
Abstract
Background
The abdominal seat belt sign (SBS) is associated with an increased risk of hollow viscus injury (HVI). Older age is associated with worse outcomes in trauma patients. Thus, older trauma patients ≥65 years of age (OTPs) may be at an increased risk of HVI with abdominal SBS. Therefore, we hypothesized an increased incidence of HVI and mortality for OTPs vs younger trauma patients (YTPs) with abdominal SBS.
Study Design
This post hoc analysis of a multi-institutional, prospective, observational study (8/2020-10/2021) included patients
Results
Of the 754 patients included in this study from nine level-1 trauma centers, there were 110 (14.6%) OTPs and 644 (85.4%) YTPs. Older trauma patients were older (mean 75.3 vs 35.8 years old, P < .01) and had a higher mean Injury Severity Score (10.8 vs 9.0, P = .02). However, YTPs had an increased abdominal abbreviated-injury scale score (2.01 vs 1.63, P = .02). On CT imaging, OTPs less commonly had intraabdominal free fluid (21.7% vs 11.9%, P = .02) despite a similar rate of abdominal soft tissue contusion (P > .05). Older trauma patients also had a statistically similar rate of HVI vs YTPs (5.5% vs 9.8%, P = .15). Despite this, OTPs had increased mortality (5.5% vs 1.1%, P < .01) and length of stay (LOS) (5.9 vs 4.9 days P < .01).
Conclusion
Despite a similar rate of HVI, OTPs with an abdominal SBS had an increased rate of mortality and LOS. This suggests the need for heightened vigilance when caring for OTPs with abdominal SBS.
Introduction
Older trauma patients (OTPs), defined as patients 65 years of age or older, currently comprise approximately 15% of all trauma activations in the United States. 1 However, this number is expected to increase as the overall population is aging with an estimated 71 million people older than 65 years old by 2030. 2 The two most common mechanisms of injury in OTPs are falls and motor vehicle collisions (MVCs). The incidence of MVCs has also been increasing with 4.8 million MVCs sustaining injuries in 2020 alone. 3 With increased adherence of seat belt use, there has been an overall decrease in mortality due to MVCs. 4 Nevertheless, the incidence of abdominal seat belt sign (SBS), defined as an abrasion or ecchymosis of the lower abdomen due to a seat belt, has increased, with some reports noting an incidence of 11% in restrained patients who are involved in an MVC.5,6 The abdominal SBS has been shown to be associated with distinct injury patterns and has been used as a marker of injury severity for patients who sustain blunt abdominal trauma. 7 Patients in MVCs with abdominal SBS have been associated with higher rates of solid organ trauma and hollow viscus injury (HVI), than patients without abdominal SBS. 8 However, there is a paucity of data regarding abdominal SBS specifically in OTPs who due to the physiological changes of aging, experience changes to their integumentary and musculoskeletal systems leading to muscle atrophy and increased bruising. This diminishes protection of the abdominal cavity. Additionally, OTPs more frequently take antiplatelet/anticoagulant medications and have less physiologic reserve than younger trauma patients (YTPs). Thus, this study hypothesized that the incidence of HVI and mortality is greater in OTPs than younger adult trauma patients with an abdominal SBS.
Methods
The current study is a secondary analysis of a previous prospective multicenter study 9 and was approved by the Institutional Review Board at each participating center, and a waiver of consent was granted to collect data on trauma patients (age ≥18) with an abdominal SBS who underwent computed tomography (CT) of the abdomen/pelvis with intravenous contrast. Pregnant women and patients who underwent an operation without abdominal CT were excluded. Patients were enrolled at nine trauma centers (8/2020-10/2021). A specific definition of abdominal SBS was not provided to study centers but rather left to the discretion of the treating attending trauma surgeon. Older trauma patients were defined as age 65 years and older and compared with YTPs (18-64 years old). The primary outcome was the incidence of HVI, and the secondary outcomes were in-hospital mortality and length of stay (LOS). Additional outcomes evaluated included intensive care unit (ICU) LOS, ventilator days, packed red blood cell (pRBC) transfusions, post-discharge presentation to the Emergency Department (ED), and hospital readmission
Study data were collected using REDCap 10 and included age, sex, Injury Severity Score (ISS), Abbreviated Injury Scale (AIS) for the abdomen, chest, face, and head, Glasgow Coma Scale (GCS), and vital signs (initial heart rate [HR], maximum HR in 24 hours, initial temperature, maximum temperature in 24 hours, initial systolic blood pressure [SBP], and initial and repeat laboratory analyses). Findings from the abdominal physical examination were collected, including the presence/absence and characterization of tenderness (localized vs diffuse) and guarding. If more than one physical exam was documented, the exam from the most senior member of the trauma team was utilized. Imaging included the results of a Focused Assessment with Sonography in Trauma (FAST) exam and CT abdomen/pelvis. A FAST scan was considered positive if free fluid was identified within the abdomen. The data for each CT was compiled based on the attending radiologist read and included the following: abdominal wall soft tissue contusion (consistent with a soft tissue SBS), free fluid with density in Hounsfield units (HU), bowel wall thickening, mesenteric stranding, mesenteric hematoma, bowel dilatation, pneumatosis, and pneumoperitoneum. Computed tomography scans were reviewed by a senior member of the research team at each institution to ensure concordance with official radiology report and to identify any missed findings. If discrepancies were found, they were discussed and confirmed with the attending radiologist of record (n = 26, 3.4%). A negative CT was defined as the absence of any of the above findings. If a repeat CT abdomen/pelvis was performed, the elapsed time, findings, and whether the repeat CT led to an operation were recorded.
Details of any abdominal operation, including time between ED presentation and operation, whether an HVI was suspected preoperatively, type of operation (ie, laparoscopy vs laparotomy), location and severity of injury (ie, full thickness vs partial thickness) of HVI, and any surgical interventions performed were collected. Data was collected on index hospitalization and a subsequent 30-day post-discharge electronic medical record review.
Hollow viscus injury was defined as the presence of an enteric injury (partial or full thickness) identified during operative exploration. If a patient did not undergo an operation, they were considered negative for HVI.
Statistical Analysis
Descriptive statistics were used to compare OTPs to YTPs and reported as median with interquartile range (continuous), mean with standard deviation (continuous), or count with percent (categorical). Additional comparisons were made between these cohorts using appropriate bivariate tests (t test, Chi-square test, and Wilcoxon rank-sum test) and reported as P-values with significance <.05. Also, multivariable logistic regression analyses were performed to evaluate risk of mortality in OTPs. Variables were selected based on author consensus and included age, ISS, and HVI.
A planned subgroup analysis of OTPs with vs without HVI was also performed with descriptive statistics and bivariate analyses as described above. Analyses were performed in Stata (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC).
Results
Demographics, Patient Characteristics, and Outcomes of OTPs vs YTPs
Demographics, Vitals, Imaging, and Outcomes for Abdominal SBS in Older (
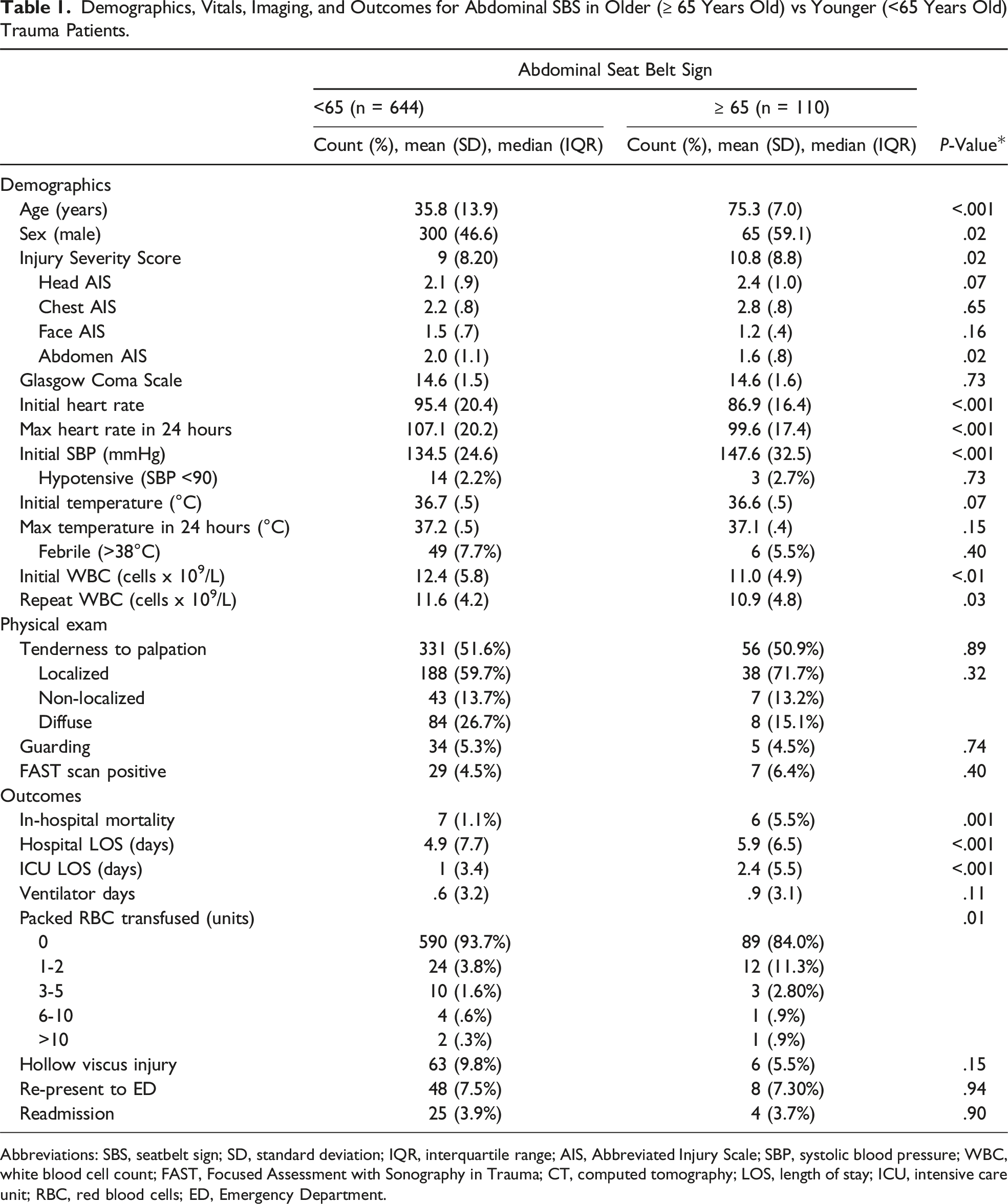
Abbreviations: SBS, seatbelt sign; SD, standard deviation; IQR, interquartile range; AIS, Abbreviated Injury Scale; SBP, systolic blood pressure; WBC, white blood cell count; FAST, Focused Assessment with Sonography in Trauma; CT, computed tomography; LOS, length of stay; ICU, intensive care unit; RBC, red blood cells; ED, Emergency Department.
Operative Findings for Elderly (
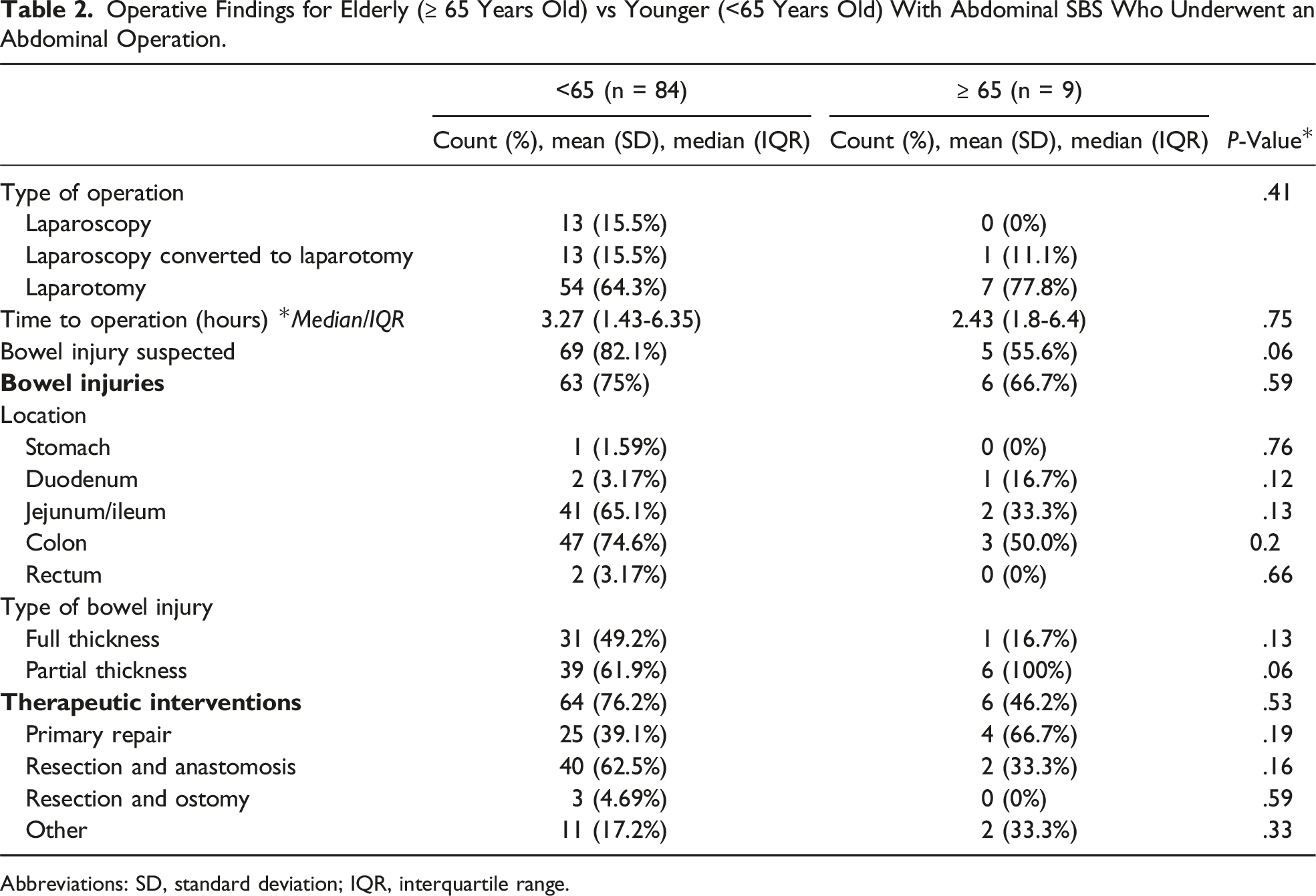
Abbreviations: SD, standard deviation; IQR, interquartile range.
Outcomes of OTPs vs YTPs
Older trauma patients had a higher mortality rate than younger patients (5.5% vs 1.1%, P = .001) (Table 1). There was no significant difference in the rate of HVI in older patients compared to younger patients (9.8% vs 5.5%, P = .15). Compared to YTPs, OTPs had a longer mean hospital LOS (5.9 vs 4.9 days, P < .001) and ICU LOS (2.4 vs 1 days, P < .001). Older trauma patients also more often received a blood transfusion and received a higher quantity of pRBC transfusions than YTPs (40 vs 17, P = .01). On multivariable logistic regression analysis, we found that when compared with YTPs, OTPs with an abdominal SBS had an increased associated risk of mortality (OR 5.20, CI [CI 1.5, 17.8], P = .009], even when controlling for ISS (OR 1.13, CI [1.08, 1.19] P < .001) and HVI. However, HVI was not independently associated with risk of mortality (OR 1.9, CI [.5, 7.5], P = .386).
Comparison of Only OTPs With and Without HVI
Of the 110 OTPs with abdominal SBS, 6 (5.4%) had an HVI. Older trauma patients with HVI compared to OTPs without HVI had a higher mean ISS (21 vs 10, P = .05) and a higher abdominal AIS score (2.8 vs 1.5, P = .004). Compared to OTPs without HVI, OTPs with HVI also had a higher 24-hour maximum HR (114 vs 99, P = .012) and a higher incidence of hypotension on arrival (2 [33.3%] vs 1 [1%], P = .007). Older trauma patients with HVI also had higher rates of abdominal tenderness to palpation (100% vs 48%, P = .047), guarding (33.3% vs 2.9%, P = .01), and positive FAST scans (33.3% vs 4.8%, P = .005).
Demographics and Presentation of Abdominal SBS in Older (>65 Years Old) Trauma Patients With and Without HVI.
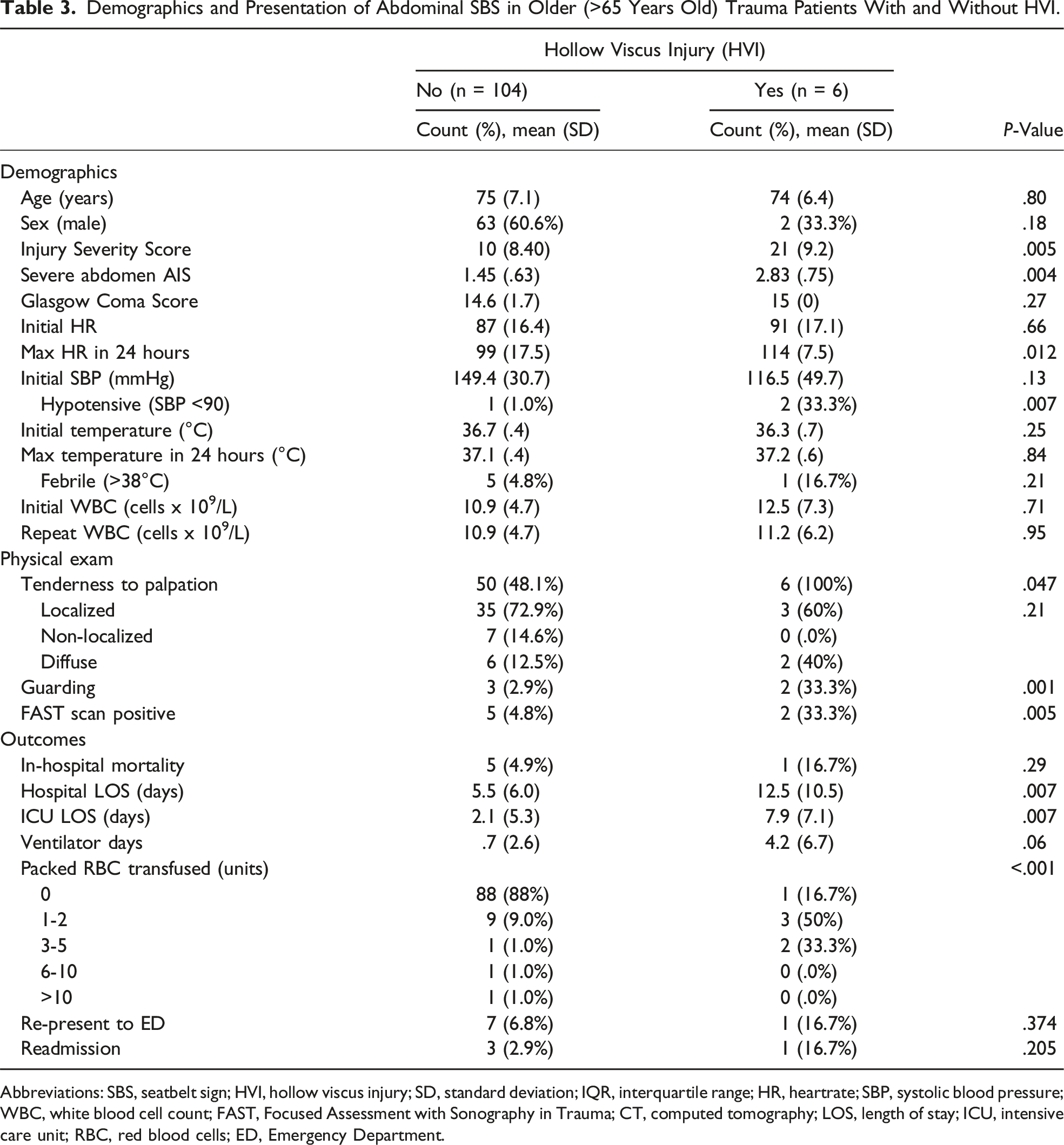
Abbreviations: SBS, seatbelt sign; HVI, hollow viscus injury; SD, standard deviation; IQR, interquartile range; HR, heartrate; SBP, systolic blood pressure; WBC, white blood cell count; FAST, Focused Assessment with Sonography in Trauma; CT, computed tomography; LOS, length of stay; ICU, intensive care unit; RBC, red blood cells; ED, Emergency Department.
Imaging Findings Between Older Patients (>65 Years Old) With and Without HVI.
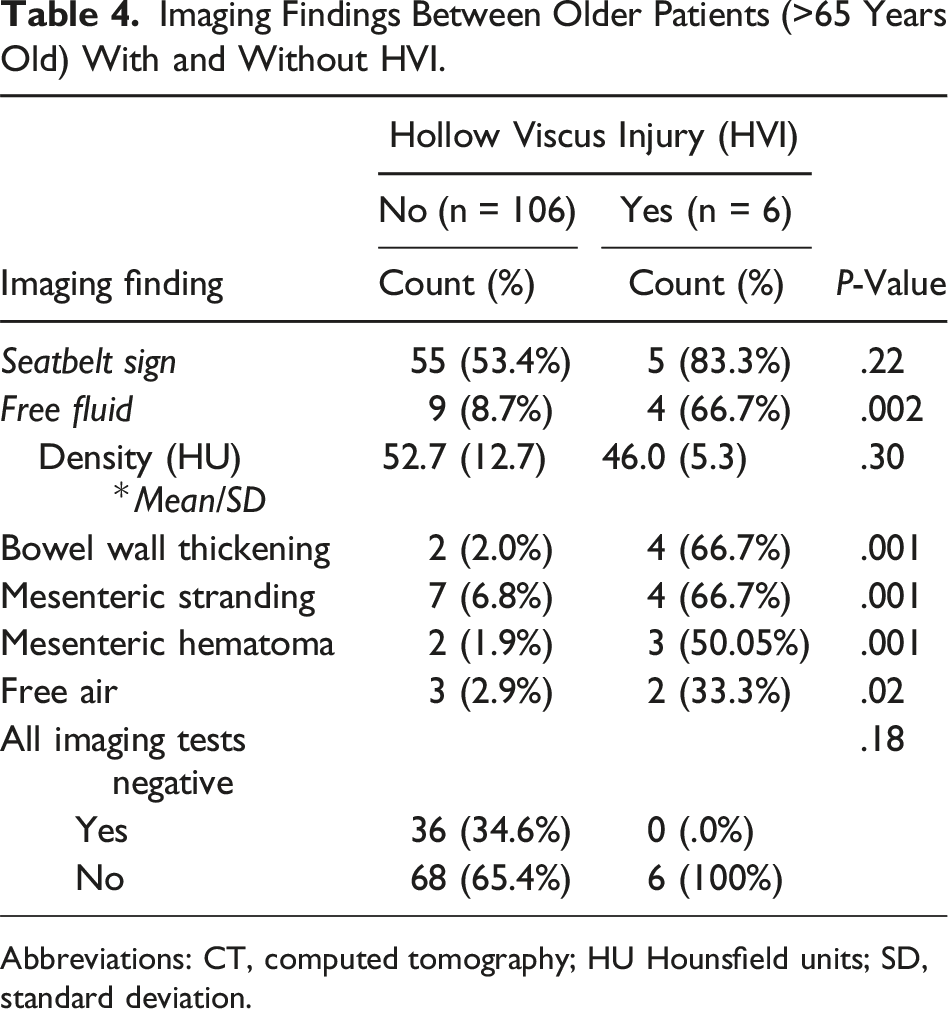
Abbreviations: CT, computed tomography; HU Hounsfield units; SD, standard deviation.
Discussion
Older trauma patients represent a unique and difficult population to manage as they are often under-triaged 11 despite a well-established increased risk of morbidity and mortality compared to younger patients.12,13 Additionally, the combination of physiologic changes of aging and derangements due to baseline comorbidities (eg, medications suppressing HR response like beta blockers and calcium channel blockers, and/or hypertension) may obscure the physical/physiologic findings in OTPs. This may lead to a delay in diagnosis of the sequalae of traumatic injuries (eg, hemorrhage or sepsis). 14 While the majority of the available research in OTPs has focused on injuries such as TBI and hip fractures, the outcomes of OTPs with abdominal SBS have not yet been explored. This multicenter study found that the incidence of HVI in OTPs presenting with abdominal SBS was over 5%. Furthermore, OTPs presented with a higher overall ISS and head AIS than YTPs, despite having no difference in the AIS score for the abdomen, chest, and face. This study also found that the abdominal SBS in OTPs was associated with increased mortality, hospital LOS, and ICU LOS compared to younger adult trauma patients with SBS. In addition, when comparing OTPs with and without HVI, OTP with HVI had an increased maximum HR, incidence of hypotension, and worse outcomes, including increased ventilator days and hospital LOS.
Motor vehicle collisions are the second most common mechanism of injury in OTPs following ground level falls and have a high associated morbidity and mortality in this population.15,16 This study found that, contrary to our hypothesis, the rate of HVI was similar between older and younger trauma patients with an abdominal SBS. However, despite the similar rate of HVI between these two groups, the OTP cohort had an increased rate of mortality compared to YTPs as well as a longer LOS. Furthermore, OTPs with an abdominal SBS continued to have an increased associated risk of mortality even when controlling for injury severity and presence of hollow viscus injury. Therefore, the abdominal SBS in OTPs appears to be a marker of significant injury and risk of mortality in the OTP population and thus should be a pertinent exam finding when evaluating OTPs.
The physiologic changes of aging on the cardiovascular system, pain perception, frailty, and comorbidities of OTPs often cause this patient population to be under triaged. The traditional markers of blood pressure and HR in a trauma evaluation have pitfalls and shortcomings when used for OTPs.17,18 However, when comparing OTPs with and without HVI, there were substantial differences in terms of maximal HR and hypotension. This suggests that, while vital signs may be an imperfect assessment in this age group, any vital sign derangement should lead to heightened concern. Furthermore, the mortality for OTPs with HVI was over three times that of those (16.7% vs 4.9%) without HVI, although this did not quite reach statistical significance, which may be due to a lack of power for this comparison. In contrast, the generalized adult population study by Delaplain et al demonstrated a mortality rate of 6% vs 1.3% for those with HVI compared to those without HVI. 19 As such, HVI in OTPs appears to be a significant factor in the outcomes of OTPs and thus appropriate counseling of patients and/or next of kin should occur.
This study has many limitations including those inherent to its post hoc design, such as a lack of power and important missing data regarding frailty. The latter is a significant limitation as this has been previously demonstrated to better correlate with adverse outcomes in trauma patients. 20 Furthermore, our data did not include prognostic scoring information that has been validated in the older trauma population (eg, National Surgical Quality Improvement Program-Surgical Risk Calculator) which would serve as a better marker and predictor for morbidity and mortality. 21 Additionally, the original study excluded patients who underwent an operation without abdominal CT, thus excluding data from a patient population that would have required immediate operation for HVI. Despite these limitations and the limitations inherent to a prospective, observational study with a small sample size, this study offers vital signs, physical exam findings, and CT imaging characteristics that can be part of a clinician’s toolbox when evaluating OTPs with an abdominal SBS and should heighten the awareness of the increased morbidity and mortality associated with HVI.
Conclusion
This multi-institutional study found that OTPs with abdominal SBS had similar injuries, severity of illness, and rates of HVI compared to YTPs with abdominal SBS. However, OTPs had increased mortality and longer hospital LOS than YTPs with an abdominal SBS, suggesting this population requires increased vigilance by providers caring for these patients and early discussions regarding potential outcomes and goals of care.
Footnotes
This article was presented at ACS Scientific Forum in San Diego, CA, on October 17, 2022.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.