
Abstract
Keywords
Introduction
Trauma has been consistently identified as one of the largest contributors to total health care costs in the United States and worldwide. 1 Despite its substantial impact, transparency regarding the cost of providing trauma care is lacking, with prior research revealing inconsistent billing and collection practices. 2 Trauma centers must invest heavily in facility infrastructure and human resources to maintain designation and ensure availability of emergency resources. This includes the availability of an operating room, interventional radiology suite, nurses, therapists, technicians, subspecialists, and backup call systems for trauma surgeons, neurosurgeons, and other staff. 3 Consequently, trauma centers impose an “activation fee” to help offset the substantial operating costs required to provide infrastructure and emergency resources available at any moment in time. 4 However, only about 30% of trauma charges are collected and concerns have arisen regarding the burden of this fee on vulnerable and financially disadvantaged trauma patients. 5 This is even more concerning as this system-wide readiness oftentimes benefits other patients, particularly those who require immediate access to specialized resources and emergency interventions in quaternary medical centers, such as hemorrhaging cancer patients or obstetric patients experiencing severe complications. In contrast, elective open inguinal hernia repair, a common procedure in the United States (estimated 800,000 cases annually), has remained relatively fixed in terms of cost. This can be attributed to the relatively unchanged surgical technique, minimal inter-hospital variation, and already low surgical costs. 6
Expenses associated with health care are the most common cause of bankruptcy in the United States. 7 Therefore, this study sought to examine trends in health care cost for trauma patients compared to unilateral elective open inguinal hernia repair patients, hypothesizing that inpatient trauma care cost would increase from 2010 to 2018, while inpatient elective open inguinal hernia repair cost would remain relatively stable during this period.
Materials and Methods
This study was deemed exempt by the institutional review board and a waiver of informed consent granted as it utilizes a deidentified national database. No funding was provided. The Nationwide Inpatient Sample (NIS) database was queried for admitted patients of any age undergoing unilateral elective open inguinal hernia repair or patients with trauma-related admission during the years 2010-2018. The NIS is an all-payer inpatient care database that contains data on over 7 million hospital stays yearly across the United States. The NIS database includes a sample of discharges from community hospitals, public hospitals, and academic hospitals, further stratifying the hospitals into rural, urban teaching, and urban non-teaching. It was developed for the Healthcare Cost and Utilization Project as a way for researchers and policymakers to estimate national utilization, cost, and outcomes associated with US health care. The database includes total charges for each hospital discharge. Of note, “charges” specify the amount that a hospital bills for services, which differs from “cost,” which are the actual expenses to produce the hospital services, including wages and supplies. The Healthcare Cost and Utilization Project (HCUP) does not include professional (physician) fees. To allow for cost estimates, the HCUP allows for conversion of the HCUP charges into cost estimates by utilizing a file with hospital-specific cost-to-charge ratios based on all-payer inpatient cost for every hospital in the database. In this study, we utilize the HCUP cost-to-charge ratio. We used data spanning from 2010 to 2018 which over this period represented 96% to over 97% of the national population. 8 International Classification of Diseases, Ninth Revision (ICD-9-CM) and Tenth Revision (ICD-10-CM) Clinical Modification codes were utilized to identify patients undergoing unilateral open inguinal hernia repair as well as trauma patients. A multiple linear regression model compared the total costs for unilateral, elective open inguinal hernia admissions to those for trauma admissions adjusted for individual- and hospital-level confounders.
Data on costs per admission, the number of elective open inguinal hernia repair and trauma admissions as well as total annual health care costs over time were analyzed. A multiple linear regression was used to estimate the association of individual variables such as year, age, severity of disease, and length of stay (LOS) as well as hospital-level variables including hospital location (urban vs rural) and teaching status with log total admission charges. Log transformation of the total charges compensated for a skewed distribution. Severity, as defined by the All Patient Refined Diagnosis-Related Groups (APR-DRG) system, categorizes illness-related loss of function as follows: 0 (no class specified), 1 (minor loss of function with no comorbidities or complications), 2 (moderate loss of function), 3 (major loss of function), and 4 (extreme loss of function). These levels reflect the clinical impact of the illness, including comorbidities and complications, on patient functionality and resource utilization. Year was initially included in the model in categorical form and showed a linear relationship with log total charges, so it was then included as a continuous covariate in the final model. Scatterplots were generated to investigate the trends in the number of admissions, cost per case, and total costs from 2010 to 2018. The missing data rate was 1.67%, and only complete records were used for the regression model. All analyses were performed using R and R Studio (2023.06.0 Build 421 “Mountain Hydrangea” Release).
Results
Trends of Total Health Care Costs for Trauma vs Elective Open Inguinal Hernia Repair
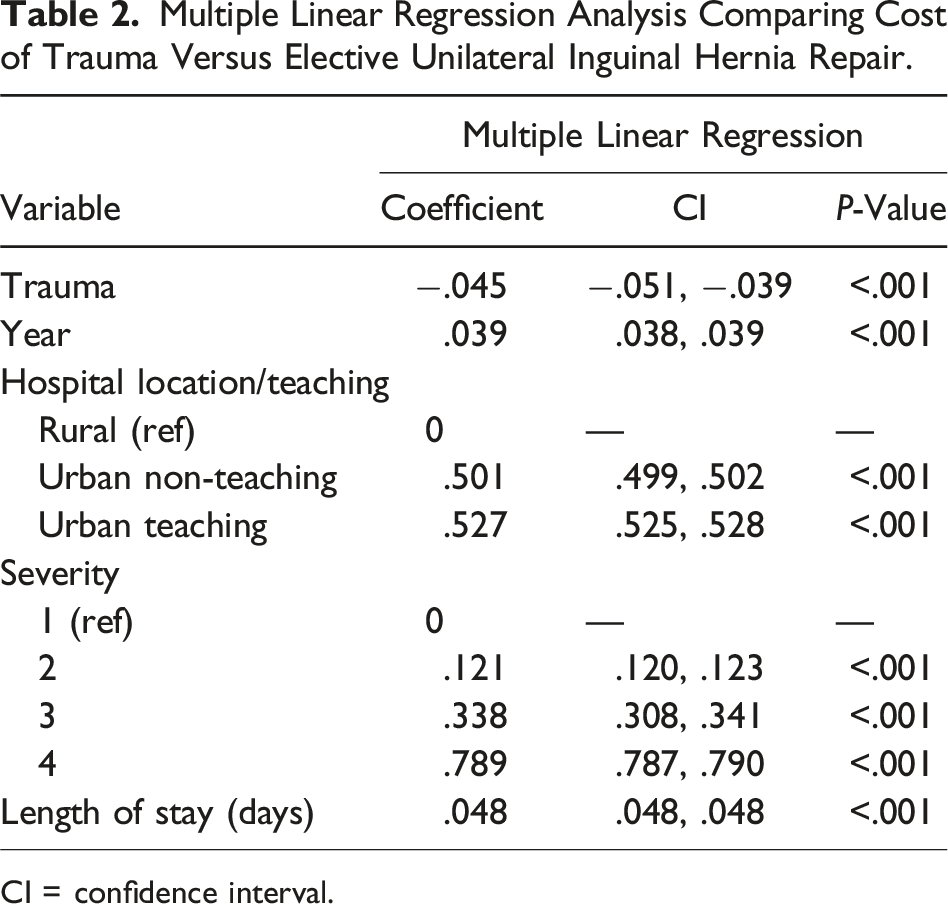
Total annual health care costs for admitted elective open inguinal hernia repairs increased from $57 million in 2010 to $72 million in 2018 (26% increase), whereas total annual trauma admission costs increased from $77 billion in 2010 to $102 billion in 2018 (32% increase) (P < .001) (Figure 1). The distribution of comorbidities in the study include hypertension being the most prevalent (55.0%), followed by tobacco use (29.2%), diabetes (26.3%), and obesity (13.7%) (Table 1). The multiple linear regression model showed that trauma admission costs were 4.5% lower than inguinal hernia admission costs, after adjusting for year, age, severity of disease, hospital location/teaching status, and LOS (Table 2). Trends in the total health care costs of patients admitted following elective unilateral inguinal hernia repair versus trauma (2010-2018). Distribution of Comorbidities in the Study Population. Multiple Linear Regression Analysis Comparing Cost of Trauma Versus Elective Unilateral Inguinal Hernia Repair. CI = confidence interval.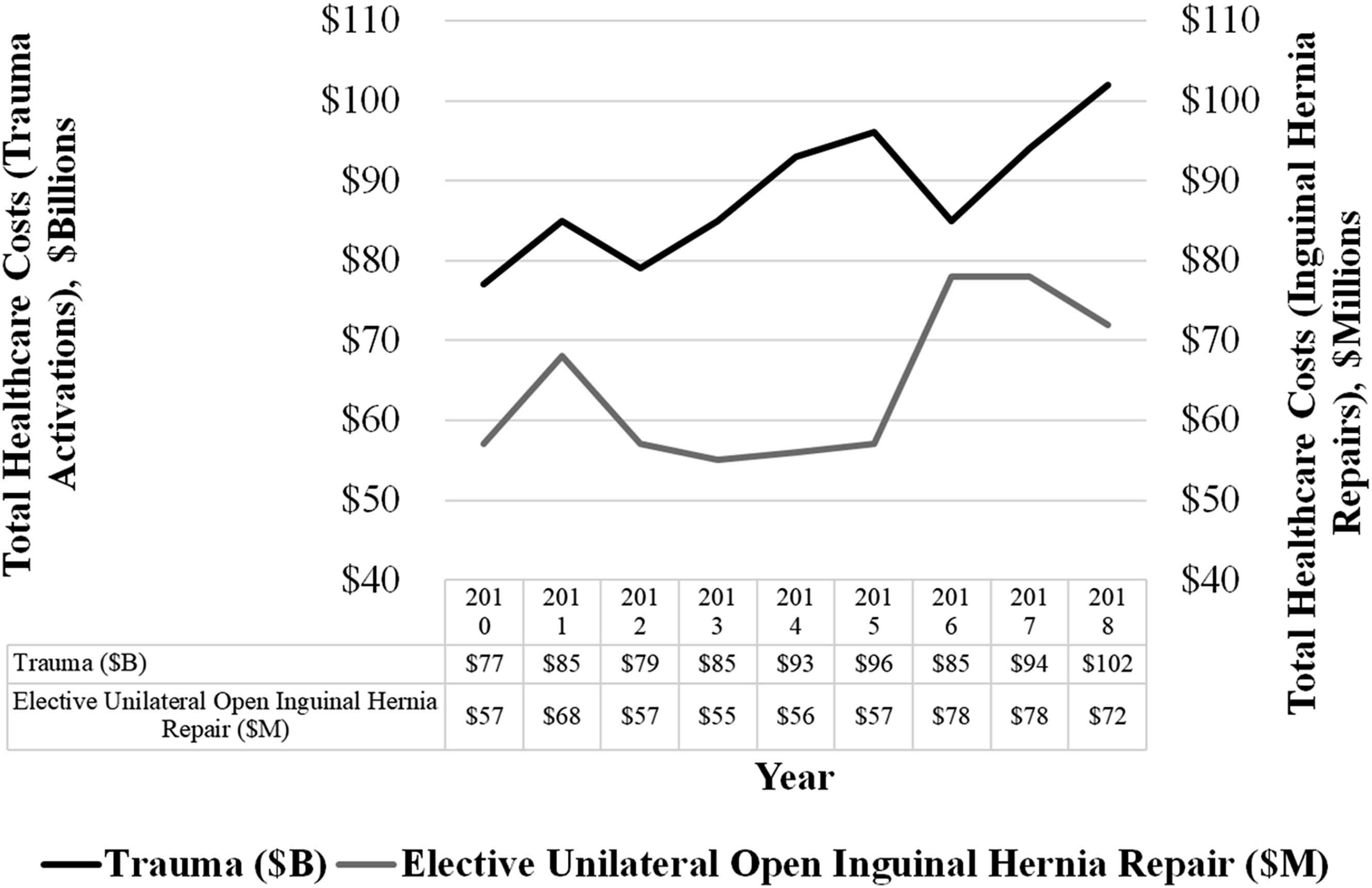

Trends of Health Care Cost per Patient for Trauma vs Elective Open Unilateral Inguinal Hernia Repair
The cost associated with unilateral elective open inguinal hernia repair admissions more than doubled over the study period, increasing from $36,053 in 2010 to $74,453 per case in 2018. Trauma admission costs rose by 34% ($61,484 to $82,347) over the same period (Figure 2). Trends in the health care costs per patient admitted following elective unilateral inguinal hernia repair versus trauma (2010-2018).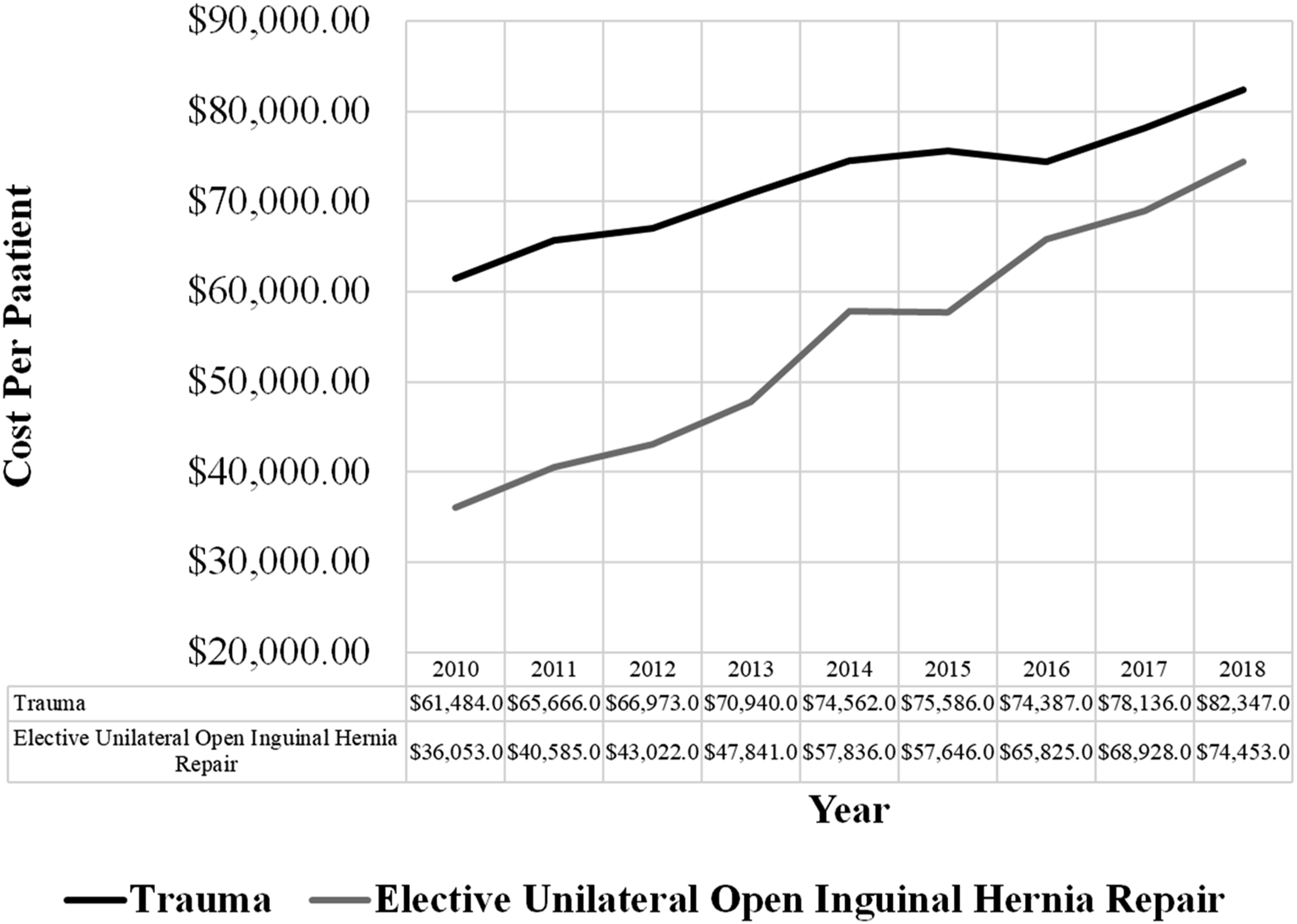
Trends of Number of Admissions for Trauma vs Elective Open Inguinal Hernia Repair
There was a slight decrease in trauma admissions (1,255,136 in 2010 to 1,236,225 in 2018) as well as a more substantial decrease in unilateral elective open inguinal hernia repair admissions (1574 in 2010 to 964 in 2018) (P < .001) (Figure 3). Trends in number of admissions for elective unilateral open inguinal hernia repair versus trauma (2010-2018).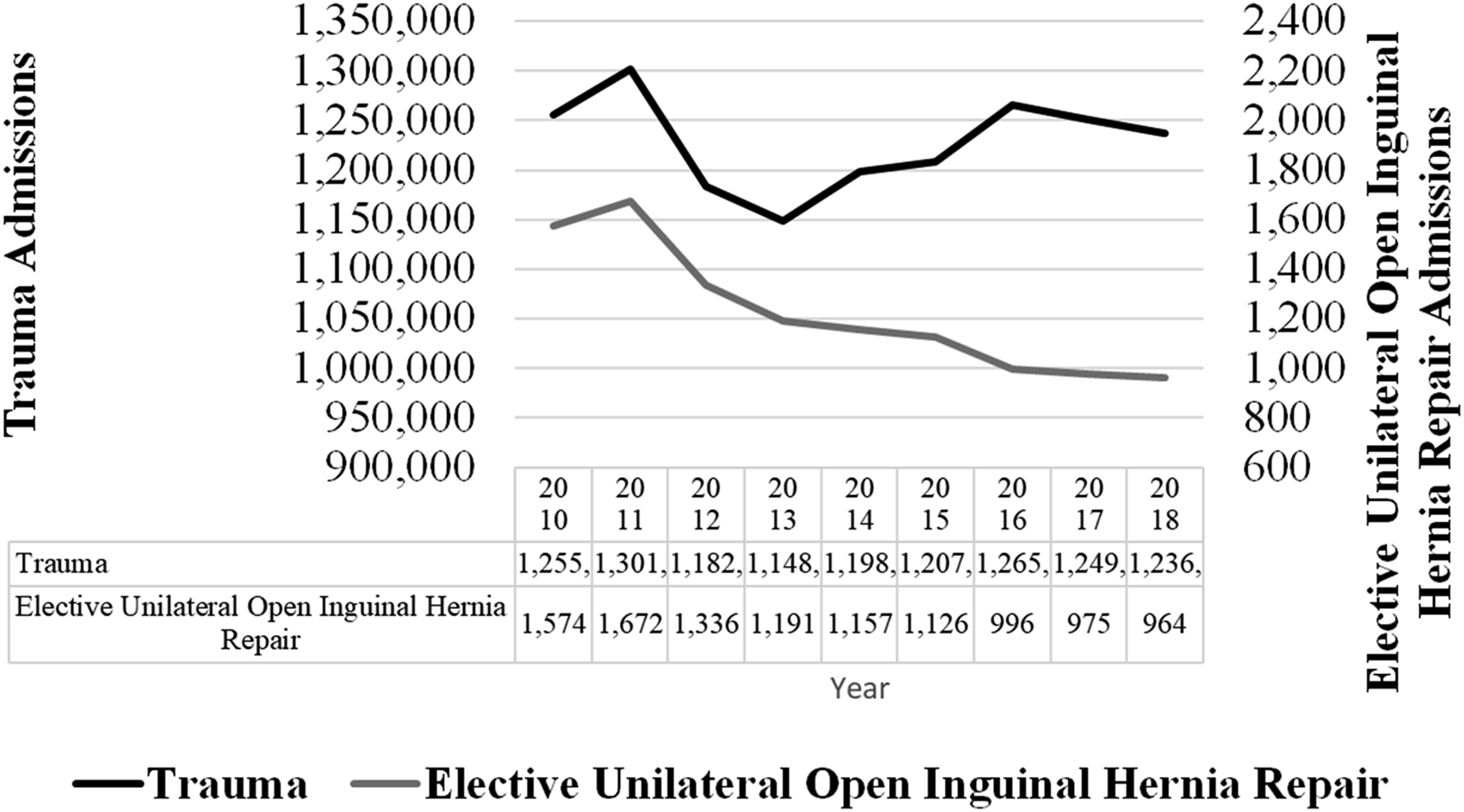
Trends of Length of Stay in Days for Trauma vs Elective Open Inguinal Hernia Repair
For inguinal hernia repair, the median length of stay was 3 days from 2010 to 2017 increasing to 4 days in 2018. For trauma patients, the median length of stay was unchanged at 4 days from 2010 to 2018 (Figure 4). Length of stay in days for trauma admissions.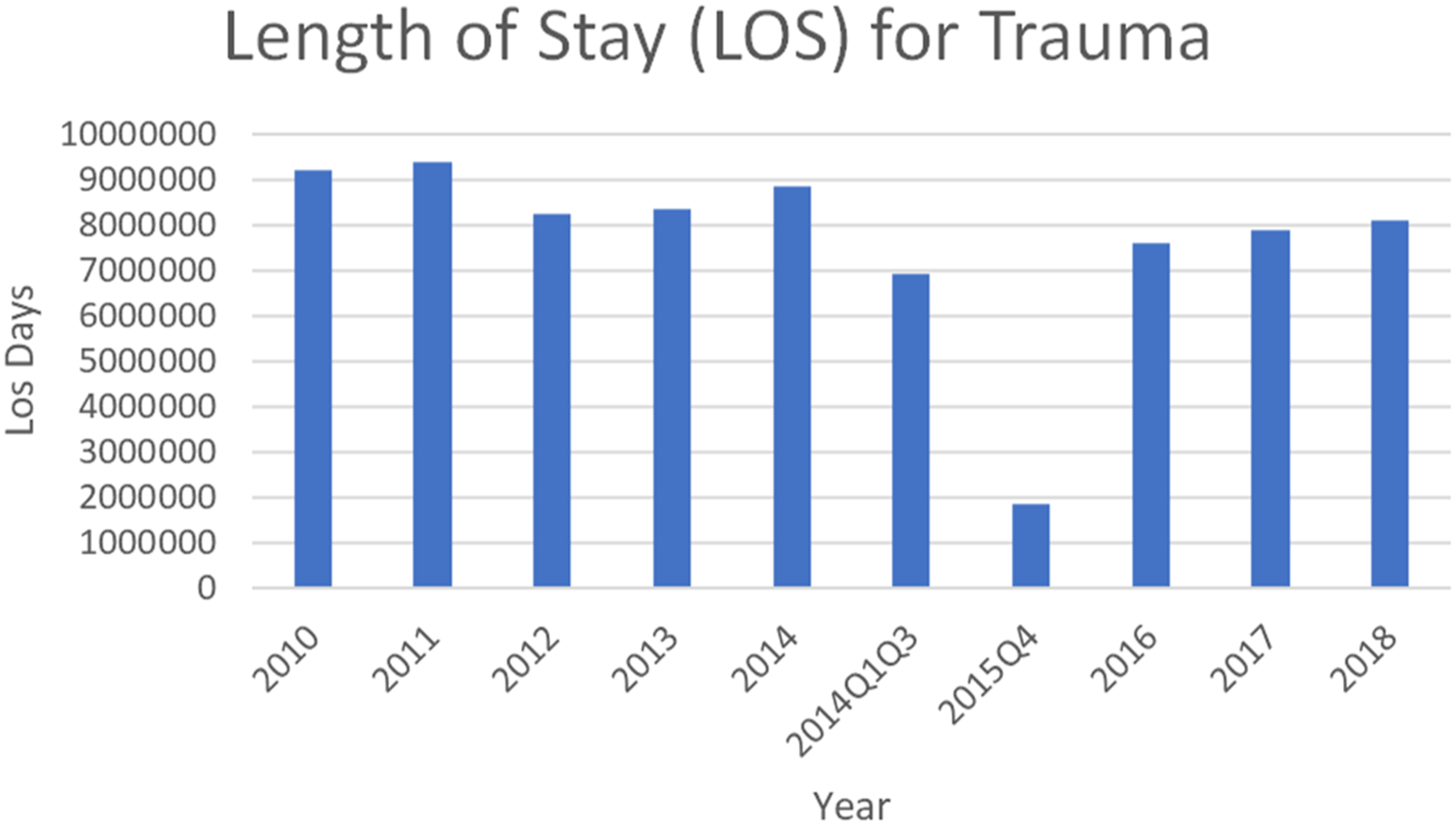
Discussion
Health care expenditures in the United States have risen significantly, in part due to the exacerbation of modifiable risk factors such as body mass index, blood pressure, and smoking, which accounted for over $730 billion in 2016. 9 Surgical patients represent another large segment of health care expenditure in the United States, accounting for over 150 billion dollars in spending by the Medicare program per year. 10 As such, this study sought to evaluate trends in admissions and costs of trauma care compared to a relatively standard surgical procedure such as elective, unilateral open inguinal hernia repair between the periods 2010-2018. In support of the hypothesis, our national analysis revealed a growing cost associated with trauma admissions. However, contrary to our hypothesis, the per-patient cost for elective open inguinal hernia repair increased even more than that of trauma patients. Despite this, the total cost of trauma admissions rose by $25 billion, partly due to increased cost of trauma admissions as well as an overall only slightly decreased number of trauma admissions. In contrast, the total economic burden of elective open inguinal hernia repairs only increased by $25 million, as while the cost of admissions substantially increased, there was also a significant decrease in overall admissions for unilateral open inguinal hernia repair.11-14
Trauma care at the beginning of this study in 2010 started from an already expensive level of over $60,000 per patient. Furthermore, the infrastructure to support trauma centers may not have undergone many changes during the study period (2010-2018). However, in 2019, the annual trauma team readiness cost per level I trauma centers was around $10 million, and for level II trauma centers, it was around $5 million. 2 Although the per-patient cost of trauma care may not have increased as rapidly as that of elective open inguinal hernia repair admissions, it still did increase even when controlling for other potential confounders on regression analysis. Therefore, there is a considerable opportunity to focus on high-value care in trauma, including injury prevention, trainee education, and the implementation of resources and science to curb this substantial rise in trauma health care expenditures.15-17
Interestingly, both urban non-teaching hospitals and urban teaching hospitals had more than 50% higher total charges compared to rural hospitals. This is undoubtedly due to multiple factors that may include increased patient complexity, adverse social determinants of health, and increased penetrating trauma seen in these locations.18-20 Regardless, efforts to promote high-value care in these institutions seem to be especially needed and merit future research (Figure 5). Length of stay in days for elective unilateral open inguinal hernia repair admissions.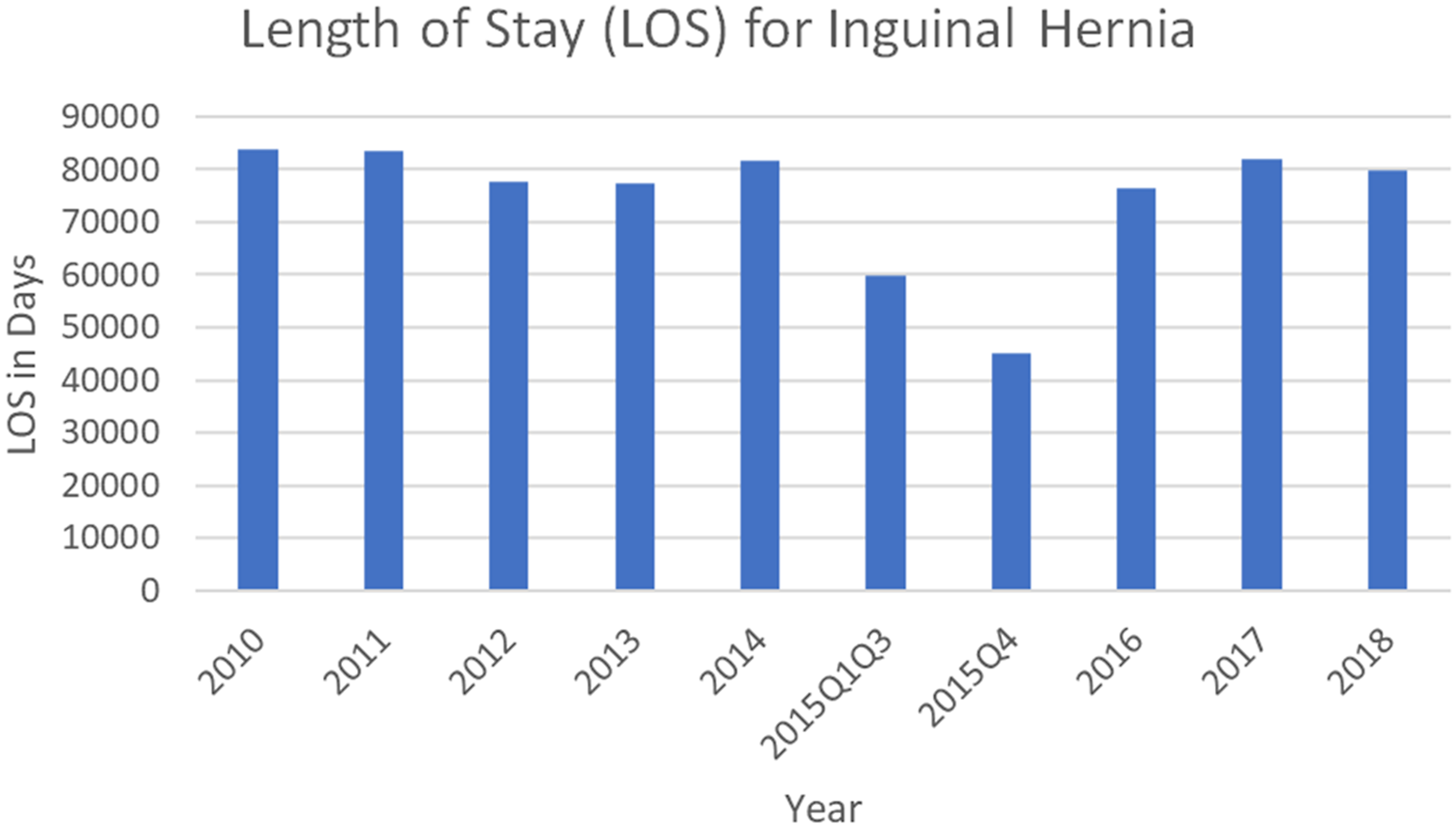
This study has several limitations, including those inherent to a retrospective database design, such as missing data and misclassification. The NIS lacks granular data (ie, cost of implantable devices, cost per night of stay, medications, and imaging) including injury-specific data based on geographic location. Consequently, we were unable to assess outcomes at the county or state level. In addition, this study does not evaluate trauma patients discharged from the emergency department or the majority of hernia repairs that are same-day procedures. Also, the study does not encompass patients treated at centers that did not participate in the NIS.
The NIS also lacks data regarding trauma activation fees, which constitutes another limitation of this study. The authors believe activation fee data should be provided to future iterations of the NIS and other databases to evaluate this factor. In general, health care has increased in cost from $2.6 trillion or $8402 per person in 2010 to $3.6 trillion or $11,172 per person in 2018 within the United States.18 The NIS does not adjust for inflation in the raw data, which is a common limitation for both hernia repair and trauma patients. According to the Bureau of Labor Statistics, the annual inflation rate in 2010 was 1.0% and the annual inflation rate in 2018 was 2.1%, whereas the percentage increase in trauma and inguinal hernia seen in this study was higher. 21
Another limitation is there are fewer trauma centers than facilities performing open inguinal hernia repairs. Notably, the use of cost data presents advantages and disadvantages, with the latter being particularly salient in health care due to substantial disparities between charges and actual costs. Also, costs may not accurately represent the expenses incurred for hospital services, including professional fees charged by physicians. Finally, in 2015 the HCUP transitioned from using the ICD-9 to the ICD-10 coding system, which may have contributed to coding-related increases in that specific year.
Conclusions
Overall, this study demonstrates the total and per-patient cost of trauma care has increased over time. Furthermore, trauma accounts for over $100 billion annually due to a steady increase in per incidence cost and a persistently high rate of trauma in the United States. These findings highlight the urgent need to focus on high-value care to mitigate the escalating costs of elective open inguinal hernia repair and, more importantly, trauma admissions in the United States. Future research should explore potential strategies for cost reduction, such as the optimization of care pathways, investment in injury prevention programs, and the development of more efficient health care systems.
Footnotes
Author Contributions
Drs Anushka Paladugu, Megan Donnelly, Areg Grigorian, and Lourdes Swentek were responsible for the conception and design of the study, along with conducting data collection, analysis, and interpretation, and critically revising the article. Dr Catherine Kuza played a pivotal role in contributing to the conception. Kurt Yamamoto and Jonathan Shipley provided insights during the critical revision process. Dr Ninh Nguyen and Jeffry Nahmias also made substantial contributions by participating in data collection, analysis, and interpretation and securing additional funding for the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.