
Abstract
Background
Patients residing in rural and frontier areas experience worse thyroid cancer outcomes than those in urban areas. This novel qualitative study sought the perspectives of rural surgeons to identify practical measures that could mitigate the disparities in thyroid cancer care between rural and urban contexts.
Methods
We contacted general and head and neck surgeons at all of California’s Critical Access Hospitals (n = 35), which are remote, rural hospitals, and requested self-referral to our study through the American College of Surgeons. We performed semi-structured qualitative interviews with surgeons at rural hospitals to understand the assets and vulnerabilities of rural hospitals in providing the highest quality care to patients with thyroid cancer. Responses were coded and analyzed using mixed-methods qualitative analysis methodology.
Results
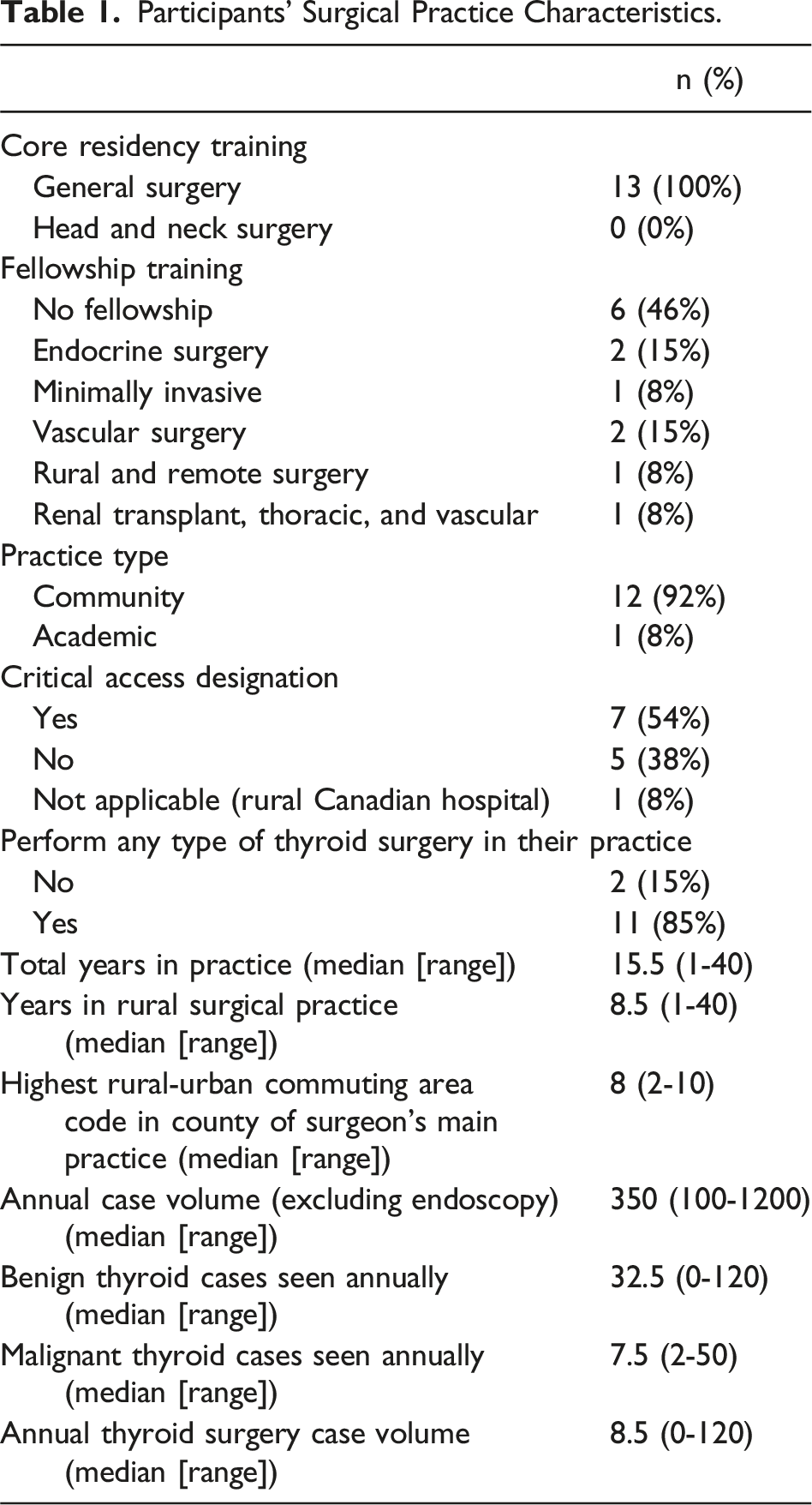
Rural surgeons (n = 13) from a geographically diverse sample of states and regions (AK, AR, CA, NE, NC, NM, TX, UT, WY, and Newfoundland) participated. All initially trained in general surgery; 46% had fellowship training (15% in endocrine surgery) and performed a median of 8.5 thyroidectomies annually.
Rural surgeons from all training backgrounds felt adequately trained to treat thyroid cancer and reported a strong desire to provide comprehensive thyroid cancer care. Most reported patients’ strong preference to be treated near home. Key challenges to local, comprehensive thyroid cancer care included limited or no access to medical endocrinology, lack of continuing education on thyroid cancer management, and professional isolation in decision-making. Interviewed rural surgeons identified connections with university health systems, expert colleagues, and telemedicine consultations as valuable assets in treating thyroid cancer in geographically isolated hospitals.
Discussion
This study identified key challenges and clear avenues for interventions in treating rural thyroid cancer patients. Interviewed rural surgeons specifically suggest improving access to endocrinology specialists, developing educational initiatives on thyroid cancer management, and fostering connections and collaborations with urban colleagues to reduce professional isolation.
Key Takeaways
• Rural surgeons feel well-trained but professionally isolated in treating patients with thyroid cancer. • Rural surgeons specifically suggest improving access to endocrinology specialists, developing educational initiatives on thyroid cancer management, and fostering connections and collaborations with urban colleagues to reduce professional isolation.
Introduction
Rural thyroid cancer patients are diagnosed with later stage disease, more aggressive cancers, are more likely to be lost to follow-up, and have higher disease-specific mortality than their urban counterparts. 1
In tandem, delivery for thyroid cancer has undergone a large change in the past 20 years: patients are increasingly referred to regional centers for surgery by high-volume surgeons at high-volume and specialized centers.2,3 What historically was considered a core surgical procedure of both the general surgeon and head and neck surgeon became increasingly something for which a minimum surgical volume standard needed to be achieved to perform safely.
However, regionalization of cancer care can have unintended consequences, particularly where regional centers are geographically or financially out of reach for patients. Across multiple domains of surgically treated cancers, including brain, bladder, breast, and thyroid cancer, promoting referral to tertiary and quaternary referral centers has had unintended consequences, by concentrating expertise and resources in centers that are not accessible to all, thereby worsening disparities.4-7
Recent work that has demonstrated that the rural and socioeconomically marginalized thyroid cancer patient has been increasingly left behind in the delivery of the highest-quality, evidence-based thyroid cancer care along a host of domains. This qualitative study responded to the urgent need to identify equitable solutions to the observed inequities in care delivery by leveraging the expertise and resources already present in rural health systems.1,7,8
Methods
Institutional Review Board exemption for this study was obtained through the University of California Los Angeles Office of the Human Research Protection Program. We performed semi-structured qualitative interviews with surgeons at rural hospitals to understand the assets and vulnerabilities of rural hospitals in providing the highest quality care to patients with thyroid cancer.
Participants
To be eligible for this study, participants needed to meet all the following criteria: be
To obtain a comprehensive and diverse set of surgeon input, we contacted all general and head and neck surgeons via email and telephone at all of California’s Critical Access Hospitals (n = 35), which are remote, rural hospitals to recruit for this study. We additionally contacted hospital administrators at all California CAHs that do not provide surgical services. We also requested self-referral to our study through the American College of Surgeons state-level and rural surgery communities. Self-referral of additional participants through index study participants was also encouraged. The definition of “rural” practice is used in this study to describe that are designated by the US Census Bureau and Rural-Urban Community Area (RUCA) with codes 4 or higher (micropolitan area core, micropolitan high commuting, micropolitan low commuting, small town core, small town high commuting, small town low commuting, or rural areas).
Data Collection
The thyroid cancer continuum of care is a conceptual model we developed to guide participant’s semi-structured interviews (Figure 1). This model conveys the journey a patient may follow from identification of a cancer through treatment and into survivorship, and it is based off of the most recent American Thyroid Association guidelines for the treatment of thyroid cancer.9,10 This conceptual model was used to structure interviews around the relevant phases of care, and the participants were asked about the assets, deficits, and areas for improvement grounded in each phase. Interviews were conducted via telephone, Zoom, or in person, based on participant preference. Rev artificial intelligence transcription software (San Francisco, 2023) was used to generate manuscripts, which were then manually reviewed and edited for accuracy based on the recording. Thyroid Cancer Continuum of Care, a conceptual model that demonstrates the continuum from recognition of a thyroid nodule through to the cancer survivorship phase.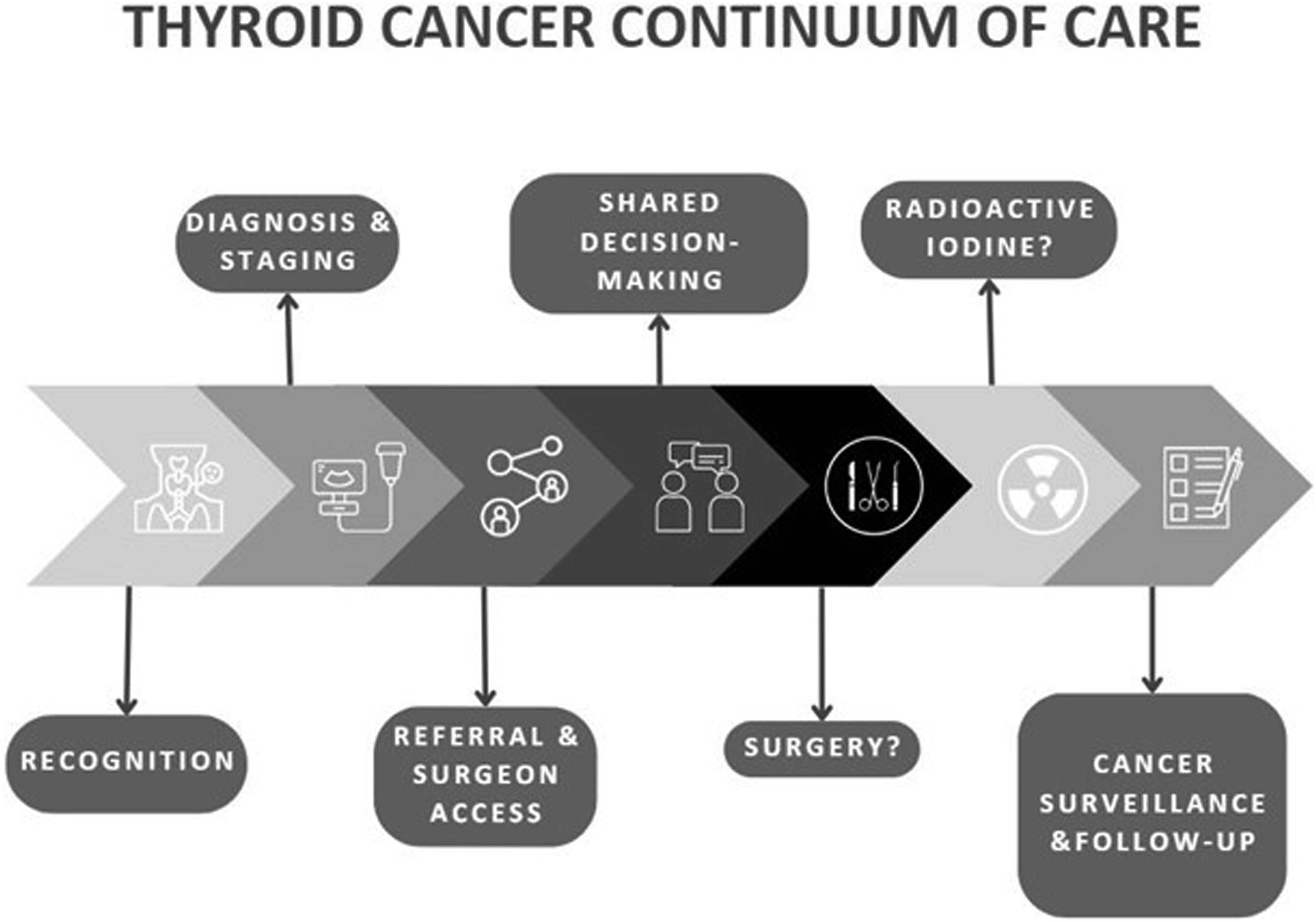
Data Analysis
Responses were iteratively coded by 3 separate researchers (HHP, YVM, and EGH) using Dedoose software (Los Angeles, 2023 v 9.0.57). A final thematic list was generated for the study through multiple iterative reviews of all interviews.
Results
Surgeon Sample
Participants’ Surgical Practice Characteristics.
Thematic Analysis
Thematic analysis identified 4 core themes (Figure 2): Thematic analysis with select subject quotations.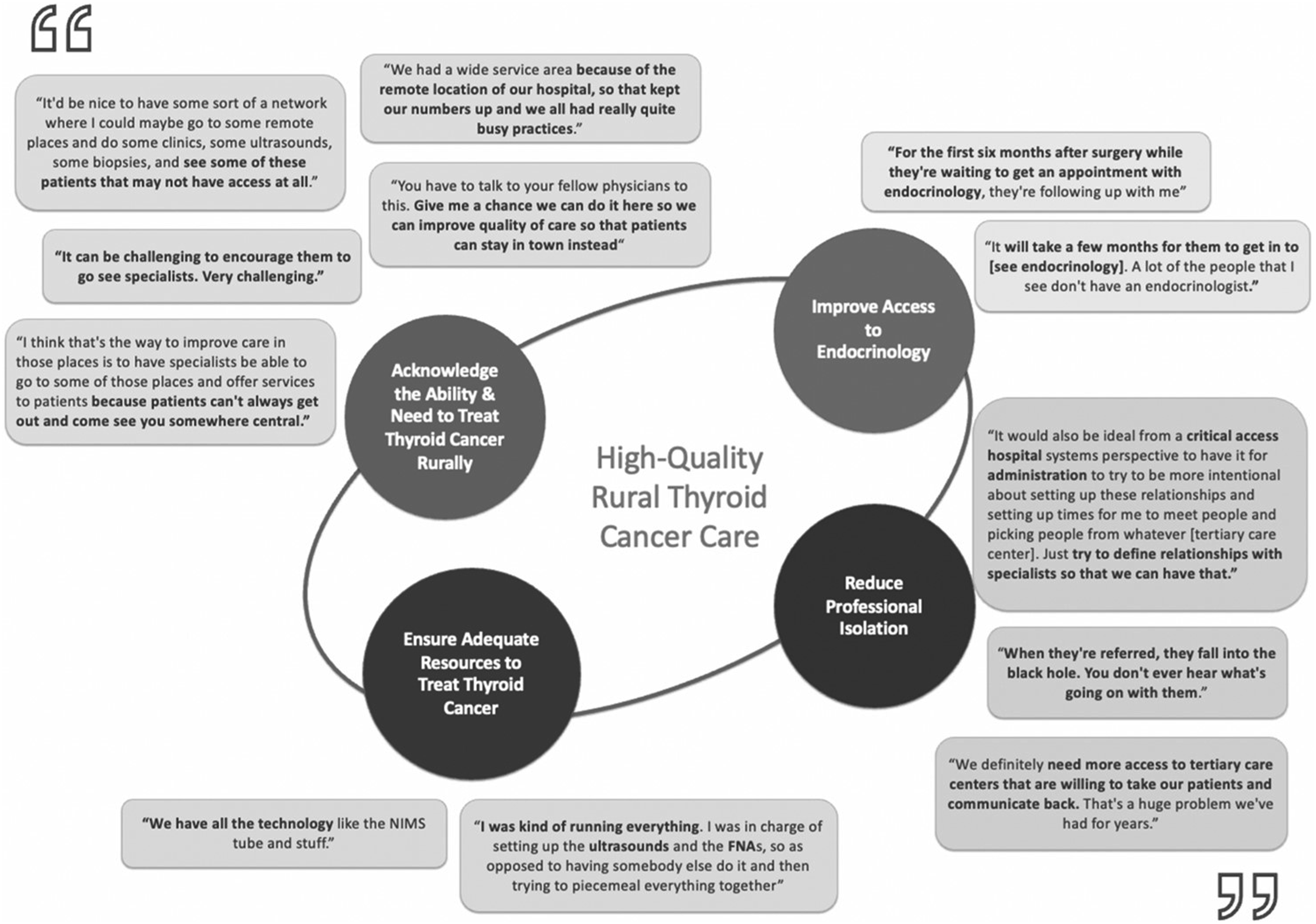
Desire and Ability to Treat Thyroid Cancer
Eleven (84.6%) participants felt adequately trained to treat thyroid cancer and reported a strong desire to provide comprehensive thyroid cancer care: “We did a lot of thyroids, and so I felt very comfortable coming out of residency doing it.” “I trained with [a high-volume thyroid surgeon] in residency, so I was very comfortable doing thyroid and parathyroid.”
High surgical volume across a host of domains, and the innovation and breadth of skills inherent to rural surgical practice were key assets for being able to confidently treat thyroid cancer: “We had a wide service area because of the remote location of our hospital, so that kept our numbers up and we all had really quite busy practices.”
Interviewed surgeons reported the desire to expand offerings to target the known disparities in outcomes among rural thyroid cancer patients: “It'd be nice to have some sort of a network where I could maybe go to some remote places and do some clinics, some ultrasounds, some biopsies, and see some of these patients that may not have access at all.” “The way to improve care in those places is to have specialists be able to go to some of those [remote] places and offer services to patients, because patients can't always get out and come see you somewhere central.”
Some cited that local providers were not referring them thyroid cancer cases that they felt able to do and encouraged communication with local providers to facilitate care close to home: “You have to talk to your fellow physicians about this. Say: “Give me a chance. We can do it here. We can improve the quality of care, so that patients can stay in town instead.”
Patient Preference to Receive Treatment Close to Home
Participants highlighted their intimate knowledge of their rural patients’ preferences and needs to be treated at local hospitals where possible. “It can be challenging to encourage them to go see specialists. Very challenging.” “The biggest challenge is that what we have available right now is centered in [a regional hospital]. So our rural patients … have to travel to [the regional hospital] for those follow-up appointments. […] But I think it’s a lot of transportation. And even though I'll drive [to the regional hospital] for work one day, the patients out there, they don't want to go [there] at all costs. Even for other general surgery procedures that I do, I'll tell them: ‘If you come down to [the regional hospital], I’ll do it on the robot! It’s the most advanced tool that we have!’ And they’re like “I don't care. I don't want to go to [there].”
They were also acutely aware of the social and economic constraints of many of their patients and the corollary need to improve local care to accommodate their unique needs: “Some of those folks didn’t even have electricity to my astonishment when I moved there, nor running water. So it was a challenge for us… there was no telemedicine involved.” “One of the things I’ve learned is that I have to be the local care coordinator, particularly for cancer things, so that people don’t have to be constantly going somewhere else.” “Like a lot of Americans, they’re working paycheck to paycheck. They don’t have a lot of emergency funds, so a lot of them don’t want to take off work, even after an abdominal surgery. They’re like, ‘Can I go to work tomorrow?’ I have to tell them - I have to force them - to even take a week off of work. I think a lot of them can’t afford to take time off work a lot […]They don’t have paid sick leave. They don’t have a lot of options. So I think having constant follow-up [for cancer] or having a bunch of appointments and scans and all these things, it’s just taking away from their income.’
Professional Isolation
Some participants reported longitudinal efforts to build relationships with regional referral centers, including the ability to informally consult colleagues from training or from their regional hubs to consult on difficult cases. This also allowed them to provide both comprehensive pre- and post-operative care to patients who did need to be referred to regional centers for surgery, thereby allowing the patient to stay close to home for the majority of their care continuum. However, many reported feeling professionally isolated, with limited support from regional referral centers: “It would also be ideal, from a critical access hospital systems perspective, to have administration try to be more intentional about setting up these relationships and setting up times for me to meet people and picking people from whatever [tertiary care center]. Just try to define relationships with specialists so that we can have that.”
Several participants reported major gaps in communication and collaboration when they referred thyroid cancer patients to regional hubs: “When they’re referred, they fall into the black hole. You don’t ever hear what’s going on with them.” “We definitely need more access to tertiary care centers that are willing to take our patients and communicate back. That’s a huge problem we’ve had for years.”
Limited Access to Medical Endocrinology
In urban contexts, medical endocrinologists routinely see patients for work up of thyroid nodules, refer to a surgeon when needed, and generally oversee the post-operative adjuvant treatment phase and surveillance for cancer patients. However, 11/13 participants reported very limited or no access to medical endocrinologists in their practice, creating significant bottlenecks: “For the first six months after surgery while they’re waiting to get an appointment with endocrinology, they’re following up with me.” “It will take a few months for them to get in to [see endocrinology]. A lot of the people that I see don’t have an endocrinologist.”
Discussion
This novel qualitative study sought the perspectives and expertise of rural surgeons to understand the root causes of well-documented inequities in outcomes for rural thyroid cancer patients. 1 This study elucidated 4 core themes with corollary actionable policy implications.
Rural Surgeons Are Willing and Able to Treat Thyroid Cancer
Participating rural surgeons felt technically well-trained and capable of providing high-quality thyroid cancer care. Rural surgeons in our study performed a median of 8.5 thyroidectomies per year, which compares favorably to a mean of 5.3 thyroidectomies performed by general surgery chief residents in 2022-2023. 11 Rural surgery is a unique discipline requiring a high level of operative independence, breadth of skill, and complex care coordination abilities. 12 Interviewed rural surgeons reported that they are committed to maintaining a deep breadth of practice, through continuing medical education, and also through the daily practice of meeting an isolated community’s need for advanced surgical skill across many organ systems. 12 Though the urban paradigm of specialization may be more familiar to recent graduates and fellowship-trained surgeons, the demands of breadth and depth in rural surgery must be recognized and respected when considering whether high-quality thyroid cancer surgery is possible in rural hospitals.
Rural Thyroid Cancer Patients Want to be Treated Close to Home
Next, interviewed surgeons nearly uniformly highlighted that their patients prefer to be treated close to home. Studies have corroborated that not only do patients prefer surgical treatment close to home where there is a parity of outcomes between their local hospital and regional centers, 13 but that patients may be willing to accept higher operative mortality14,15 and lower 5-year survival 16 in order to be treated locally. Thus, shared decision-making in the continuum of thyroid cancer care must consider patient preference for treatment location.
Referral to regional centers may be appropriate for select thyroid cancer cases, especially for regionally advanced disease with cancer extending to the lateral nodal basins or the aerodigestive tract. However, many thyroid cancers can be treated close to home if the surgeon feels well-trained. Recent studies suggest that the minimal center volume required to achieve parity of outcomes for thyroid cancer is 5 thyroid cancer cases per year. 7 In this study, the median volume was 8.5 thyroidectomies/year, which, if performed at single hospitals, would meet this lower volume threshold. Local quality improvement initiatives can be implemented in these rural and Critical Access Hospitals to demonstrate to the community and regional partners that patients are receiving the highest-quality thyroid cancer care.17,18
Rural Surgeons Feel Professionally Isolated and Desire Partnerships with Thyroid Cancer Referral Centers
Interviewed surgeons reported that good relationships with surgeons at regional referral centers are central to reducing professional isolation and improving the quality of care that they are able to deliver locally. Though patients may be referred to regional centers for initial management, they may need to be surveilled locally for a host of socioeconomic reasons in addition to patient preference. Regional referral centers that receive surgical consultations for rural-dwelling patients should endeavor to provide dedicated case management to these patients to reduce care fragmentation. Pilot projects have explored the unique case management needs of rural cancer patients: academic centers may consider implementing similar strategies in partnership with rural hospitals.19,20 At minimum, receiving hospitals and surgeons must consider and address the structural vulnerabilities of rural residency, and ensure that there is consistent communication with the referring surgeon in the patient’s area. These discussions and “warm hand-offs” serve as opportunities to build bidirectional collaborations with skilled rural surgeons.
There is a Need for Increased Accessibility of Endocrinology to Improve the Quality of Rural Thyroid Cancer Care
Lastly, many reported that long-waits to see, or the total absence of, medical endocrinologists in rural areas served as a treatment bottleneck in certain cases and, in others, made comprehensive thyroid cancer care difficult. While rural surgeons reported competency with performing their own ultrasounds and fine-needle aspirations in austere contexts, medical endocrinologists typically see patients after surgical excision of a thyroid cancer where multidisciplinary thyroid cancer care is accessible. Some surgeons may also not feel comfortable with comprehensive diagnostic workup of thyroid nodules and would benefit from endocrinology partnership in that regard as well. Care of the patient certainly extends far beyond just the thyroid operation. Medical endocrinologists often oversee the decision to provide adjuvant radioactive iodine treatment, follow biomarkers for cancer recurrence, and determine surveillance strategies in the cancer survivorship phase. Telemedicine opportunities should be enhanced in these rural health systems: collaboration with the well-resourced and high-volume centers that often receive referrals from these hospitals could be explored. Ultimately, developing more collaborative relationships across the rural-urban divide will enhance the ability to provide the majority of thyroid cancer care close to home, while minimizing care fragmentation. 21
Limitations
Rural surgical practices have diverse patient populations with variable health needs, and this study represents only a small proportion of perspectives. Our study was limited by response bias, given that all respondents trained in general surgery residency programs, and we had no response from otolaryngologists. However, the themes that emerged from our study should apply equally to surgeons from both training pathways. Nonetheless, future studies should increase efforts to engage both general surgeons and otolaryngologists. Additionally, multiple treatment models including private hospitals, not-for-profit community hospitals, academic satellite institutions, Indian Health Service facilities, and Veterans Affairs Hospitals will have their own unique sets of resources and corollary constraints. However, this is an important first step in understanding the broad landscape of thyroid cancer surgical care delivery in the rural context. Regional thyroid cancer referral centers may consider performing dedicated outreach to their referring rural colleagues to better understand the unique needs of their rural patient populations. For future studies, we can take the themes identified in this study and survey a larger cohort of critical access rural hospitals to begin to quantify which factors most impede thyroid cancer care in rural settings.
Conclusion
This study identified key challenges and clear avenues for interventions in treating rural thyroid cancer patients. Key challenges to local, comprehensive thyroid cancer care included the following: limited or no access to medical endocrinology, lack of continuing education on thyroid cancer management, and professional isolation in decision-making. Rural surgeons specifically suggest improving access to endocrinology specialists, developing educational initiatives on thyroid cancer management, and fostering longitudinal and bidirectional collaborations with urban colleagues to reduce professional isolation.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Huston-Paterson was supported by the VA Office of Academic Affiliations through the National Clinician Scholars Program. The contents do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.