
Abstract
Background
The COVID-19 pandemic posed significant challenges to healthcare systems worldwide, including surgical care. While many studies examined the effect of the pandemic on different patient outcomes, there are none to date examining the impact of the pandemic surge on surgical outcomes. Our aim is to evaluate the impact of the COVID-19 surges on surgical outcomes using data from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database.
Methods
A single-center retrospective analysis of 7436 patients who underwent surgery between February 2020 and December 2022 was conducted. Patients were divided into those who underwent surgery during the surge of the pandemic (n = 1217) or outside that period (n = 6219). Primary outcomes were 30-day mortality and morbidity. Secondary outcomes included 30-day mortality, operation time, transfusion, reoperation, and specific postoperative complications. Multivariable logistic regression was used in our analysis. All analyses were conducted using the software “R” version 4.2.1. Statistical significance was set at α = .05 level.
Results
After adjusting for confounders, we found no significant difference in 30-day mortality and morbidity (OR: 1.06, 95% CI: .89-1.226, P = .5173) or 30-day mortality only (OR: 1.39, 95% CI: .788-2.14, P = .1364) between the two groups. No significant differences were observed in secondary outcomes. Sensitivity analyses yielded similar results to the multivariable logistic regression.
Conclusion
We found no evidence of increased 30-day mortality and morbidity in patients undergoing surgery during the COVID-19 surges compared to those undergoing surgery outside that period. Our results suggest that surgical care was maintained despite the challenges of the pandemic surges.
Introduction
The COVID-19 pandemic caused by the SARS-CoV-2 virus has had a significant global impact since its emergence in late 2019. 1 As of 2023, there have been over 7 million deaths worldwide, with some even estimating a higher count. 2 Healthcare systems worldwide faced unprecedented challenges during the pandemic, including limited resources, workforce shortages, 3 and increased demands for care. 4
Considerable efforts have been dedicated to evaluating the impact of the pandemic on patient outcomes. A growing body of literature has documented a worsening of surgical outcomes during the COVID-19 pandemic.5-9 Among patients infected with COVID-19 and undergoing surgery, the risk factors for postoperative complications include the time to surgery after COVID-19 infection, 10 vaccination status, 11 comorbidities, 12 male sex, 13 and advancing age. 12 The SARS-CoV-2 virus can cause endothelial damage and immunosuppression, resulting in a higher incidence of postoperative thromboembolism and infectious complications.10,14
Despite the growing evidence of worsening surgical outcomes during the pandemic, there is limited data on the impact of COVID-19 surges on surgical patient outcomes. During such surges, certain hospital services were mandatorily shuttered. Consequently, the effects of restrictions on medical access, 15 increased demands on healthcare systems, and financial burdens on patients during these surge periods remain poorly understood. 16 Furthermore, there is a noticeable lack of extensive, large-scale studies assessing the differences in surgical outcomes between surge and non-surge time frames during the pandemic.
As a result, our study aims to investigate the 30-day postoperative mortality and morbidity in patients who underwent surgery during the COVID-19 surge compared to non-surge periods.
Material and Methods
Study Design and Patient Population
This is a retrospective cohort study conducted at XX. The study includes adult patients who underwent major surgeries between February 1, 2020, and December 31, 2022, and were registered with the National Surgical Quality Improvement Program (NSQIP). Exclusion criteria were patients who underwent minor procedures, such as those requiring sedation or local anesthesia only. Various surgical specialties were considered such as general surgery, vascular surgery, thoracic surgery, otolaryngology, neurosurgery, plastic surgery, and urology. Multiple surgical procedures were assessed within these fields to comprehensively evaluate the impact of COVID-19 surges on patient outcomes. Our study received was deemed exempt by the institutional review board at Beth Isreal Deaconess Medical Center (BIDMC).
COVID-19 Surge Definition
In this study, the COVID-19 surge period is defined as the time when the Massachusetts Department of Public Health mandated the closure of certain hospital services, which resulted in restricted medical access. Three main surge periods were analyzed: the first spanned from March 15, 2020, to June 15, 2020, and the second from December 11, 2020, to March 1, 2021, as well as December 27, 2021, to January 31, 2022. During these three periods, elective and non-urgent procedures were limited at BIDMC.
Data Source
We used data from patients who underwent surgery at our center and enrolled in the American College of Surgeons NSQIP database, a nationally validated program that is risk-adjusted, and outcomes-based, and designed to improve the quality of surgical care. The database collects data from over 700 hospitals throughout the United States. It focuses on objectively capturing surgical outcomes, including morbidity and mortality, within 30 days. Participating hospitals receive detailed reports to support quality improvement initiatives. 17 The study was constrained to data from BIDMC participants in the NSQIP due to the unavailability of information on COVID-19 infection and vaccination status of patients in other centers, which could serve as significant confounders.
Primary and Secondary Outcomes
The primary outcome in this study was the incidence of 30-day mortality and morbidity Secondary outcomes included 30-day mortality only, 30-day thrombotic complications, 30-day hemorrhage complications, and 30-day pulmonary complications. Our null hypothesis was that surgical complications did not increase during the COVID-19 surge compared to the post-surge period during the pandemic.
Covariates
Different covariates related to both patient and surgical factors were considered. Patient factors included age, sex, race, body mass index (BMI), socioeconomic status (type of insurance), American Society of Anesthesiologists Physical Status (ASA-PS), functional status, and comorbidities such as diabetes, hypertension, steroid use, ascites, sepsis, ventilator dependency, malignancy, congestive heart failure, chronic obstructive pulmonary disease, dialysis, and acute kidney injury. Surgical factors included the type of surgery, type of anesthesia, COVID-19 infection status at the time of surgery, operation time, conversion rate, transfusion, reoperation, length of hospital stay, complications, and death. We created a Directed Acyclic Graph (DAG) to identify variables requiring adjustment to estimate in a less biased manner. These variables were COVID-19 Surge (referred to as “Exposure”) and 30-day Complication (referred to as “Outcome”). We adjusted and tested for the minimum number of squared factors necessary to close the open Backdoor Path between Exposure and Outcome (Supplement 1).
Statistical Analysis
We conducted a sample size calculation at first. The reported 30-day complication rate is typically around 3%. Reports indicate that during the COVID-19 pandemic, there has been a postoperative mortality rate of approximately 8%. This suggests that the rate of postoperative complications may increase even further during a pandemic, indicating a conservative calculation. When alpha and power are set to .05 and .9, respectively, and with the Non-surge group and Surge group ratio set at .1, the overall sample size required is 2544, with 2131 participants in the Non-surge group and 213 for the Surge group. Continuous variables such as patient demographics were compared using the t-test, while categorical variables were assessed using chi-square or Fisher’s exact test. We performed multivariable logistic regression to adjust for confounders based on our DAG. Several confounders were identified including age, sex, race, BMI, socioeconomic status, ASA-PS, functional status, comorbidity, COVID-19 infection at the time of surgery, and preoperative COVID-19 vaccination. These confounders were adjusted for in our analysis. To evaluate potential effect modification, such as the COVID-19 variant, we conducted a test for homogeneity. A sensitivity analysis by using multiple imputations for missing values and inverse probability weighting (IPW) for selection bias and confounding was carried out for the primary outcome to assess the robustness of the result. We conducted two-sided tests and considered results with a P-value of less than .05 as statistically significant. Continuous variables are presented as mean (standard deviation (SD)), while categorical variables are denoted as N(%). All statistical analysis was performed using R software version 4.2.1, and a two-tailed P-value of less than .05 was considered statistically significant.
Results
The Trends in the Incidence of Complications in the State of Massachusetts
Our study spanned the period of 2018 to 2022. We observed a temporary increase in the incidence of 30-day postoperative complications immediately following the beginning of the pandemic. However, the incidence of surgical complications fluctuated around the average value in the subsequent period, demonstrating no long-term deviation from the pre-pandemic trend (Figure 1). Trends in the incidence of 30-day mortality and morbidity in Massachusetts.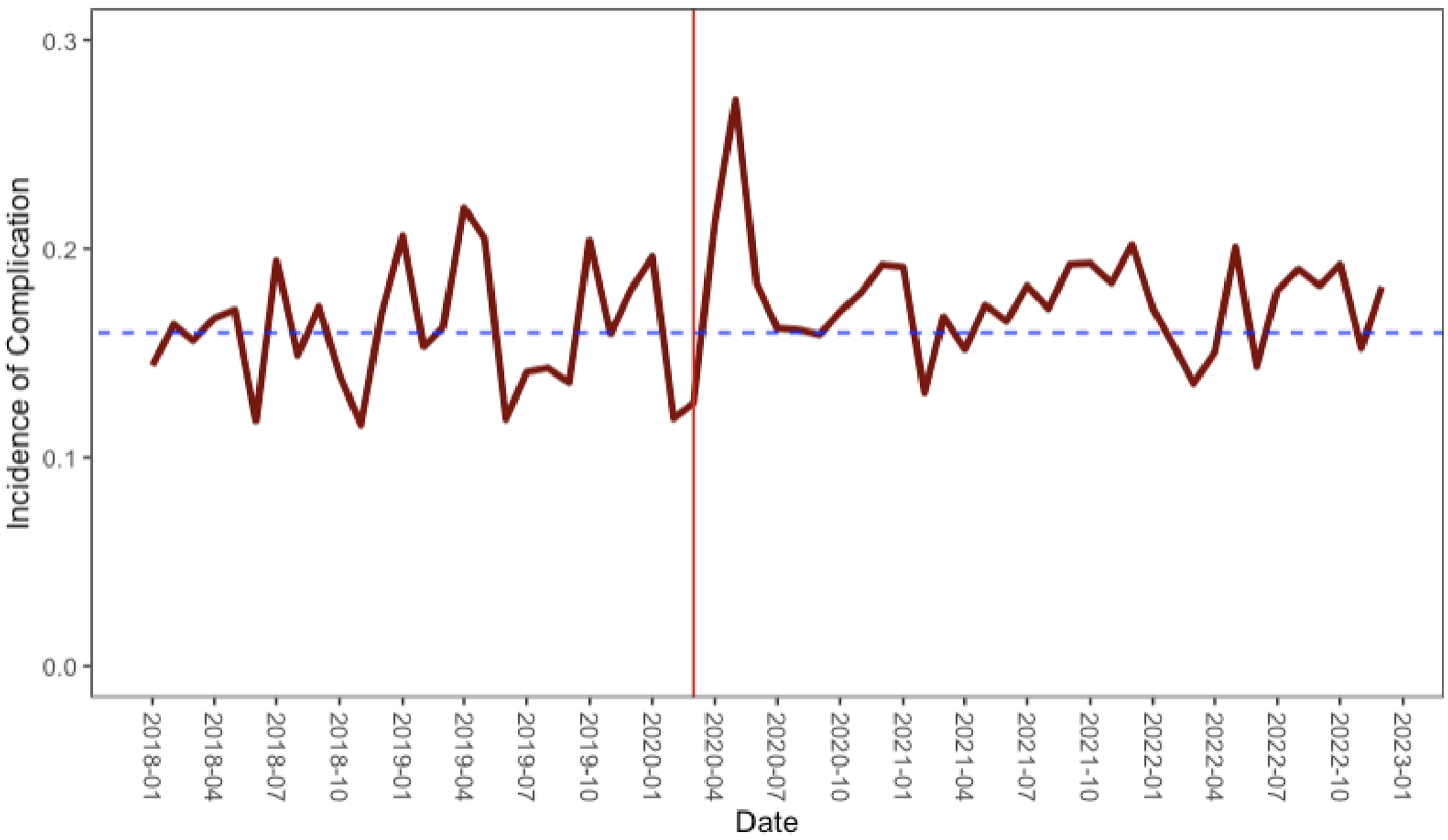
Study Flow
A total of 8078 patients who underwent surgery at BIDMC and were registered in the NSQIP database during our study period were initially identified (Figure 2). Among them, 640 patients met the exclusion criteria previously described and were removed from our analysis. Additionally, two patients were excluded due to a high number of missing data points across multiple variables. Our final study population consisted of 7436 patients, with 1217 patients undergoing surgery during the surge period and 6219 patients during the non-surge period. Study flow.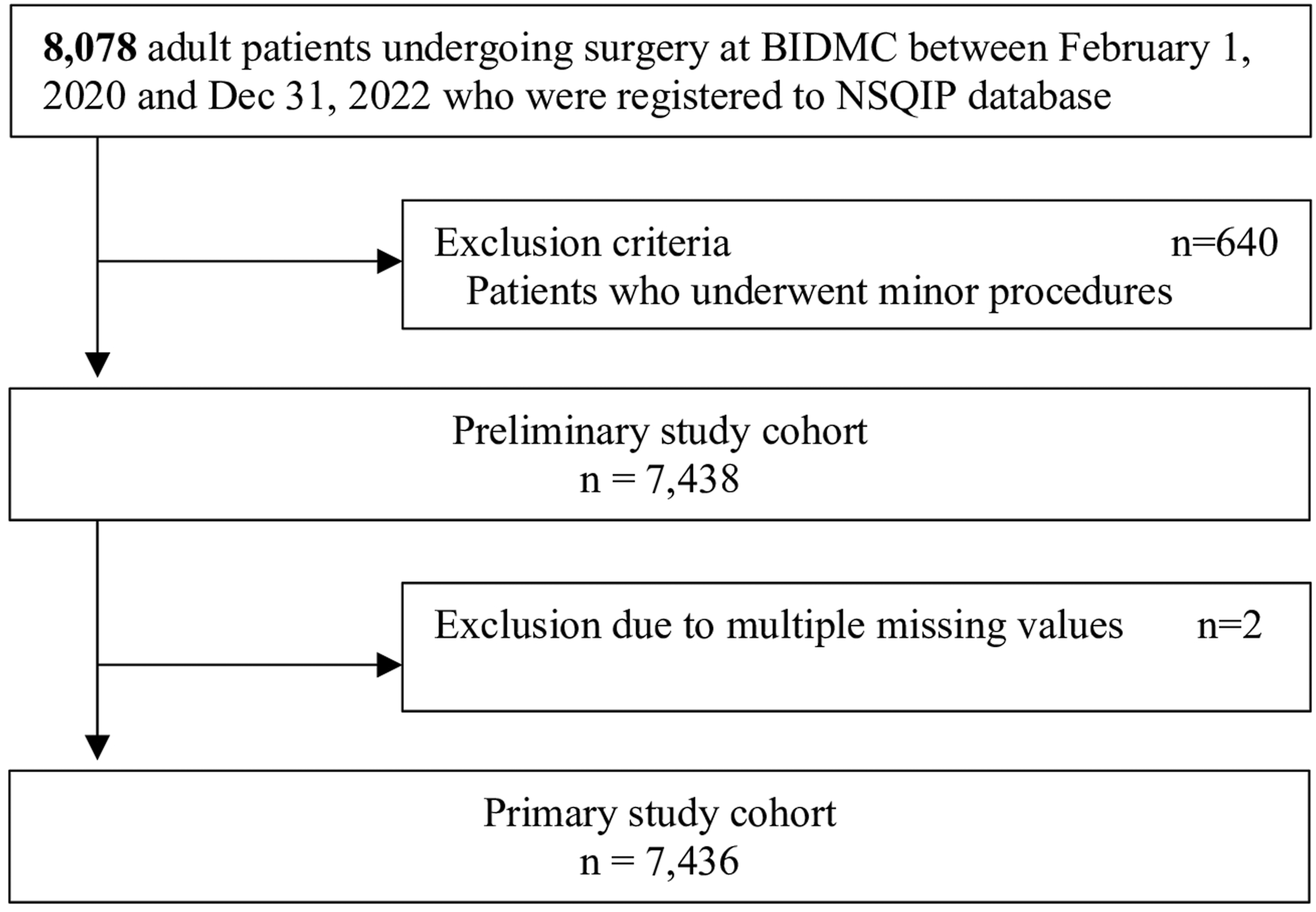
Descriptive Statistics on Baseline Characteristics
Descriptive Statistics on Baseline Characteristics.
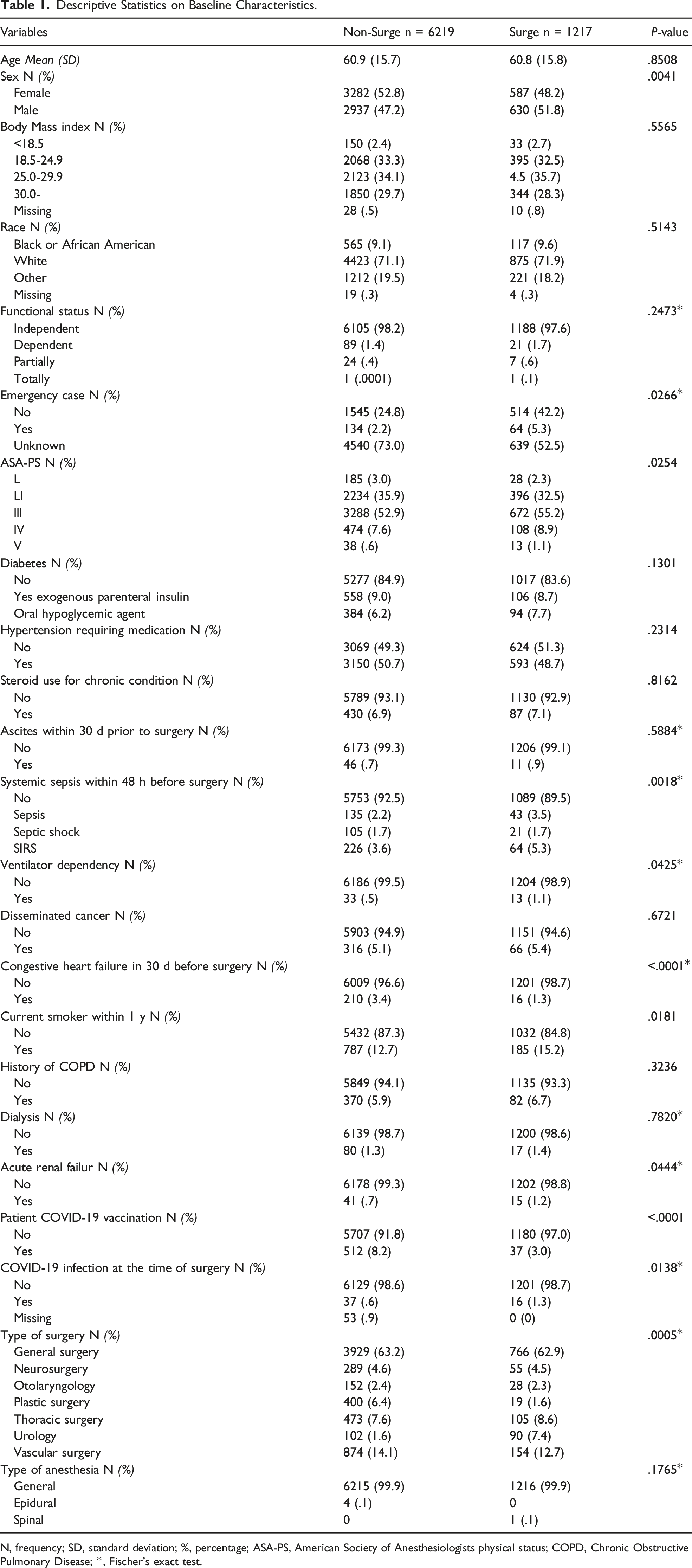
N, frequency; SD, standard deviation; %, percentage; ASA-PS, American Society of Anesthesiologists physical status; COPD, Chronic Obstructive Pulmonary Disease; *, Fischer’s exact test.
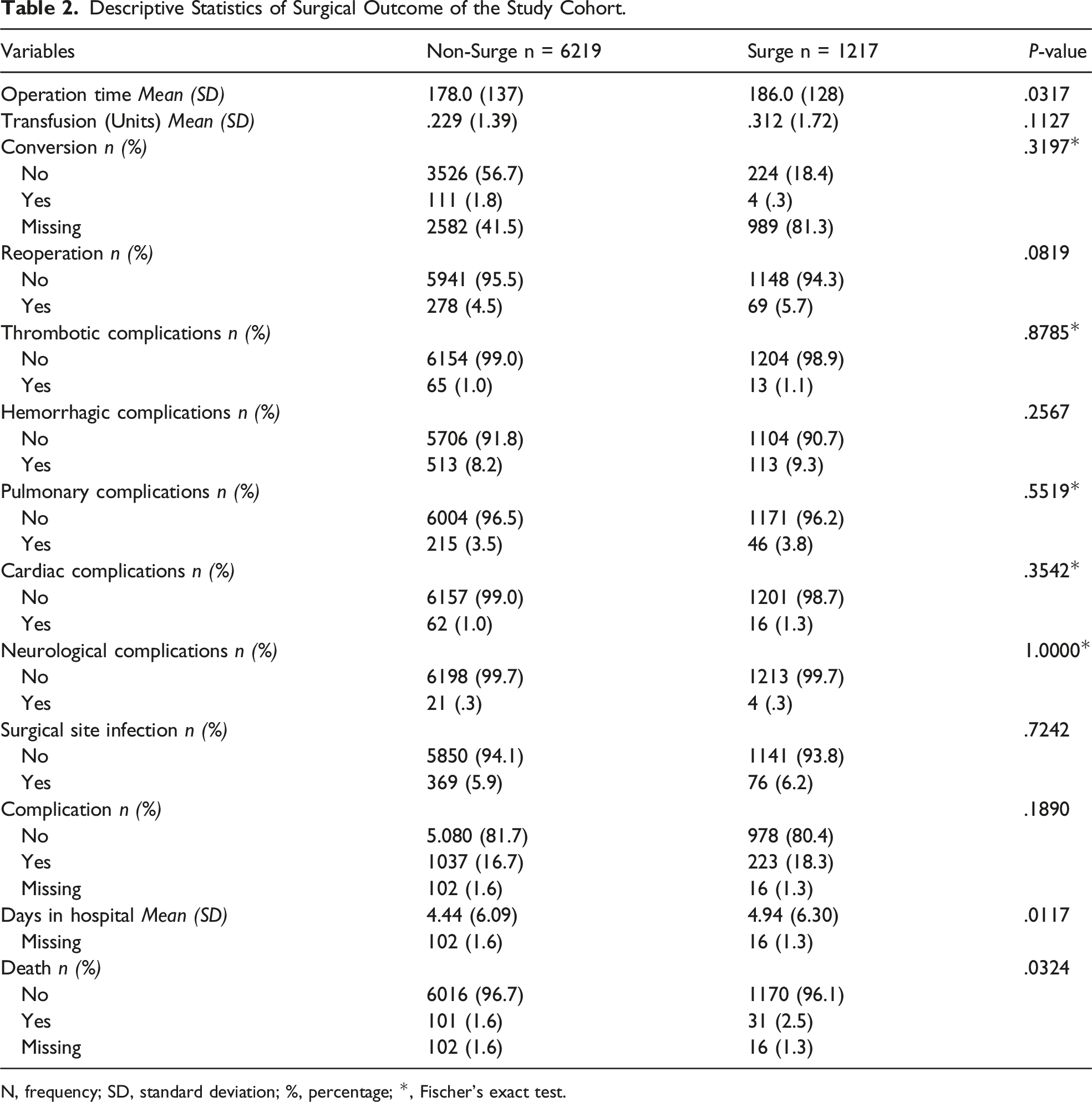
Descriptive Statistics of Surgical Outcomes of the Study Cohort
The difference in the mean operation time for the non-surge and surge groups was statistically significant with 178.0 minutes (SD: 137) and 186.0 minutes (SD: 128), respectively (P = .0317). The difference in the mean number of transfusion units was not statistically significant between the groups, with .229 units (SD: 1.39) for the non-surge group and .312 units (SD: 1.72) for the surge group (P = .1127). The rate of conversion, reoperation, and various complications, including thrombotic, hemorrhagic, pulmonary, cardiac, and neurological complications, did not show any significant differences between the two groups (P > .05). The overall complication rate was comparable between the non-surge and surge groups, with 16.7% and 18.3% respectively (P = .1890). The mean length of hospital stay for the non-surge group was 4.44 days (SD: 6.09) and 4.94 days for the surge group (SD: 6.30), and the difference was statistically significant (P = .0117). The death rate in the non-surge group was 1.6% compared to 2.5% in the surge group, but this difference was also statistically significant (P = .0324) (Table 2).
Main Analysis: Multivariable Logistic Analysis
Primary Outcome
The multivariable logistic analysis showed that the COVID-19 surge was not significantly associated with an increased risk of 30-day mortality and morbidity. (OR 1.06, 95% CI: .89-1.26, P-value .5173) (Table 3).
Secondary Outcomes
Our multivariable logistic regression analysis showed that the COVID-19 surge was not significantly associated with an increased risk of 30-day mortality only (OR 1.39, 95% CI: .88-2.14, P-value .1364). The COVID-19 surge was also not significantly associated with an increased risk of thrombotic complications (OR 1.00, 95% CI: .52-1.78, P-value .9912). Moreover, the COVID-19 surge was not significantly associated with an increased risk of pulmonary complications (OR 1.11, 95% CI: .78-1.53, P-value .5550) (Table 4).
Interaction of COVID-19 Surge and COVID-19 Variant
The interaction analysis of the COVID-19 surges and the Delta variant did not show any evidence of effect measure modification (P-value .1049). There were no patients infected with the Omicron variant during the surge period as well.
Sensitivity Analysis for 30-Day Morbidity
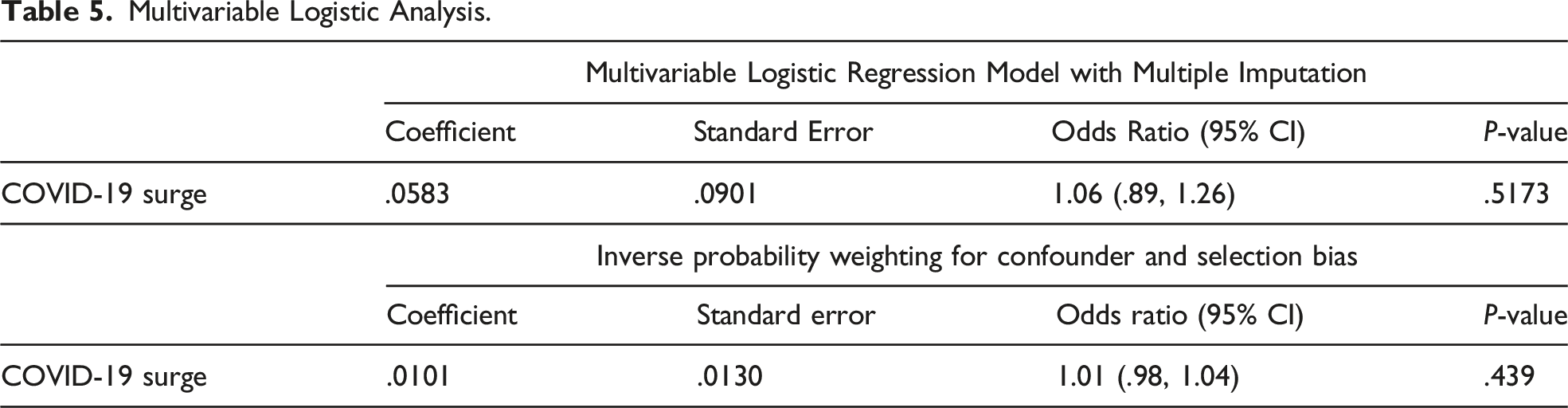
The sensitivity analysis using a multivariable logistic regression model with multiple imputations showed that COVID-19 surge was not significantly associated with an increased risk of 30-day morbidity and mortality (OR 1.06, 95% CI: .89-1.26, P-value .5173). The sensitivity analysis using IPW to adjust for confounding and selection bias demonstrated that the COVID-19 surge was not significantly associated with an increased risk of 30-day morbidity and mortality (OR 1.01, 95% CI: .98-1.04, P-value .4390) (Table 5).
Discussion
Our study investigated the impact of COVID-19 surges on the surgical outcomes of patients during the pandemic. We analyzed 7436 patients, including 1217 who underwent surgery during the surge period and 6219 during the non-surge period. The primary outcome, 30-day mortality and morbidity, and secondary outcome, including 30-day mortality only and various postoperative complications, were not significantly different between the surge and non-surge periods.
We included a large sample size and a diverse range of surgical specialties to obtain a comprehensive assessment of the impact of COVID-19 surges on surgical outcomes. Additionally, our study used the NSQIP database, which is known for its high-quality data and minimal missing values, ensuring a robust analysis of the surgical outcomes. Furthermore, multivariable logistic regression analysis adjusted by confounders selected by DAG and sensitivity analysis, including multiple imputations and inverse probability weighting, allowed for a robust evaluation of the impact of COVID-19 surges on surgical outcomes. Our study thus offers valuable insights into the maintenance of surgical care quality during the pandemic.
Our findings offer novel insights into the repercussions of COVID-19 on surgical procedures since the onset of the pandemic. To date, numerous studies have explored perioperative outcomes in surgery throughout this period. For instance, Doglieoo et al 18 observed that surgical mortality and complications were significantly higher in patients with COVID-19 infections compared to those without immediately after the pandemic started. An international, multi-center cohort study conducted by the COVIDSurg Collaborative 19 revealed an elevated risk of postoperative pulmonary complications and mortality among patients with perioperative COVID-19 infections. In their analysis, 30-day mortality constituted 23.8% of patients who had confirmed COVID-19 infections within seven days before surgery or 30 days post-surgery. Furthermore, pulmonary complications arose in 51.2% of these patients, representing an alarmingly high risk.
While these investigations have provided invaluable insights into the effects of COVID-19 on surgical patient outcomes, 20 there remains a shortage of literature exploring the impact of COVID-19 surges on such outcomes. Surges like these have a multitude of consequences on health care systems, such as limited medical access, 21 heightened patient demand, 22 and staffing difficulties.23,24 Our study investigates the effects of the pandemic surge on surgical care and outcomes, and to our knowledge, no such study has been reported to date. It is noteworthy that our research extends the existing literature by examining a wider range of surgical procedures. Additionally, we employed rigorous statistical methodologies to account for potential confounders and selection bias.
There were no significant differences in surgical outcomes between surge and non-surge periods during the pandemic, which may be attributed to the adaptability and resilience of healthcare systems during the pandemic. Hospitals implemented various measures, such as reallocating resources, rescheduling elective surgeries, and optimizing patient triage, to minimize the impact of COVID-19 surges on patient care.25,26 Furthermore, increased awareness of infection control measures and strict adherence to safety protocols among healthcare professionals could have played a pivotal role in sustaining the quality of surgical care throughout the pandemic. 27 The nursing staff also played an important role in maintaining adequate surgical care during both the non-surge and surge periods, despite facing a staff shortage. Additionally, their expertise can be leveraged to inform healthcare policies and management during pandemics. 28 Field hospitals also serve as a viable solution to manage pandemic surges. Through collaboration between healthcare organizations and government/military personnel, field hospitals can ease the patient burden on large health institutions. Clear communication and cooperation among these entities ensure an efficient and effective response to emergencies and crisis. The use of field hospitals can also provide additional resources and medical staff to address the needs of the affected population. 29
Our study is not without limitations. First, it is a retrospective study, which carries the potential for selection bias. Second, our period of interest is a surrogate of the COVID-19 surge, which is the time when some of the hospital services were mandatorily shut down. Using this surrogate measure could potentially introduce bias; however, we conducted a sensitivity analysis to account for potential bias, and the risk of biased results appears to be minimal. Third, our study was based on data from a single tertiary hospital. This is because data of COVID-19 vaccination history and the presence or absence of COVID-19 infection at the time of surgery was not available from the state-level NSQIP data. Fourth, we did not carry out our analysis on specific procedures but rather a combination of surgical procedures including those in general surgery, plastic surgery, vascular surgery, etc. Further studies are needed to look at the outcomes during the COVID-19 surges but in a procedure-specific manner, which may yield varying findings. Lastly, we did not have access to the nurse-to-patient ratio, any supply shortage data, and surgical difficulty during the surge period, which are relevant to our study. However, these factors acted as mediators rather than confounders on our DAG and should not be adjusted for in the multivariable analysis. The results from the sensitivity analysis appear to confirm this. Despite these limitations, our study provides valuable insights into the impact of the COVID-19 pandemic on surgical outcomes and contributes to the growing body of evidence in this area.
Conclusion
Descriptive Statistics of Surgical Outcome of the Study Cohort.
N, frequency; SD, standard deviation; %, percentage; *, Fischer’s exact test.
Multivariable Logistic Analysis for Primary Outcome.

Multivariable logistic regression adjusted by age, sex, race, body mass index, socioeconomic status, American Society of Anesthesiologists physical status, functional status, comorbidities, COVID-19 infection at the time of surgery, and preoperative vaccination.
Multivariable Logistic Analysis for Secondary Outcome.
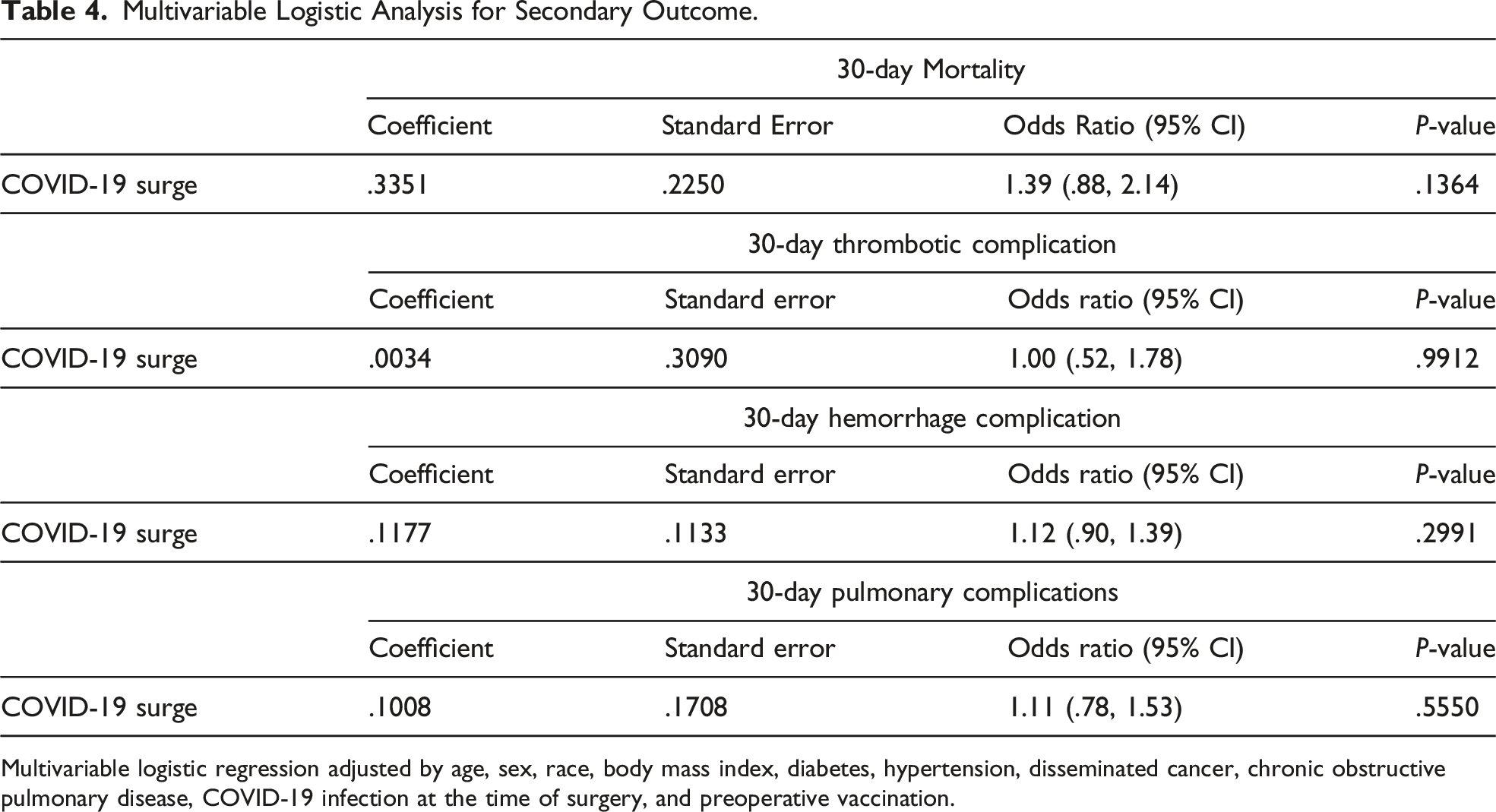
Multivariable logistic regression adjusted by age, sex, race, body mass index, diabetes, hypertension, disseminated cancer, chronic obstructive pulmonary disease, COVID-19 infection at the time of surgery, and preoperative vaccination.
Multivariable Logistic Analysis.
Supplemental Material
Supplemental Material - Impact of COVID-19 Pandemic Surge on Surgical Outcomes: A Retrospective Study
Supplemental Material for Impact of COVID-19 Pandemic Surge on Surgical Outcomes: A Retrospective Study by Takuto Yoshida, MD, MPH, Rosemary Chude-Sokei, MD, MHA, CPHQ, Tarek Araji, MD, and Souheil Adra, MD in The American Surgeon.
Footnotes
Acknowledgments
We would like to express our gratitude to Dr. HJ Baer, Department of Epidemiology, Harvard School of Public Health, Boston, MA, USA. Dr. Baer provided valuable input on study design and statistical analysis.
Author Contributions
Study conception and design: T.Y. and S.A. Data collection and analysis: T.Y. Draft manuscript preparation: T.Y., R.C.K., and T.A. All authors reviewed the results and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.