
Abstract
Background
Rib fractures in elderly trauma patients carry increased morbidity and mortality. Prior guidelines recommended indiscriminate intensive care unit (ICU) admission for patients ≥65 years with ≥3 rib fractures. In 2024, our institution implemented the Rib Injury Guideline (RIG) score, a novel triage and disposition tool, through a standardized smartphrase (SP).
Methods
We retrospectively reviewed trauma patients ≥65 years with ≥1 rib fracture admitted between 1/1/2020 and 7/5/2025. Patients admitted before 10/31/2024 (pre-RIG) were compared to those admitted after (post-RIG). Primary outcomes were ICU admission and unanticipated ICU upgrade. Secondary outcomes included mortality, ICU and hospital length of stay (LOS), and compliance with the RIG SP.
Results
546 patients were included, with a median age of 80 years and median Injury Severity Score (ISS) of 10. There were 462 (85%) patients pre- and 84 (15%) post-RIG. ICU utilization significantly decreased in the post-RIG cohort (61% vs 37%, OR 0.38, P < 0.01), with an even greater reduction among patients with multiple rib fractures (67% vs 38%, OR 0.29, P < 0.01). Unanticipated ICU upgrade was 1% for both groups (P > 0.99). ICU LOS (median 2 vs 3, P = 0.17), hospital LOS (median 6 vs 6, P = 0.65), and mortality (4% vs 5%, P = 0.55) were similar between cohorts. Compliance with the SP was 82%.
Discussion
Implementation of the RIG score with an integrated smartphrase substantially reduced ICU admissions in elderly rib fracture patients without compromising patient safety, as evidenced by the absence of increased rates of ICU upgrades and no impact on mortality.
Keywords
Key Takeaways
• The Rib Injury Guidelines (RIG) score was associated with lower ICU admission rates while preserving patient safety. • Simultaneous use of an integrated smartphrase (SP) within the EMR facilitated broad adoption and standardized clinical decision making.
Introduction
Rib fractures are among the most common injuries seen in trauma patients worldwide and are virtually omnipresent in blunt thoracic trauma patients, carrying significant morbidity and mortality.1–3 Elderly patients are disproportionately affected by rib fractures, with higher rates of pneumonia, intensive care unit (ICU) admission, mechanical ventilation, and death than their younger counterparts.4,5 Based on projections from the latest United States (US) Census Bureau data, we can expect that the elderly population in the US will continue to grow, surpassing 80 million individuals in the year 2050 and accounting for almost one quarter of the US population. 6 The combination of our aging population with the mortality risk that elderly rib fracture patients face illustrates one way in which our health care system is becoming increasingly strained. 7 Due to this strain, numerous triage tools and scoring systems for rib fractures have been developed to help identify patients that are most at risk for poor clinical outcomes. These scores differ in their levels of complexity and the variety of factors considered. For example, the Rib Fracture Score (RFS) considers age, number of rib fractures, and presence of bilateral rib fractures. On the other hand, scores like the Thoracic Trauma Severity Score (TTSS) and the Battle score take physiologic data like oxygen saturation into consideration on top of number of rib fractures.8–10 Though many different triage tools are able to identify high-risk patients with accuracy, practice guidelines are equally important tools designed to standardize care and improve efficiency in health care systems.11,12
Our institution, an urban Level I trauma center, evaluates more than 300 adult patients with rib fractures annually. Based on the Western Trauma Association (WTA) guideline, our management approach for elderly patients 65 years or older with 3 or more rib fractures was indiscriminate ICU admission.
13
We observed, however, that many of these ICU admissions were transitioned to a lower level of care within 24 to 48 h, raising the question of whether universal ICU admission criteria optimally allocate ICU resources in the absence of early physiologic compromise. During this same period, several triage tools and practice guidelines were published that combined elements from existing scoring systems with incentive spirometry measurements to identify high-risk patients and guide clinical decision-making.14–16 Using the framework proposed by Nelson et al (2022), we implemented the Rib Injury Guidelines (RIG) score at our institution in October 2024. Within our electronic medical record (EMR), we created a smartphrase (SP) to be used in the initial consultation or history and physical completed by the admitting trauma surgery service (Figure 1). An example of the RIG SP.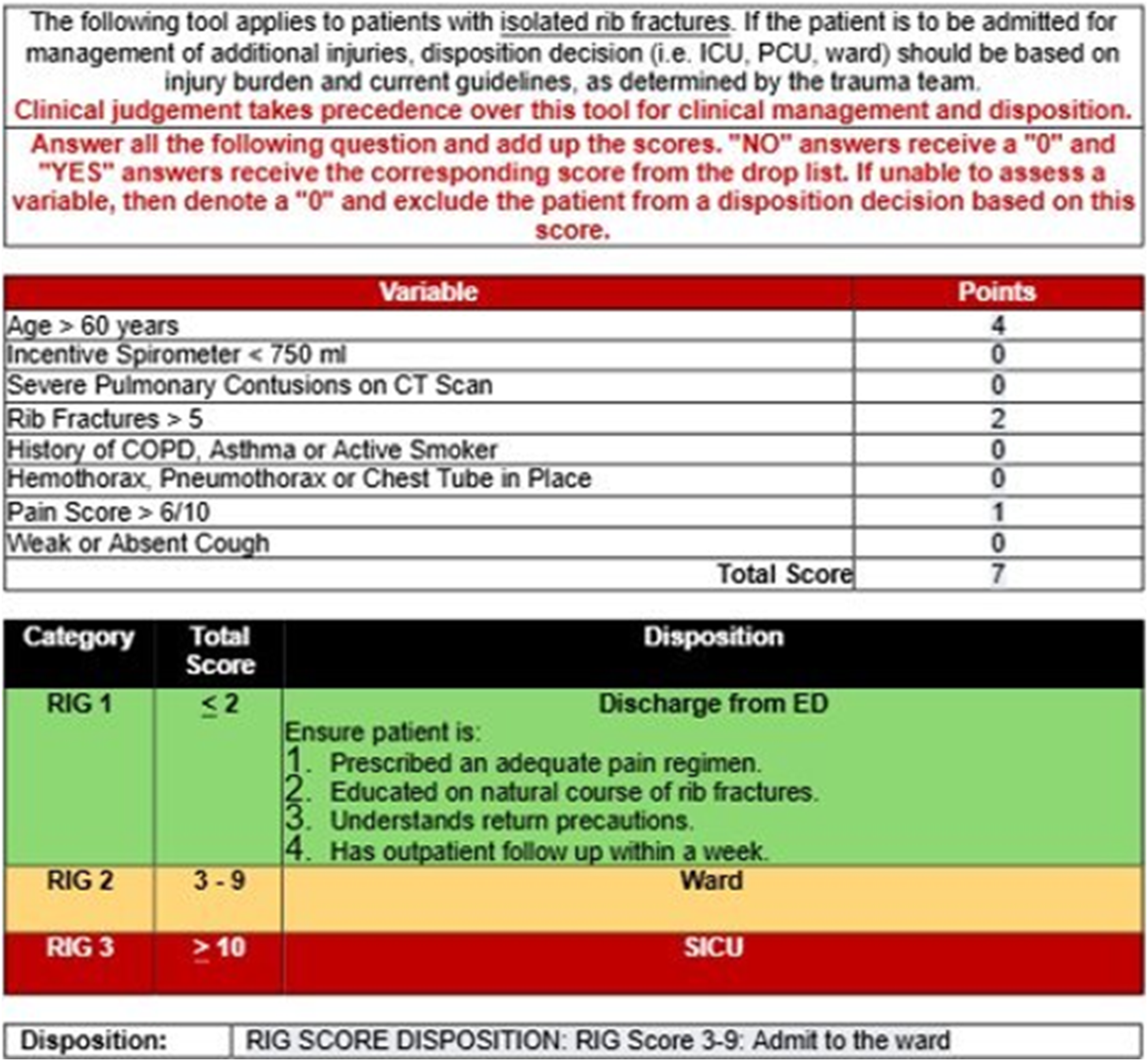
Although the RIG score has been validated, real-world, large-scale implementation and post-implementation compliance remain poorly described. Moreover, adoption and utilization likely vary across trauma centers based on pre-existing workflows and local practice factors. Therefore, the purpose of this study was to quantify the impact of using the RIG score as a triage tool for patients with rib fractures, specifically focusing on patient safety and resource utilization. We hypothesized that the use of the RIG score would decrease the rate of ICU admission for elderly patients with rib fractures without compromising patient safety.
Methods
After obtaining institutional review board (IRB) approval, the trauma registry at our Level I trauma center was queried for trauma patients who presented between January 1, 2020 and July 5, 2025 and met the following inclusion criteria. 1. Age 65 or older 2. Blunt trauma 3. One or more rib fracture
Tracked variables included demographics, diagnosis codes, Injury Severity Score (ISS), abbreviated injury scale (AIS) scores for all body regions, emergency department (ED) disposition, ICU admission, ICU length of stay (LOS), hospital LOS, mortality, and 30-day readmission.
Patients were stratified into two groups based on the date the RIG score was implemented at our institution. The pre-RIG cohorts included patients who presented prior to October 31, 2024, and the post-RIG cohorts included patients who presented on or after that date. Patients with AIS scores greater or equal to 3 in body regions other than chest were excluded. The rationale for this was that the disposition of these patients would likely be driven by concomitant injuries, rather than rib fracture severity. For the post-RIG cohort, the electronic medical records were additionally reviewed to assess compliance with the RIG SP.
RIG Smartphrase
Implementation of the RIG was accompanied by the development of a mandatory SP to be utilized and aid clinicians with patient classification and disposition. The SP allows for a user-friendly calculation of the RIG score after assigning a number for each of the score’s elements using a drop-down menu. The score’s elements include patient factors such as age and medical history, radiographic findings, clinical evaluation of inspiratory capacity with an incentive spirometer and level of pain. The clinician then adds the scores from each element for a final RIG score (range 0-18). Of note, all patients 60 years or older receive a minimum score of 4 which translates into a recommended admission to the ward, even in the presence of a single rib fracture. While there are three ranges of RIG score associated with a proposed disposition (RIG ≤2: discharge patient; RIG 3-9: admission to ward; RIG ≥10: admission to ICU), we emphasized that clinical judgment takes precedence over the RIG score alone. The SP allowed the clinician to select from a drop-down menu the disposition plan, including whether they were selecting a different disposition based on clinical judgment (Figure 1).
Rib Fractures Management Pathway
At our institution, the rib fracture management pathway consists primarily of a multimodal pain regimen and aggressive pulmonary toilet. We prioritize multimodal non-opioid pain medications with judicious use of opioids as breakthrough pain medications. We also utilize regular consultation with the inpatient pain service for evaluation and placement of epidural and paravertebral catheters for additional pain control in all patients with multiple rib fractures or uncontrolled pain with routine pain management orders. The primary change with implementation of the RIG score was the disposition guidance operationalized through the RIG SP.
The primary outcomes were ICU admission rate and unanticipated upgrade to the ICU, which was defined as ICU upgrade for a patient initially admitted to the ward. The secondary outcomes were overall mortality, ICU and hospital LOS, and compliance with the RIG SP. A subgroup analysis was performed for patients with multiple rib fractures, defined as two or greater rib fractures.
Statistical analysis was performed using IBM SPSS for Windows, version 29.0.2.0 (IBM Corp., Armonk, NY). Continuous variables were presented as median with interquartile ranges (IQR), and categorical variables were proportions and percentages. The two cohorts were compared using standard statistical tools. Proportions were compared using chi-square tests or Fisher’s exact tests where appropriate. Binary logistic regression was used to analyze association between binary variables and binary outcomes. Odds ratios and 95% confidence intervals are reported. Statistical significance was set at P < 0.05.
Results
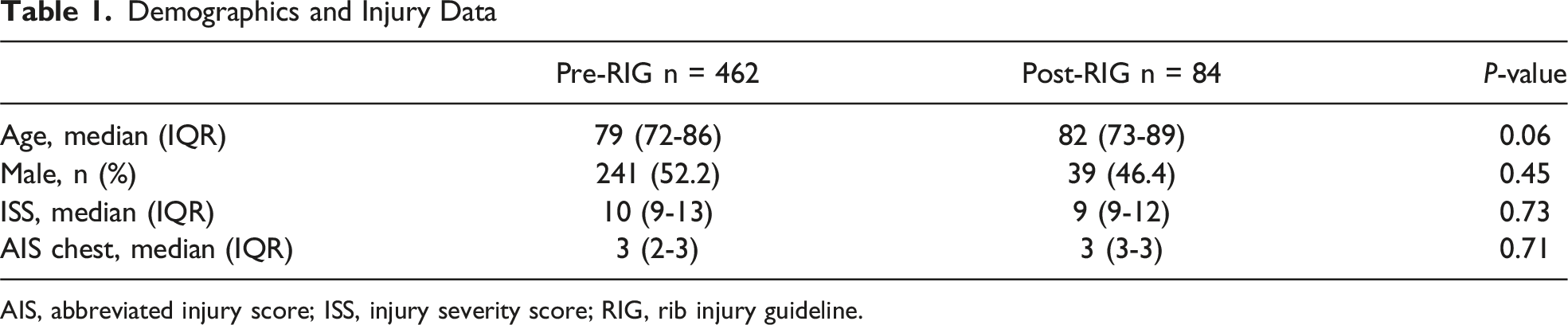
Over the 5 ½ -year study period, a total of 1673 patients presented with rib fractures and of those 546 (32.6%) met inclusion criteria (Figure 2). The median age was 80 years (IQR 73-87 years), and the majority were male (51.3%). The median ISS was 10 (IQR 9-13). 462 (84.6%) patients were in the pre-, and 84 (15.4%) were in the post-RIG group. Age (P = 0.06), gender (P = 0.45), ISS (P = 0.73), and AIS Chest (P = 0.71) were similar between the two groups (Table 1). Study flow chart. Demographics and Injury Data AIS, abbreviated injury score; ISS, injury severity score; RIG, rib injury guideline.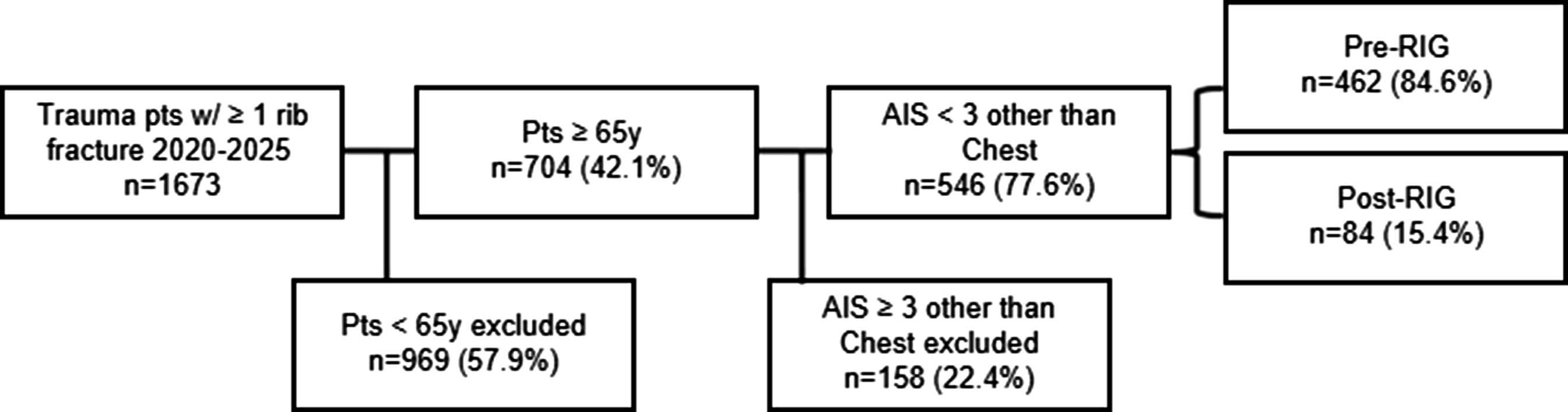
Primary Outcomes
Primary and Secondary Outcomes
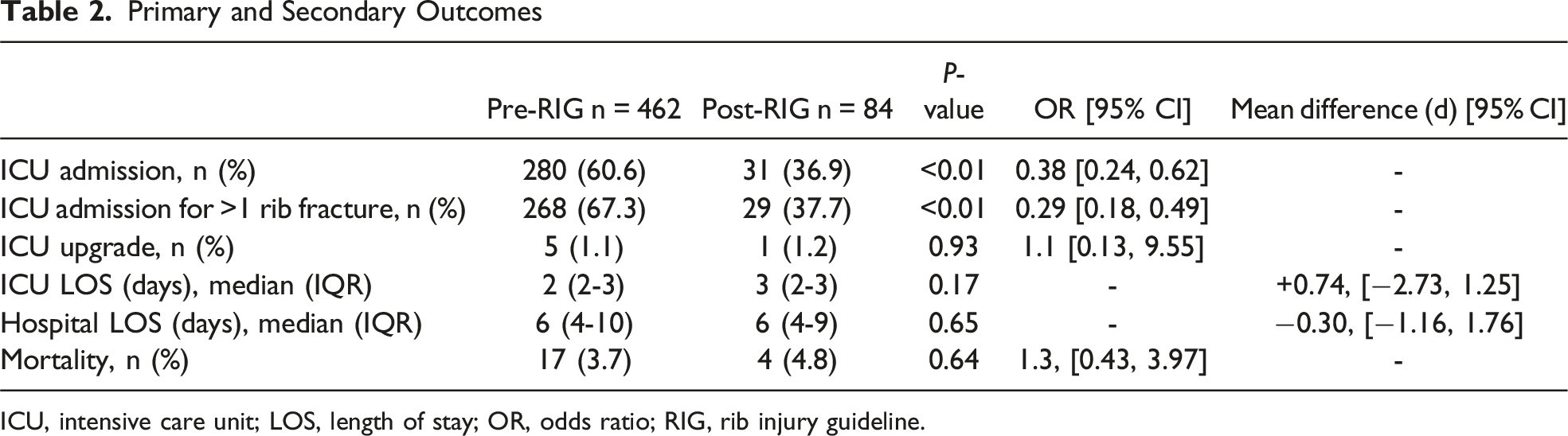
ICU, intensive care unit; LOS, length of stay; OR, odds ratio; RIG, rib injury guideline.
Secondary Outcomes
There was no difference in overall mortality between the pre-RIG and post-RIG groups (3.7% vs 4.8%, OR 1.3, 95% CI [0.43, 3.97], P = 0.64). Similarly, there was no difference in median ICU LOS (2 vs 3, P = 0.17) or median hospital LOS (6 vs 6, P = 0.65) between the pre-RIG and post-RIG groups (Table 2). In the post-RIG group, the RIG SP was used 82.1% (69/84) of the time, and the rate of compliance in each month was similar (P = 0.91) throughout the post-RIG period, including during the initial month of implementation (Figure 3). Review of the EMR revealed that in the 15 instances of non-compliance with the RIG SP, the most common reason for its omission was that the patient’s disposition was not based primarily on their rib fractures, but rather on a more severe injury (eg, traumatic brain injury or unstable spinal fracture). In the other instances, it is unknown why the SP was not used. Five of these 15 patients were admitted to the ICU during their hospital stay, and there were no unanticipated ICU upgrades or mortalities in this small sub-section. RIG SP compliance by month.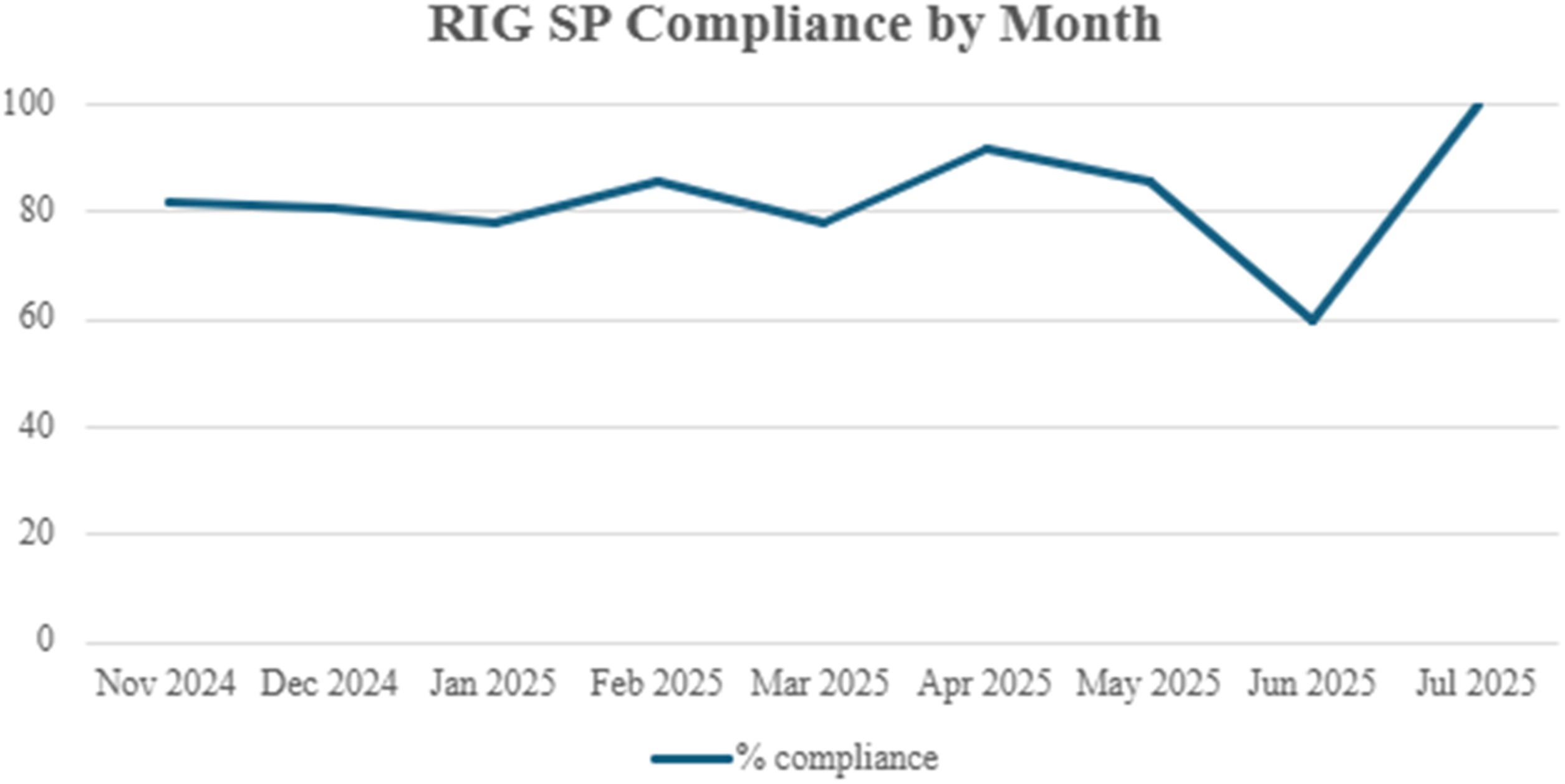
Discussion
In this study that analyzed the impact of implementing the RIG score as a triage tool for trauma patients at an urban Level I trauma center, we found that patients seen during the post-RIG group experienced over 60% lower odds of being admitted to an ICU without any impact on patient safety. Neither mortality nor unanticipated upgrade to the ICU were impacted by the implementation of the RIG score, confirming its safety. Furthermore, this reduction in ICU odds was even greater among patients with multiple rib fractures while preserving the same level of patient safety. Neither hospital nor ICU LOS was different in the post-RIG group, though ICU LOS did trend towards being longer. We theorized that this may have been in part due to fewer unnecessary ICU admissions, thus isolating patients who truly needed to be in the ICU for respiratory monitoring. The use of the RIG score with an integrated smartphrase within EMR allowed for broad adoption and good compliance and standardization of care at our trauma center.
The implementation of the RIG score at our institution did not modify any of the pre-existing framework set out by Nelson et al, 15 so it is unsurprising that we found similar results as they described. However, the extent to which we observed decreased ICU admission rates was unprecedented (Nelson et al, OR [95% CI] 0.46, [0.25-0.84]; Our study, OR [95% CI] 0.29, [0.18, 0.49]). 15 An explanation for this degree of reduction in ICU odds is that, as we theorized, had been over-triaging patients to the ICU. That we were able to cut our ICU admissions so drastically while preserving patient safety was a significant improvement for our institution. Our analysis contributes more evidence to support the use of comprehensive rib fracture triage systems, which combine clinical, anatomic, and physiological factors to determine appropriate management. Though we are unable to isolate the effect of the smartphrase alone on our clinical outcomes, the value of integrated EMR smart tools and their ability to improve efficiency at large volume institutions is noteworthy. Designing a SP to be used alongside clinical guidelines was not novel to our institution, as we had recent positive experience with creating a SP to be used with the modified Brain Injury Guidelines (mBIG) score. 17 The experience we had working with the mBIG SP likely contributed to the high level of compliance we saw in the initial months and the sustained compliance in the post-RIG period. Though we observed acceptable rates of compliance with the SP, we are continuing to evaluate other strategies to increase SP compliance in our clinical documentation.
When comparing the performance of the RIG score to previous triage tools or clinical practice guidelines, it is important to assess the variety of elements that are incorporated into the calculation of the RIG score. Previous guidelines and triage tools for rib fractures focused primarily on patient age and the extent of injury to the ribs and lungs, with less focus on physiologic factors.9,10,13,18 The addition of physiologic data such as incentive spirometry (IS) and vital capacity (VC) added another element to the triage and management of rib fractures, providing evidence that patients with lower IS and VC are at higher risk of pulmonary complications.15,16,19
Our study was limited by its retrospective nature and its pre- and post-design. The post-RIG period was only 8 months, which resulted in a sample size discrepancy between the pre- and post-RIG cohorts, limiting power to detect small differences in rare safety outcomes, including mortality and unanticipated upgrade to the ICU. Other potentially important trends in pain management and rib fixation during the study period were not captured with our study design, which was limited to the impact of the RIG score on ICU admission rates rather than pulmonary complications or surgical interventions. Despite these limitations, our study is able to clearly capture and quantify the benefits of the RIG score implementation in resource utilization without compromising patient safety.
In conclusion, implementation of the RIG score supported by an EMR-integrated SP was associated with a substantial reduction in ICU admissions among older trauma patients with rib fractures at our Level I trauma center, without an observed increase in morbidity, mortality or unanticipated ICU upgrades. As the RIG score safety has been previously validated, the findings from this study attribute substantial health care resource utilization too. Embedding the tool within routine documentation facilitated broad adoption and standardization of disposition decisions. Future research should evaluate the durability of these results across longer post-implementation periods and diverse settings.
Footnotes
Acknowledgments
We would like to acknowledge all those who contributed to this project, from its inception to the composition and editing of the manuscript. We would also like to especially thank the staff within our Trauma department and Trauma registry for their tireless work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.