
Abstract
Background
Traumatic brain injury (TBI) due to single-level falls (SLF) are frequent and often require interhospital transfer. This retrospective cohort study aimed to assess the safety of a criteria for non-transfer among a subset of TBI patients who could be observed at their local hospital, vs mandatory transfer to a level 1 trauma center (L1TC).
Methods
We conducted a 7-year review of patients with TBI due to SLF at a rural L1TC. Patients were classified as transfer/non-transfer according to the Brain Injuries in Greater East Texas (BIGTEX) criteria. The primary outcome measure was the occurrence of a critical event defined as deteriorating repeat head computed tomography (CT) scan or neurological status, neurosurgical intervention, or death.
Results
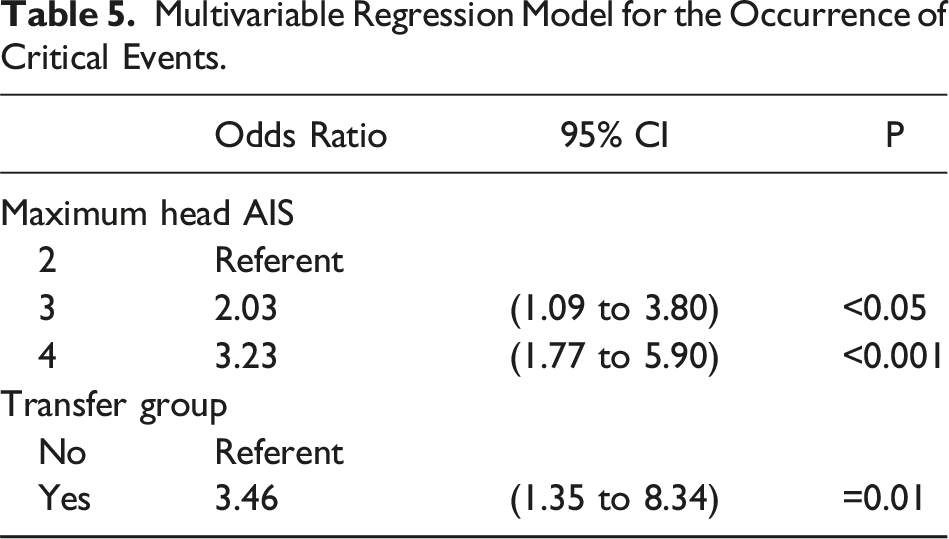
Of the 689 included patients, 63 (9.1%) were classified as non-transfer. Although there were 4 cases with a neurological change and one with a head CT change among the non-transfer group, there were no neurosurgical procedures or deaths. The Cox Proportional Hazard model showed a near 3-fold increased risk of experiencing a critical event if classified as a non-transfer. The multivariable regression model showed patients with an Abbreviated Injury Scale (AIS) of 3 was twice as likely to experience a critical event, with an AIS of 4, three times, and 3 times more likely to be classified to transfer.
Discussion
The BIGTEX criteria identify a subset of patients who can safely be observed at their local hospital. To confirm the safety and efficacy of this transfer criteria recommendation, a prospective study is warranted.
• Identifying distinct clinical traits facilitate safe surveillance of mild TBI patients at their local hospital. • The BIGTEX criteria identified mild TBI patients who can forego transfer to their level 1 trauma center. • A prospective pilot study is called for to validate the safety and efficacy of the proposed TBI transfer criteria.Key Takeaways
Introduction
According to the Centers for Disease Control and Prevention (CDC), traumatic brain injury (TBI) in the United States resulted in approximately 2.8 million related emergency department (ED) visits, hospitalizations, and deaths in 2013. 1 Age-adjusted rates of TBI related emergency care were 47.3% higher in 2013 when compared to 2007, with patients 75 years of age and older accounting for 17.9% of this increase, primarily due to falls. 1 The CDC also estimated that among the 2.5 million emergency room visits for TBI in 2010, 87% were treated in the ED and released, 11% were hospitalized then released, and 2% died. 2
Reports of improved mortality and functional outcomes among patients treated in tertiary centers 3 have led to the widespread practice of transferring most injured patients to a level 1 trauma center (L1TC). This has resulted in a climate where patients with minimal injuries travel long distances, incur increased medical expenses, but require no higher level of care available at their local hospital. More recently, the cost of treating all injured patients in a tertiary referral center has come into question. 4 A feasibility cost reduction pilot program utilized teleconsultations with neurosurgeons to mitigate transfers following mild head trauma. 5 Additionally, investigators into mild TBI and transfer reduction utilizing the TQIP database advocated for infrastructure development of local hospitals to optimize ED surgical care. 6
These findings underscore the relevance of transfer reduction following mild head trauma and emphasize the value of enhancing services provided in outlying lower level hospitals. Criteria to define minor to major head trauma and strategies to decrease transfer and resource usage are abundant in the literature.7,8 However, such paradigm shifts require ongoing study to inform clinical practice.
We sought to identify a subset of TBI patients, following a single level fall (SLF), to determine if they could safely remain at their local hospital using a brain injury transfer criteria created for this study. We hypothesized radiographic and clinical characteristics can identify patients who have a low probability of injury progression, neurosurgical intervention, or death, consequently, eligible to remain at their local hospital for observation and release.
Methods
This retrospective cohort study of patients admitted to a single rural L1TC for a SLF TBI from July 2014 through December 2021 received Institutional Review Board approval from the University of Texas at Tyler. Patients 18 years or older, who sustained a SLF TBI with an intracranial hemorrhage on head computed tomography (CT) were included. Injury was identified through 2015 Abbreviated Injury Scale (AIS) codes for skull fracture, subdural hematoma (SDH), subarachnoid hematoma (SAH), intraparenchymal hematoma (IPH), and epidural hematoma (EDH). Patients were excluded from the study if they had a head AIS ≥5 or intraventricular hemorrhage (IVH). Patients with such injuries require care at an L1TC due to complexity of injury and potential for deterioration, 9 making it appropriate to exclude these patients from this study, which focused on identifying those who can safely remain at their local hospital. Further, patients were excluded if no anatomic injury was found on head CT scan or had another anatomic body region AIS severity >3.
The BIGTEX Criteria.
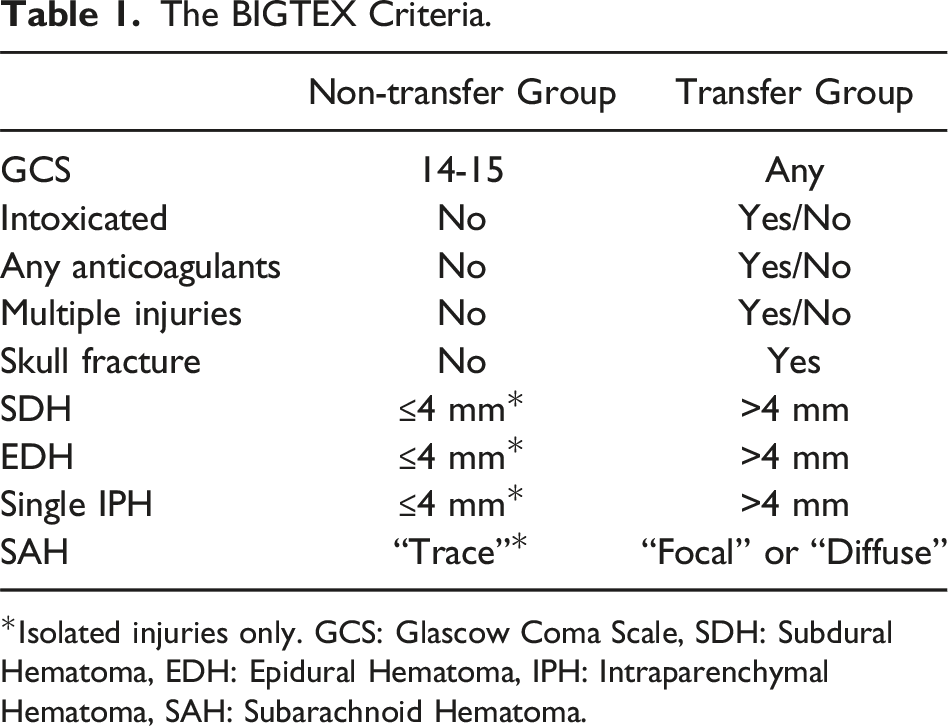
*Isolated injuries only. GCS: Glascow Coma Scale, SDH: Subdural Hematoma, EDH: Epidural Hematoma, IPH: Intraparenchymal Hematoma, SAH: Subarachnoid Hematoma.
The primary outcome measure was the occurrence of a critical event, defined as a worsening head CT scan, decline in neurological status, neurosurgical intervention, or death. Data collected from patient records included age, sex, race/ethnicity, vital signs on presentation, loss of consciousness, presenting Glascow Coma Scale (GCS), best in-hospital GCS, head AIS score, Injury Severity Score (ISS), alcohol intoxication (blood ethanol level of 0.08 g/dl or greater), use of antiplatelet or anticoagulant medications, details of CT scans, neurological findings on presentation, neurological changes during hospitalization, consultations, or interventions, intensive care unit (ICU) length of stay (LOS), hospital LOS, hospital complications, 30-day readmission, and in-hospital mortality. When the size of hemorrhage was unclear from the CT report, the CT scan was reviewed by attending clinicians.
Characteristics of the patients were calculated as frequencies and percentages or medians and interquartile ranges (IQR). Examination of associations or differences among the groups was tested using a chi-square or Fisher’s exact for categorical variables and the Mann-Whitney U test for continuous variables where appropriate. We tabulated the timing of a critical event during the initial 7 days of admission based on the IQR of our patient populations hospital LOS, which fell between 2 and 6 days. The Kaplan-Meier plot with a log-rank test and the Cox Proportional-Hazard Model were used to test time to any of the defined events. Hosmer, Lemeshow, and Sturdivant’s process of purposeful selection was applied to select independent variables for inclusion in the multivariable regression model. 14 Significance was defined as P < 0.05. Statistical calculations were performed using STATA v.16.1 (Stata, Inc., College Station, TX).
Results
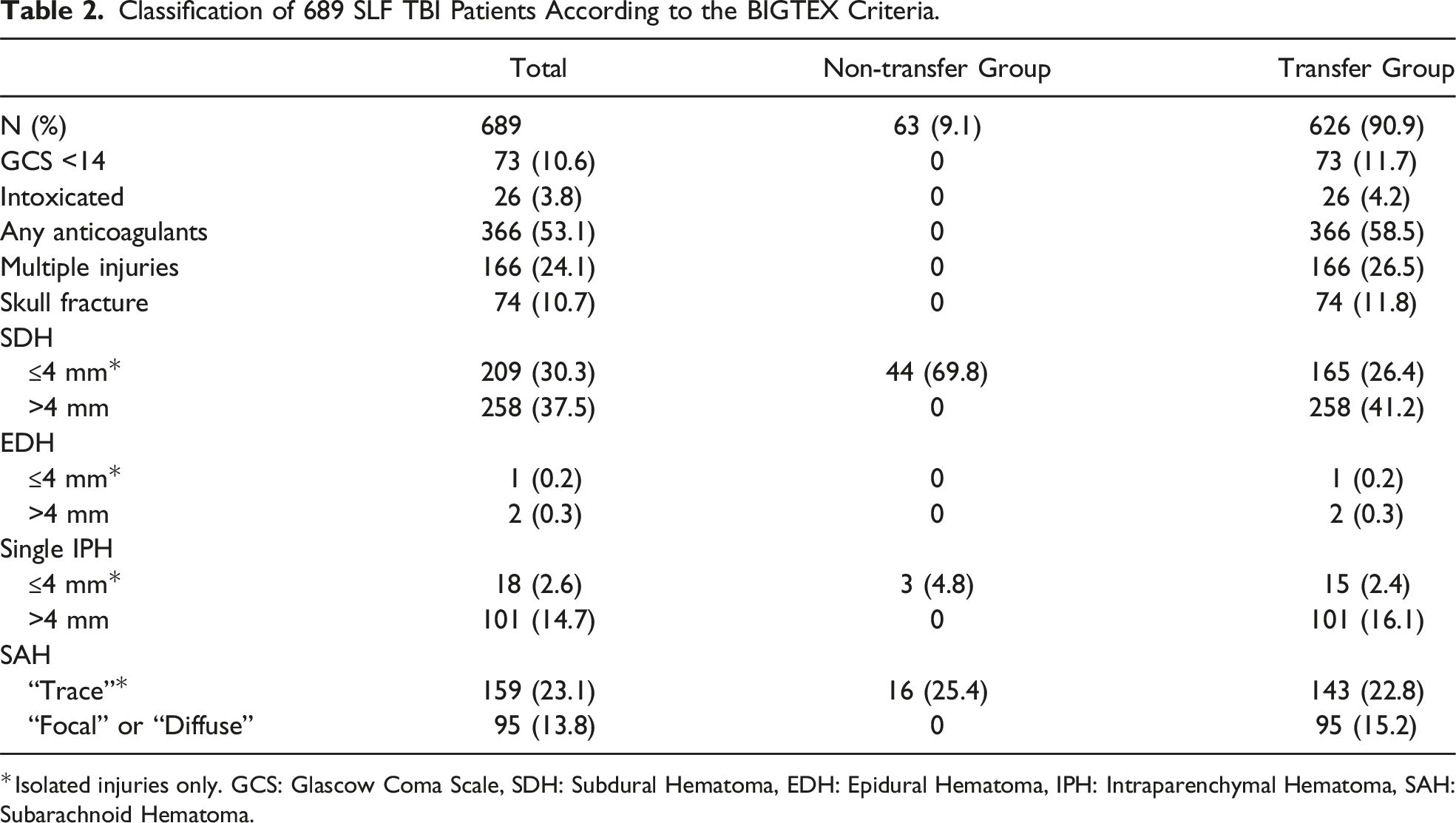
Of the 1,133 patients identified with a TBI, 689 met inclusion criteria (Figure 1). Most patients met 1 or more criteria for transfer (90.9%; n = 626). Among the transfer group, 73 (11.7%) had a GCS <14, 26 (4.2%) were intoxicated, 366 (58.5%) were on some type of anticoagulant or antiplatelet medication, 166 (26.5%) had multiple injuries, and 74 (11.8%) had a skull fracture. The most common TBI among both patient groups was SDH(67.8%), followed by SAH(36.9%). The non-transfer group included 63 patients (9.1%). Table 2 details the classification patients according to the BIGTEX criteria. BIGTEX flow diagram. Classification of 689 SLF TBI Patients According to the BIGTEX Criteria. *Isolated injuries only. GCS: Glascow Coma Scale, SDH: Subdural Hematoma, EDH: Epidural Hematoma, IPH: Intraparenchymal Hematoma, SAH: Subarachnoid Hematoma.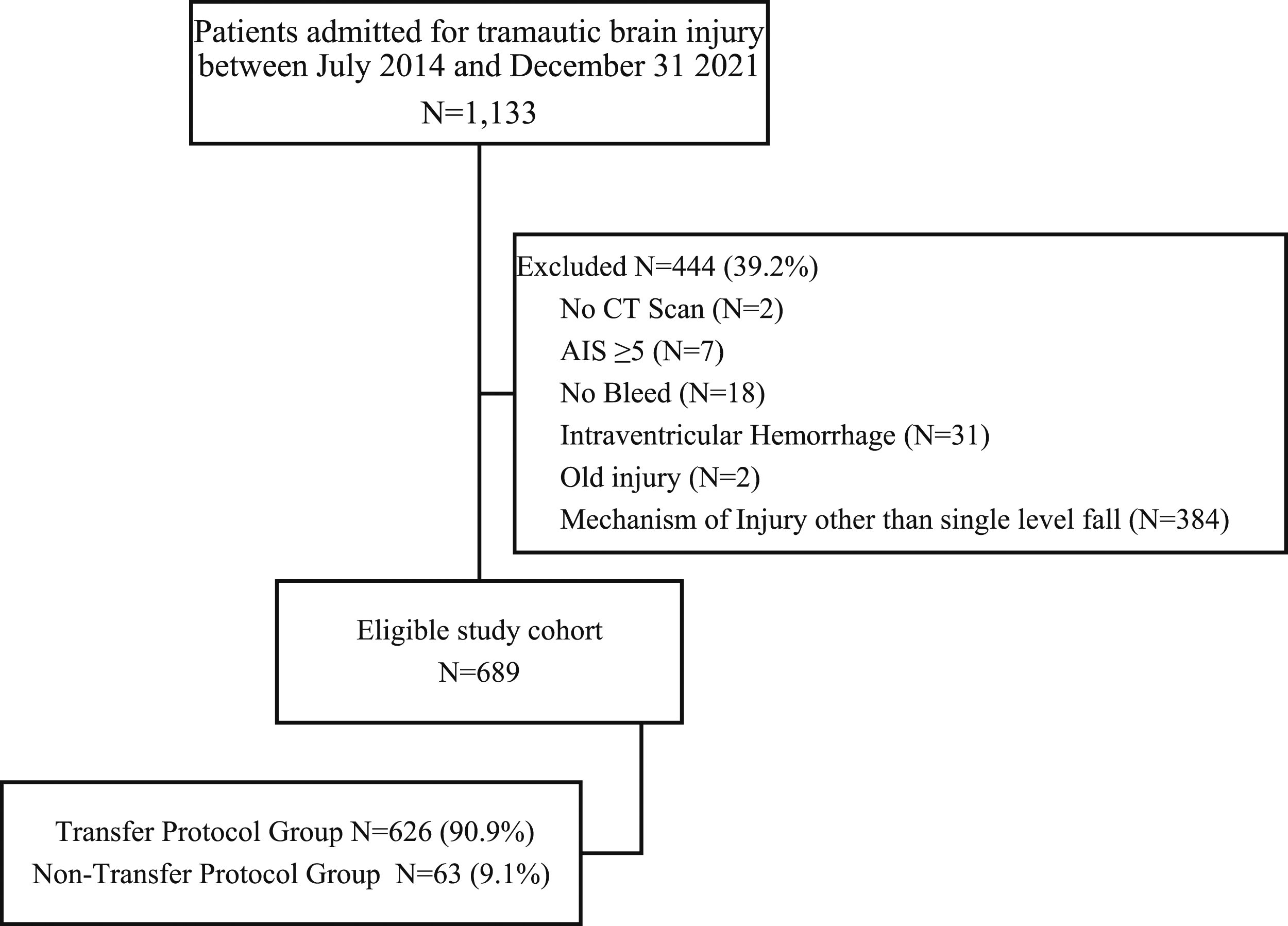
Patient Characteristics of 689 Single Level Falls by Transfer Recommendation.
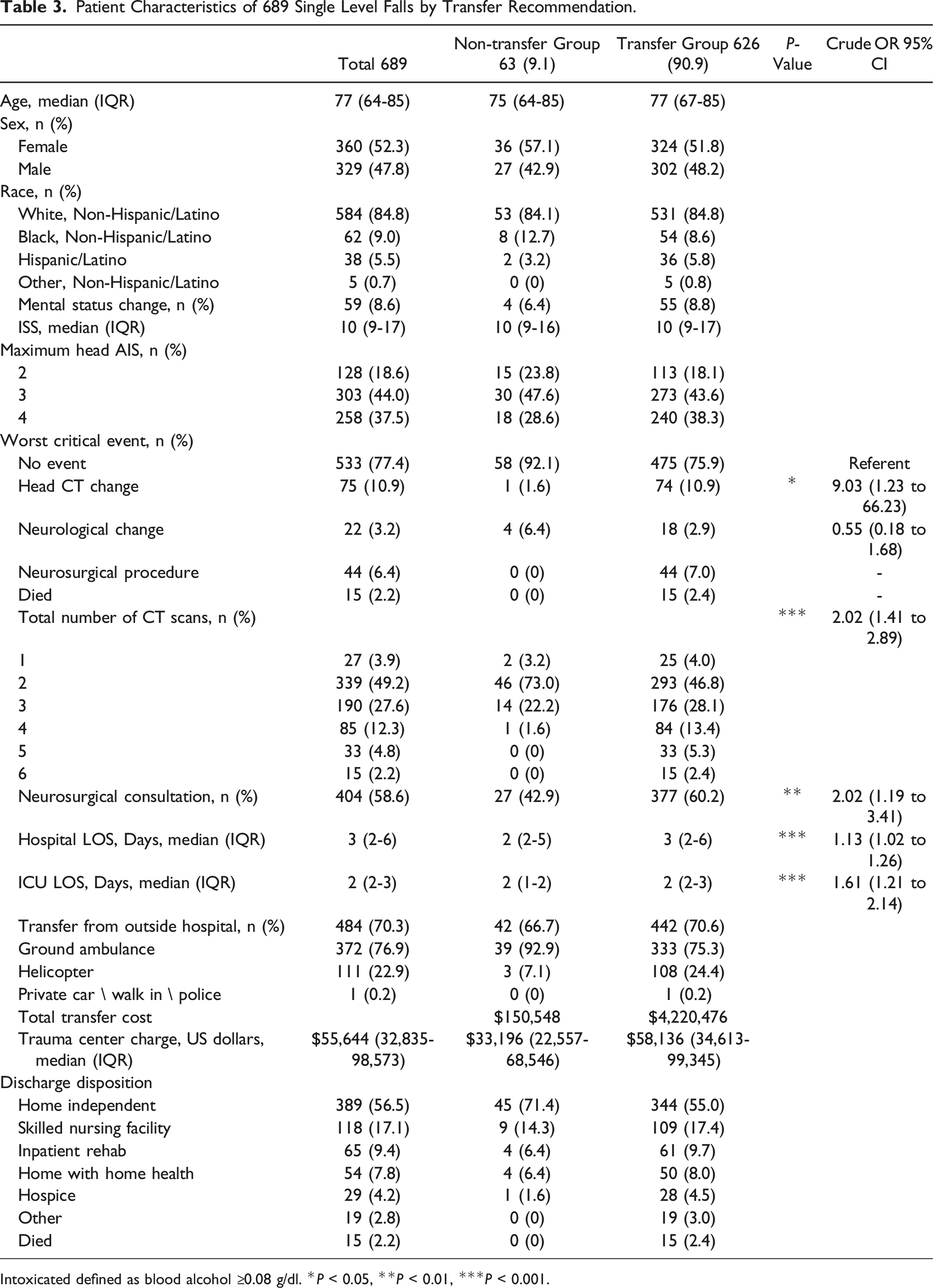
Intoxicated defined as blood alcohol ≥0.08 g/dl. *P < 0.05, **P < 0.01, ***P < 0.001.
Comparing transfers to non-transfers, length of stay (LOS) showed a linear effect, where with each 1-day increase in hospital or ICU LOS there was an increased chance of meeting transfer criteria of 13% (OR: 1.13; 95% CI: 1.02 to 1.26) or 61% (OR: 1.61; 95% CI: 1.21 to 2.14). Roughly half of the transfer group were discharged home (55%) compared to 71.4% of the non-transfer group, followed by 17.4% of the transfer group vs 14.3% of the non-transfer group discharged to a skilled nursing facility (SNF). There were no neurosurgical interventions or deaths among the non-transfer group. See Table 3.
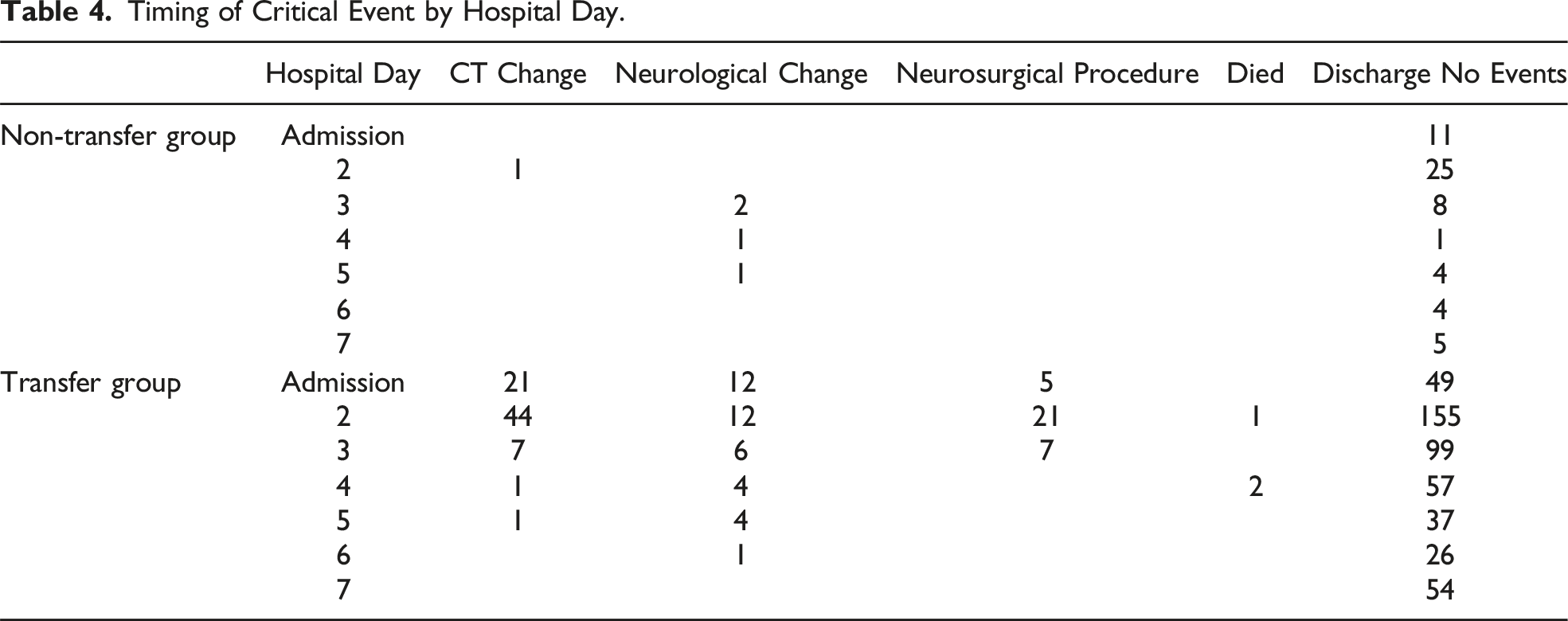
Timing of Critical Event by Hospital Day.
Multivariable Regression Model for the Occurrence of Critical Events.
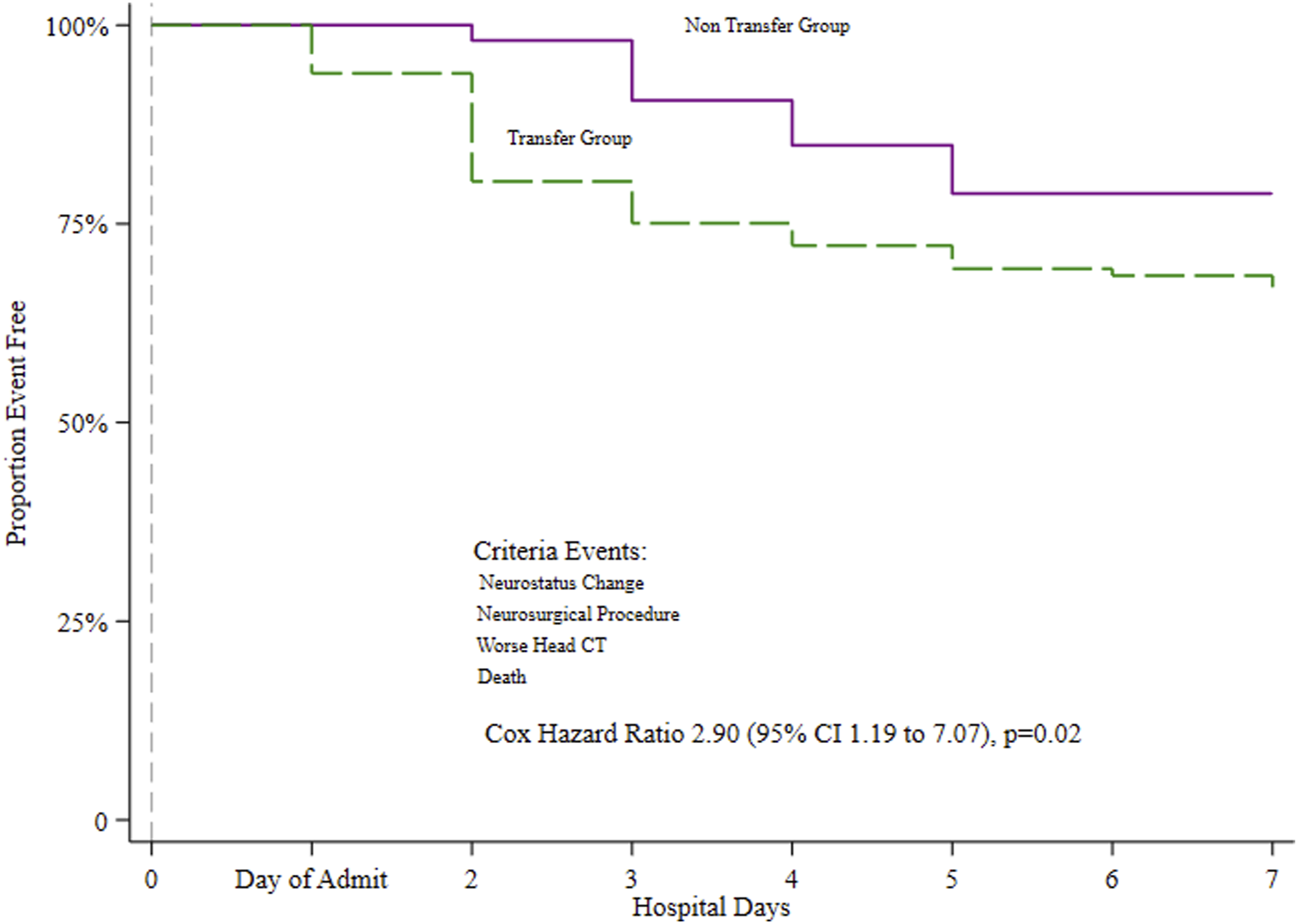
Hospital days until critical event.
Discussion
The current practice for TBI patients in our rural trauma system has been to transfer all patients with any findings on a head CT scan at their local hospital to obtain a repeat head CT and neurosurgical consultation at our L1TC, regardless of clinical status. These practices have been called into question. 15 This study explored a rural interhospital TBI non-transfer guideline, the BIGTEX criteria, with the aim of identifying distinct clinical traits that would facilitate the safe surveillance of patients at their local hospital. Upon examination of these data, it appears that the non-transfer patient group classified using the predefined radiographic and clinical characteristics identifies patients who can be safely managed by their local hospital.
Which combination of clinical variables provides accurate diagnosis of mild TBI has been debated. Beginning in 1974, GCS has been used to classify mild, moderate, and severe TBIs, even though the scale was not designed with the intention of diagnosing mTBI. 16 Concern pertaining to patients classified as mild with a score of 13-15 has been voiced, resulting in calls to shift a GCS of 13 and/or 14 to the moderate category and continue work towards identification of clinical variables to combine with the GCS to more effectively identify mTBI. 15 Conflicting results identifying the right mix of clinical features has caused continual shifts in the foundations of mild TBI management. Implementation of proposed guidelines has been controversial.16,17 Several investigators have argued in favor of universal brain injury guidelines7,8, 9; however, to date, no consensus yet exists. Using the Glasgow Outcome Scale, combinations of GCS, ISS, and AIS has been reported to improve classification of TBI. 18 Yet, reliability has yet to be established.11,19 While there was no difference in univariate analysis between transfer groups and maximum head AIS, the multivariable regression model showed as the patients head AIS increases the probability of experiencing a critical event increased.
Current dogma, among our health care system, involves monitoring all TBI patients through repeat head CT and neurosurgical consultation at their L1TC. Within our non-transfer patient group a majority had repeat head CT (73%), where 1 patient had a CT scan change in classification without increase in size of hemorrhage, and no patients required intervention or died. Clinicians at local lower level unit hospitals may utilize resources to screen and make informed decisions to guide decision making pertaining diagnostic tool usage, weighing the balance of efficacy of repeat head CT and increased medical care costs. Two repeat head CT criteria have been reported to reduce rates of unnecessary repeat scans: The New Orleans Criteria (headache, vomiting, drugs or alcohol, amnesia, visible trauma above clavicle, seizure) or the Canadian CT Head Rule-Mild TBI (GCS <15 2 hours after injury, skull fracture, vomiting, amnesia, dangerous MOI). 17 The neurosurgical consultation rate within our non-transfer group approached 50%, with no interventions. Reports on the utility of neurosurgical consultation among mild TBI patients varies, with calls for overall reduction in usage due to low rates of death or intervention, 10 and recommendation for increased usage through telemedicine in order to avoid unnecessary transfer. 5
In the United States, 40% of the population live in a trauma desert: defined as living in a county over an hour from a hospital equipped for major traumatic injuries. Research exploring rural emergency transport and outcomes revealed age and increasing ISS, not transport distance or time, contributed to the mortality of the patient. 20 Recommendations include building regional trauma systems, with local stabilization units, in order to stabilize patients and reduce negative outcomes. 6 Of concern, in a rural setting, is the need for emergent care. Accordingly, triage applied in this setting must provide for ongoing consultation with the affiliate L1TC. 21 Integrating and promoting usage of scoring tools like the BIGTEX criteria, Glasgow Outcome Scale, GCS, repeat head CT criteria, and neurosurgical consultation through telemedicine at lower level trauma care hospitals provide the triage tools that effectively classify patient level of care while reducing healthcare resource utilization, namely, transfer to a level 1 trauma center.
The next stage would be to conduct a pilot study utilizing these guidelines for non-transfer of mTBI patients. Training with all relevant personnel will be required to communicate the updated transfer guidelines. Continual communication and follow-up support throughout the pilot phase will be necessary while shifting away from the current practice of transferring all patients with even trace evidence of TBI to a L1TC. A concerted effort to connect neurosurgeons at the L1TC with hospitalists at the lower level unit is vital when support is needed to make timely decisions when the decision to retain a patient is unclear. Alan et al. demonstrated, in their pilot study utilizing teleconsultations with a neurosurgeon at a L1TC to reduce transfers of mTBI patients, was not only feasible but also reduced costs by more than half, with a mean cost reduction of $4482 to $2003 per patient. 5
The financial advantages of reducing transfers are particularly pronounced in rural locations compared to urban settings. A comprehensive literature search from 1991 to 2019, found a higher propensity for patient transfers to other facilities in rural areas as compared to urban areas (rural: 8.5% vs urban: 2.7%). 22 This emphasizes the economic sagacity of curtailing superfluous L1TC transfers in rural regions. In these contexts, the monetary strain of medical transfers disproportionately impacts rural residents. In the wake of such findings, guidelines to formulate cost mitigation strategies in health care systems have gained increasing prominence. 11 Reducing interhospital transfers can yield substantial cost reductions, primarily due to the associated reduction in both transfer expenses and overall medical outlay.7,10
Limitations
Data was collected from a single L1TC, which potentially limits the generalizability of the findings. The current patient group had no EDHs among the non-transfer group and only 3 patients with an IPH, as such the safety of these patients being retained for non-transfer should be interpreted with caution. Additional studies involving institutions in varying regions and larger sample sizes are recommended. Implementation of the BIGTEX criteria will require close surveillance to ensure the safety of the patient under the newly established clinical practice recommendations pertaining to management of TBI in the decision to transfer.
Conclusion
Through the implementation of a systematic non-transfer criteria based on clinical and radiological factors, health care providers can effectively identify a subset of patients with a single-level fall and TBI who may be safely managed at a rural trauma center without the need for transfer to a L1TC. This approach could streamline the management of patients with TBI in a rural setting, classifying those who are unlikely to need a higher level of care to be managed at their local hospital. To confirm the safety and efficacy of this transfer criteria recommendation, a prospective pilot study is warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.