, mitochondrial proteins, ATP among others) along with pathogen-associated molecular patterns (PAMPs, such as viral particles), which in turn are recognized by cells of the innate immune system, leading to the production of pro-inflammatory cytokines. 37 Secondly, a dysregulated activation of the immune system entails an over-production of immune/inflammatory cells, leading to endotheliitis. 34 This process also causes, besides an abundant release of cytokines, a considerable production of “neutrophil extracellular traps” (NET). Neutrophil extracellular traps consist of DNA fragments that, once extruded from neutrophils and bound to histones, inflammatory proteins, and activated platelets, can contribute to specific microcirculatory damage.38,39 Thirdly, a hyper-production of platelets, generated by megakaryocytes observed even in the pulmonary parenchyma, triggers microcirculatory hyper-coagulation. 40 Finally, the adaptive cell-mediated immune system, if abnormally activated, can lead to a more severe hypersensitive “leukocytoclastic vasculitis,” with an abnormal production of antibodies and auto-antibodies. This aggravates the already present hyper-coagulant state, leading to an antiphospholipid-like syndrome, further underlining the strong links between hyper-coagulation and inflammation (Figure 1).17,41
Recently, the neutrophil-platelet axis has been invoked as an additional damaging mechanism involved in COVID-19 disease. Platelets and neutrophils cooperate as mobile overseers to maintain host integrity and to protect against sterile and infectious injury. In pathological conditions, however, this liaison of platelets and neutrophils can be harmful, resulting in thrombo-inflammatory processes that can lead to lethal thrombotic events.42,43
Clinical Aspects of Vascular LC
We thought that some COVID-19 pathophysiological elements can also affect the peripheral vascular system, in particular, viral action against the endothelium, and the activated immune system with its associated hyper-coagulant state that characterized the acute phase of the disease.7,41,44 By analogy, these fundamental protagonists, the virion load, and the adaptive immune reaction, when affecting cardiomyocytes instead of endothelial cells, promote an equivalent necroptosis, and a lymphocytic myocardial infiltration in place of a vasculitis.45,46 It follows that in the arterial system consisting of medium/large-sized arteries, the long-term effects of COVID-19 primarily induce endothelial dysfunction, sometimes becoming evident through an accelerated progression of pre-existing atherosclerotic lesions. This correlates with an augmented deposition on pre-existing atherosclerotic plaques of conglomerates of abnormal inflammatory proteins, circulating inflammatory cells, platelets, and lipid-laden macrophages.46,47,48,49 Moreover, the same endothelial damage, associated with an abnormal immune-inflammatory response, can involve normal arterial walls, where circulating immune-inflammatory cells, neutrophils, lymphocytes, and macrophages, favor dispersion of smooth muscle cells from the medial layer, and their migration to intima, attempting to replace the lost endothelial cells.2-33,50-52 In a hyper-coagulant milieu, both these factors directly lead to vascular thromboses, mainly venous, but also arterial (Figure 2). In most cases, all the elements of Virchow’s triad are fulfilled: endothelial damage, hyper-coagulant state, and the altered blood dynamics, consisting in partial obstructions and/or aneurysms. In our opinion, the other cases confirm the outstanding impact of the endothelial damage, and the associated micro-thrombosis, which beginning in the acute phase of the COVID-19 disease, can progress all over the interval time before the LC, until the onset of a clinically evident arterial thrombosis. This long course agrees with histopathology of thrombi retrieved in course of embolectomies, demonstrating an organized inner texture, and a well-developed network of endothelium-lined microvessels.17,22,50 Thrombosis of the extra-parenchymal splenic artery in a COVID-19 patient (Hematoxylin-Eosin staining). (A) The external part of the medial layer, infiltrated by inflammatory circulating cells, indicates an acute arteritis; inside a recent, non-recanalized thrombus [10X]. (B) Cordons of inflammatory cells, intercalated with bands of smooth muscle cells, containing lymphocytes, macrophages, and mainly neutrophils [40X].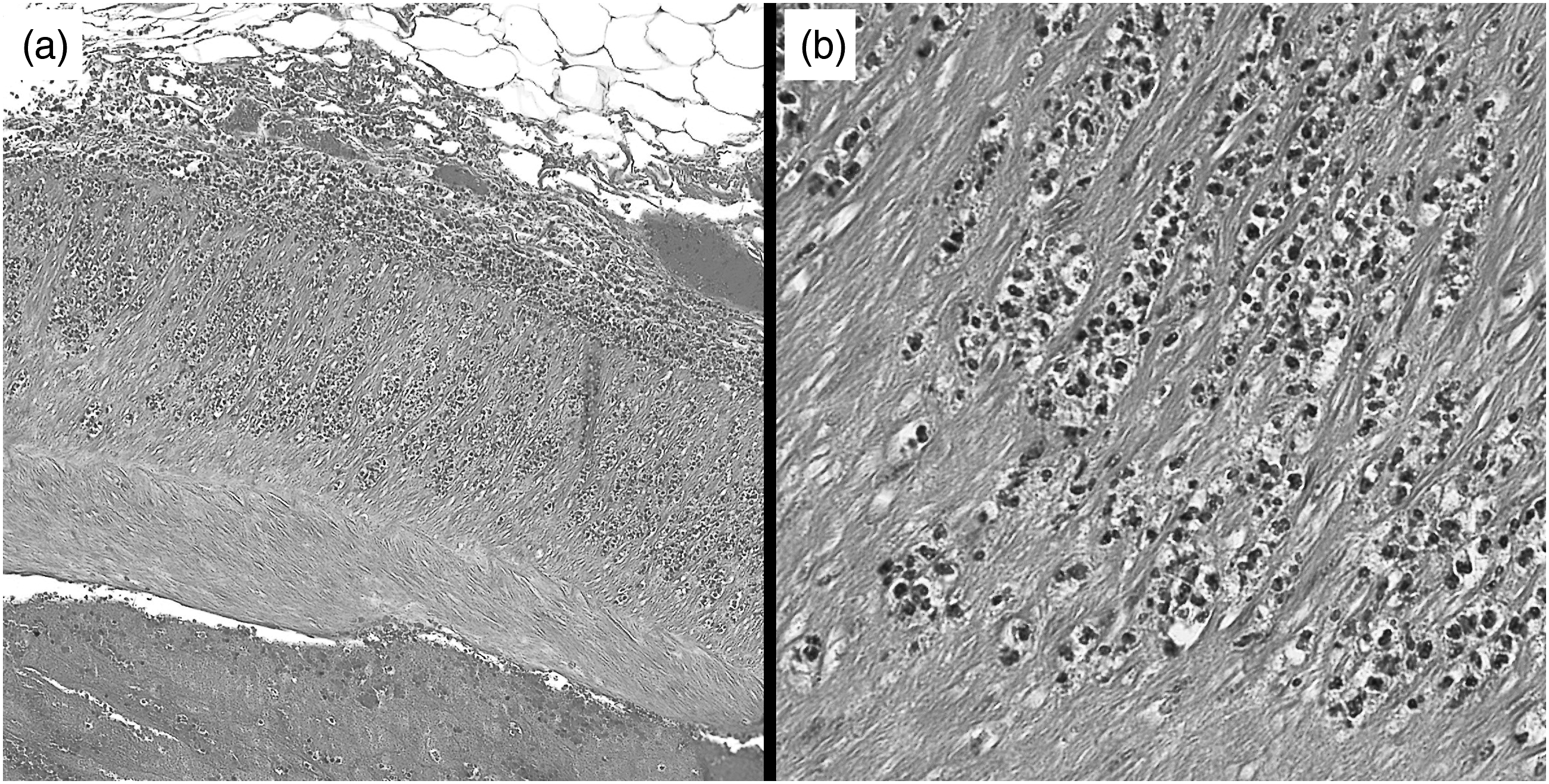
Aortic aneurysms can also have a more rapid increase in size, with an inherent increased risk of rupture. In a hyper-coagulant condition, this can be correlated with vasa vasorum thrombosis, and an accelerated increase of the intraluminal thrombus, that, by tightly adhering to the aneurysm walls, aggravates parietal hypoxia.17,51 The consequent great release of oxygen reactive species, and the high oxidative stress further damage the aneurysm walls, already submitted to an inflammatory process, atherosclerosis correlated.17,22,50 In addition, the typical COVID-19 circulating inflammatory cells, penetrating inside the aneurysm thrombus, get in contact with extraneous molecules present in the aortic atherosclerotic plaques, such as cholesterol crystals and calcium compounds, further increasing the local inflammatory reaction, and release of elastases and metalloproteinases.17,22,50,51 In turn, these proteases promote digestion of collagen and elastin components of the aortic medial tunica, favoring dispersion of the smooth muscle cells, and their accelerated necroptosis
52
(Figures 2 and 3). Coronary arteries can also be expected to manifest a similar LC pathology, expressing a greater risk of obstruction.
53
Diagram suggesting the pathway leading to vascular thrombosis and aortic aneurysm worsening in Long Covid.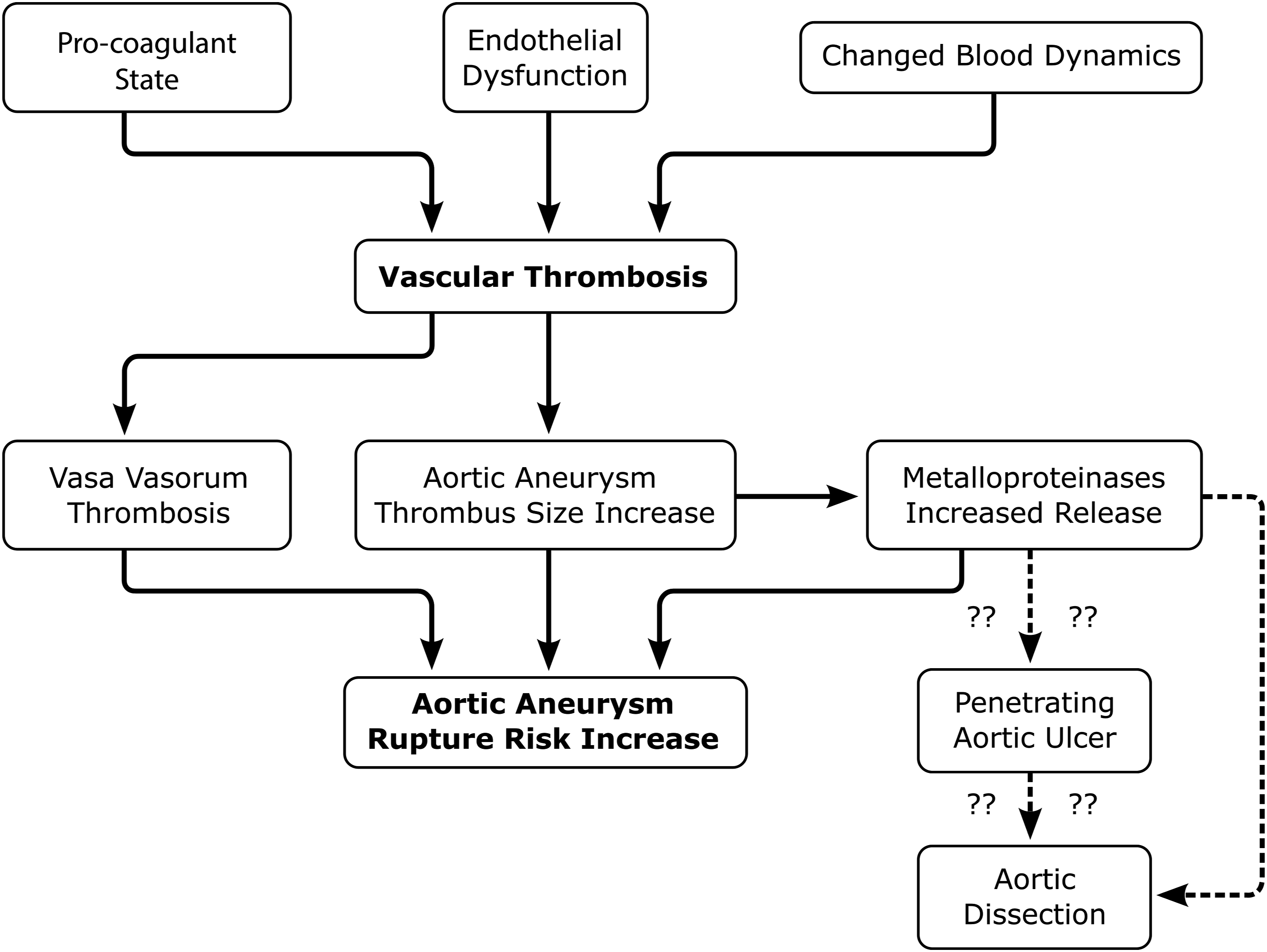
Conclusions
We propose this deductive/translational study method in order to define vascular LC, as a possible complication of SARS-CoV-2 infection, and to facilitate the diagnostic process. Limitations to our research are represented by the patients’ unknown immunological assessment, acting as a possible predisposing factor, and the time extension of these sequelae, is not yet established.52-54
Many people have been infected by SARS-Cov2, so any association might remain circumstantial without additional molecular evidence. Also, we are currently battling against new variants, that is, Omicron variants showing potential differences in the LC clinic and symptoms compared with the Delta variants. 12 COVID-19-associated vascular pathologies, if recognized early, can be an indication for adequate preventive measures, mainly when surgical open or endovascular procedures become necessary. Similarly, unexpected vascular thromboses, worsened pre-existing atherosclerotic lesions, or rapidly increased in size of an aortic aneurysm, could advise physicians to search for possible associations with a recent SARS-Cov-2 infection.
Prevention of Vascular Long-COVID
To prevent vascular LC, it is necessary to identify the predisposing risk factors so as to stratify risk in each patient. The scenario is changing following the introduction of vaccines that have modified the response to the virus and following the development of subsequent variants. The framework determined by the Delta variant is different from that determined by the Omicron variant. However, it is necessary to pay attention to the involvement of the vascular system in LC syndrome to avoid neglecting this aspect.
Further studies dedicated to the evaluation of vascular function in patients with LC are needed in order to adopt appropriate strategies for patients.
Footnotes
Author Contribution
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and, (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.