
Abstract
Background
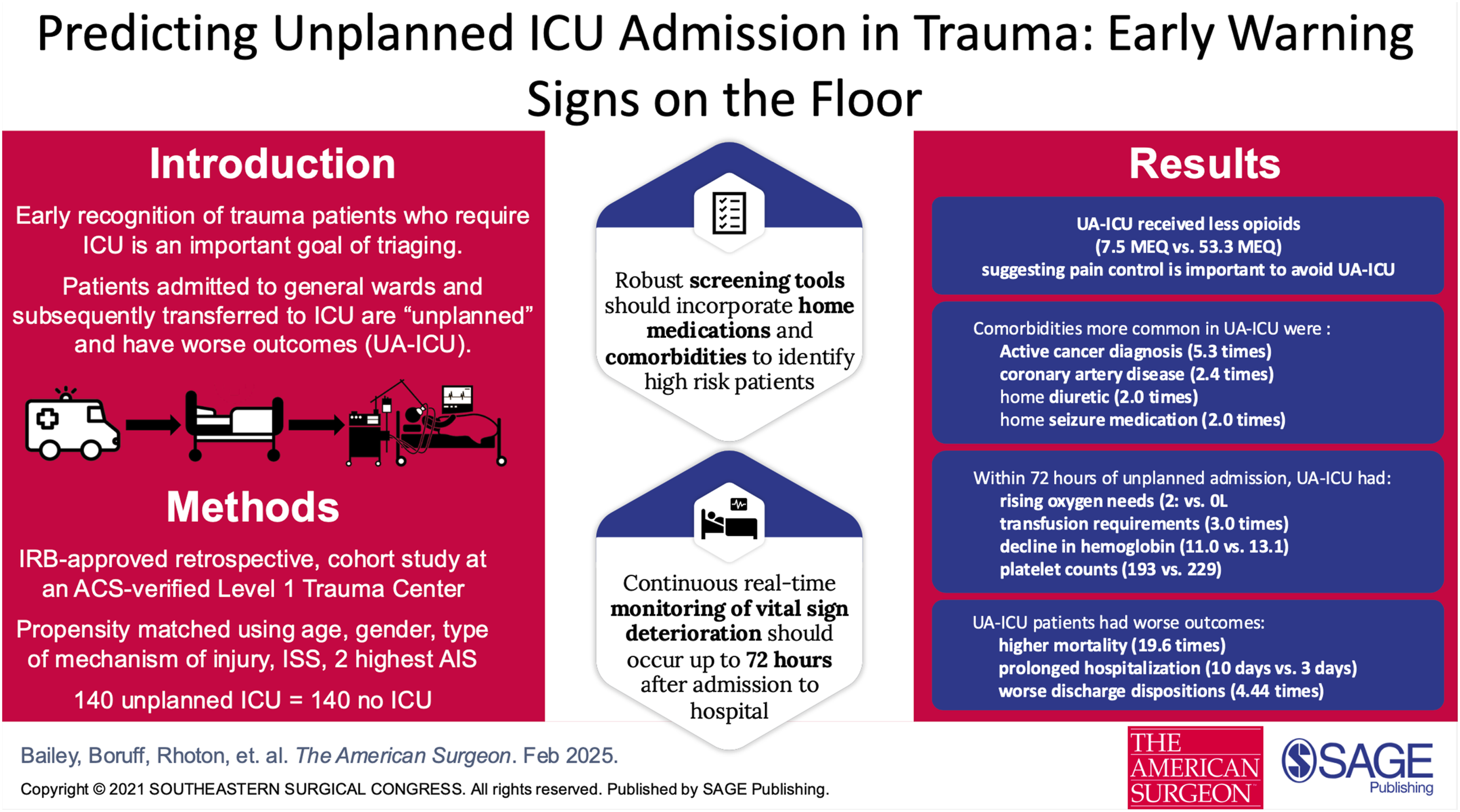
Unplanned ICU admissions (UA-ICU) is a TQIP metric associated with increased morbidity, mortality, and resource utilization. Despite identification of certain predictive factors in prior publications, gaps remain in identifying patients at-risk, particularly once in-hospital and outside the emergency room setting. Our study investigates novel predictors and emphasizes outcomes in UA-ICU for trauma.
Methods
Retrospective cohort study. Single ACS-verified Level 1 Trauma Center (2019-2023). N = 140 UA-ICU after initial non-ICU hospital ward admission and 140 controls never admitted to ICU propensity-matched for age, gender, mechanism of injury (MOI), ISS, and top two highest abbreviated injury values (AIS). We compared variables including demographic, injuries, comorbidities, laboratory, and pharmacology. Statistical analysis was performed utilizing SPSS-28 (Armok, NY) software.
Results
UA-ICU patients demonstrated higher mortality (22.1% vs 1.4%, P < 0.001), longer length of stay (LOS) (10 vs 3 days, P < 0.001), and fewer discharges home (33.6%, P < 0.001). Comorbidity predictors included cirrhosis, active cancer diagnosis, CHF, and home medication for seizure and loop diuretics. Between 48-72 h post-admission, UA-ICU had higher heart rates (107 vs 96 P < 0.001), lower hemoglobin (11 vs 13, P < 0.001), lower platelets (193 vs 229, P = 0.002) and supplemental oxygen requirements (2L vs 0, P < 0.001).
Discussion
Our study affirms established predictors and introduces novel indicators for UA-ICU. Length of stay, discharge other than home, and mortality outcomes are consistent with research linking UA-ICU to prolonged hospitalization and adverse outcomes. Early detection, dynamic monitoring, and interdisciplinary interventions should coalesce to mitigate preventable UA-ICU and conserve resources. We proposed integration of additional predictors into clinical practice/scoring systems to optimize patient outcomes.
Get full access to this article
View all access options for this article.