
Abstract
Background
Previous studies suggest increased abdominal girth in obese individuals provides a “cushion effect,” against severe abdominal trauma. In comparison, the unique anatomic/physiological condition of pregnancy, such as the upward displacement of organs by an expanding uterus, may decrease risk of abdominal injury. However, increased overall blood volume and vascularity of organs during pregnancy raise concerns for increased bleeding and potentially more severe injuries. Therefore, this study aimed to elucidate whether the “cushion effect” observed in obese patients extends to pregnant trauma patients (PTPs). We hypothesized a lower risk of blunt solid organ injury (BSOI) (liver, spleen, and kidney) in pregnant vs non-pregnant blunt trauma patients.
Methods
The 2020-2021 Trauma Quality Improvement Program was queried for all female blunt trauma patients (age<50 years) involved in motor vehicle collisions (MVCs). We compared pregnant vs non-pregnant patients. The primary outcomes were incidence of BSOI, and severity of abdominal trauma defined by abbreviated injury scale (AIS).
Results
From 94,831 female patients, 2598 (2.7%) were pregnant. When compared to non-pregnant patients, PTPs had lower rates of liver (5.5% vs 7.6%, P < .001) and kidney (1.8% vs 2.6%, P = .013) injury. However, PTPs had higher rates of serious (13.4% vs 9.0%, P < .001) and severe abdominal injury (7.5% vs 4.3%, P < .001).
Discussion
BSOI occurred at a lower rate in PTPs compared to non-PTPs; however, contrary to the “cushion effect” observed in obese populations, pregnant women had a higher rate of severe abdominal injuries. These data support comprehensive evaluations for PTPs presenting after a MVC.
Level of Evidence
IV (therapeutic).
Key Takeaway
• Blunt solid organ injury (BSOI) occurred at a lower rate in pregnant trauma patients compared to non-pregnant trauma patients. • Pregnant trauma patients have higher rates of severe abdominal injury compared to their non-pregnant counterparts.
Introduction
Trauma remains a leading non-obstetric cause of mortality among pregnant women, with pregnancy presenting unique challenges and concerns for trauma surgeons. Blunt abdominal trauma (BAT) is the most prevalent form of injury within this population, largely attributed to motor vehicle collisions (MVCs). 1 Previously published series have suggested that pregnant trauma patients (PTPs) have almost twice the mortality rate of non-PTPs. 2 This discrepancy can be attributed to the distinctive anatomic and physiological alterations accompanying pregnancy, which can potentially reshape both the injury patterns and the body’s response to trauma. 3
The increased blood volume during pregnancy may increase risk of bleeding and potentially result in more severe injuries with increased transfusion requirements. Furthermore, the relaxation and stretching of abdominal muscles during pregnancy could compromise the protective integrity of the abdominal wall, exacerbating vulnerability to abdominal injuries. 4 In contrast, the gestational redistribution of adipose tissue, especially toward the upper abdomen, may provide a protective mechanism akin to the “cushion effect” seen in obese individuals. 5 In obese patients, a layer of subcutaneous fat has been observed to reduce the severity of abdominal injuries by absorbing some of the impact force. Studies have shown that obese patients often have lower injury severity scores (ISS) and reduced abdominal maximal Abbreviated Injury Scale (AIS) grades compared to leaner individuals. The cushioning effect of subcutaneous fat potentially protects internal organs and lessens the impact of trauma forces.6,7
This study aimed to explore the applicability of the “cushion effect” to PTPs. We hypothesized a lower risk of blunt solid organ injury (BSOI) (liver, spleen, and/or kidney) in PTPs compared to non-PTPs presenting after blunt trauma. 8
Methods
This study was deemed exempt by our local Institutional Review Board as it utilized de-identified data through the American College of Surgeons Trauma Quality Improvement Program (TQIP) database. The 2020-2021 TQIP database was queried for all female blunt trauma patients involved in a MVC. All male patients and females that were not likely of child-bearing age (older than 50 years; median age of menopause) were excluded. Two groups were compared: PTPs vs non-PTPs presenting after MVC.
The primary outcomes were incidence of BSOI, and severity of abdominal trauma defined by AIS. Secondary outcomes included length of stay, in-hospital complications, and mortality. Patient demographic information was collected as well as pre-hospital comorbidities including alcohol use disorder, cirrhosis, chronic obstructive pulmonary disease, cerebrovascular accident, dementia, diabetes, congestive heart failure, hypertension, and current tobacco use. Vital signs on arrival were collected with hypotension defined as systolic blood pressure less than 90 mmHg and tachypnea defined as respiratory rate greater than 22. Trauma injury profile included ISS, revised trauma score (RTS), seat-belt use, location of injury separated by organ system, and severity of abdominal injury defined by abbreviated injury scale (AIS).
Descriptive statistics were performed for all variables with comparison of categorical variables with the chi-square test and comparison of continuous variables with the Mann-Whitney U test. Categorical data were reported as percentages, and continuous data were reported as medians with interquartile range. The study also incorporated a multivariable logistic regression model to assess the associated risk of mortality, with covariates selected by author consensus. Covariates included hypotension, ISS, and age. Risk for mortality was reported with an odds ratio (OR) and 95% confidence intervals (CI). All P-values were two-sided with a statistical significance level of <.05). We additionally performed a propensity-score matched analysis. Matched variables included age, comorbidities, ISS, RTS, vitals and injury burden as measured by the AIS for the head, chest, and abdomen. Patients with similar propensity scores were matched in a 1:2 ratio. We included in our analysis only those cases that were within .001 of the estimated logit (8). All statistical analyses were performed using IBM SPSS Statistics for Windows (version 29, IBM Corp., Armonk, NY).
Results
Patient Demographics, Comorbidities, and Vital Signs on Arrival
Demographics, Comorbidities and Vitals on Arrival for Female patients Presenting After a Motor Vehicle Collision Stratified by Pregnancy Status.
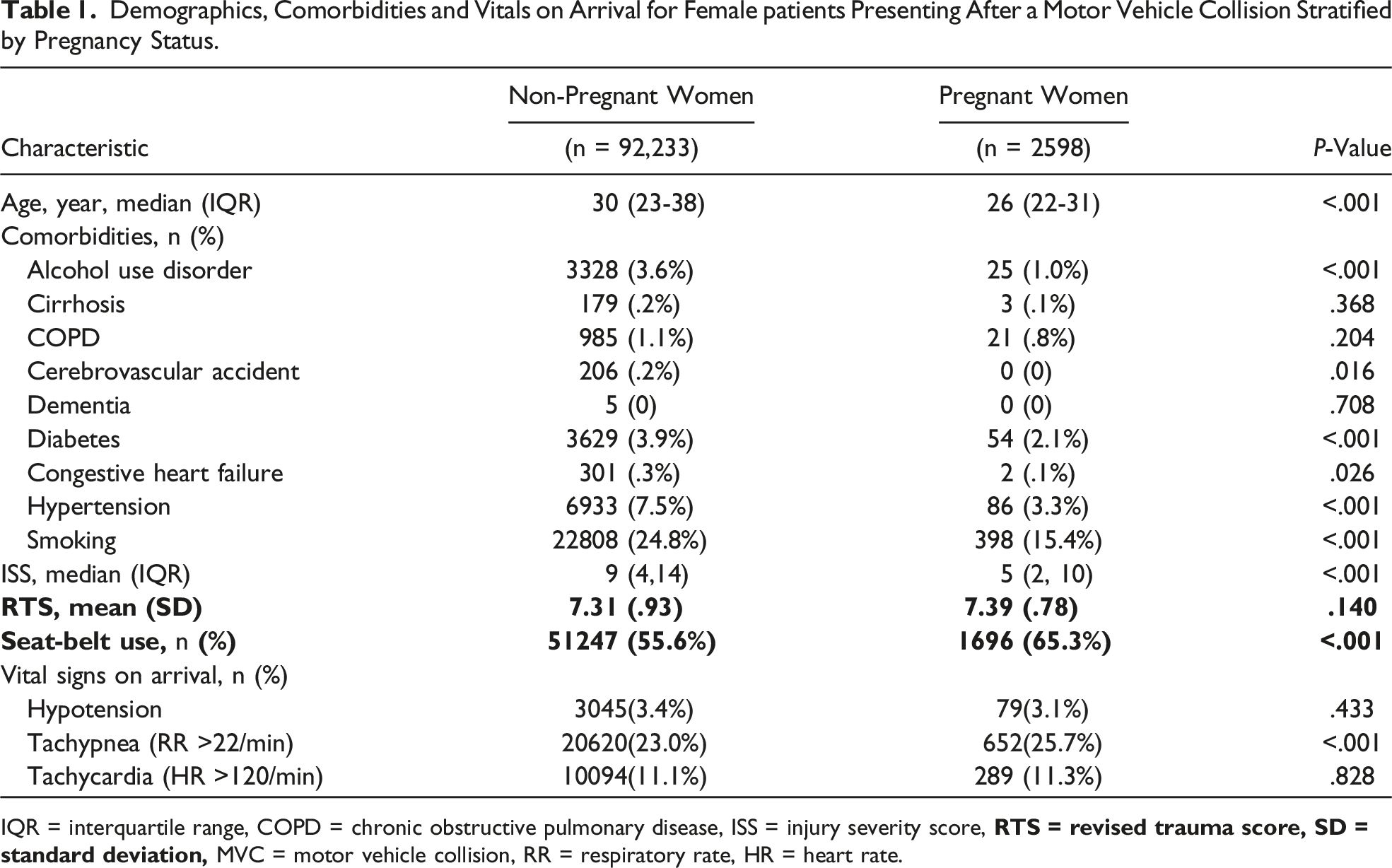
IQR = interquartile range, COPD = chronic obstructive pulmonary disease, ISS = injury severity score,
Injury Profile and Primary Outcome
Injuries Sustained in Female patients Presenting After Motor Vehicle Collision Stratified by Pregnancy Status.
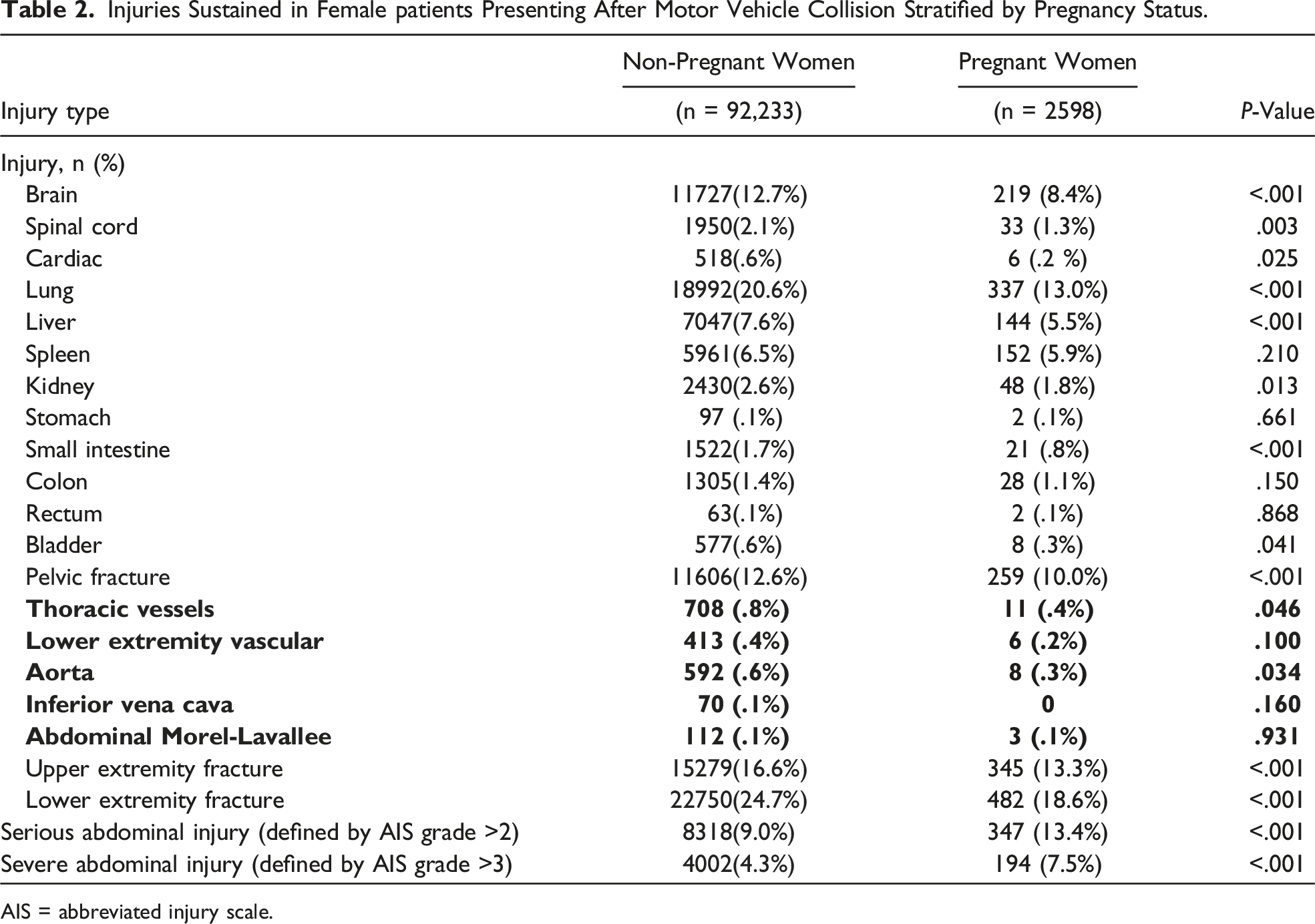
AIS = abbreviated injury scale.
Secondary Outcomes and Complications
Outcomes and Complications for Female patients Presenting After Motor Vehicle Collision Stratified by Pregnancy Status.
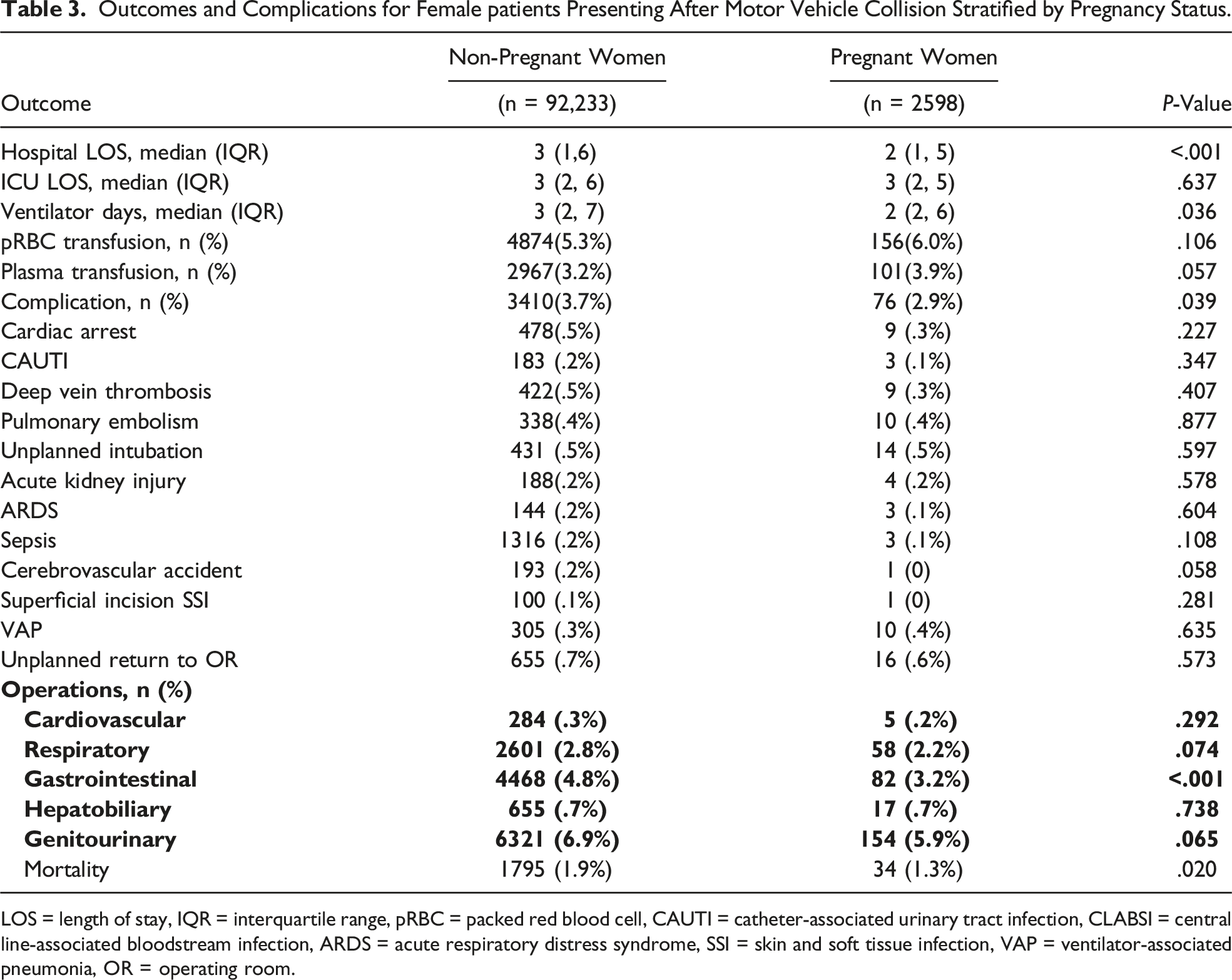
LOS = length of stay, IQR = interquartile range, pRBC = packed red blood cell, CAUTI = catheter-associated urinary tract infection, CLABSI = central line-associated bloodstream infection, ARDS = acute respiratory distress syndrome, SSI = skin and soft tissue infection, VAP = ventilator-associated pneumonia, OR = operating room.
Risk of mortality
Multivariable Logistic Regression Analysis for Risk of Mortality in Pregnant Versus Non-Pregnant Female Patients Presenting After Motor Vehicle Collision.
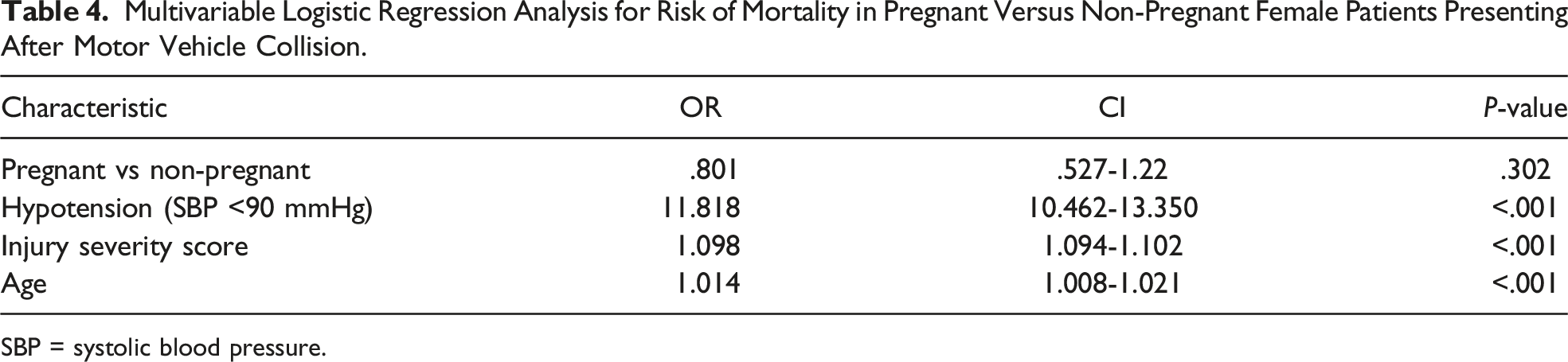
SBP = systolic blood pressure.
Discussion
The escalating incidence of trauma during pregnancy emphasizes the need for trauma centers to develop expertise in managing this unique patient population. This national study revealed that PTPs involved in MVCs presented with lower rates of BSOI, effectively challenging the notion of a protective “cushion effect” with pregnancy. However, in instances where injury does occur, PTPs experienced higher rates of serious and severe abdominal trauma. Interestingly, in contrast to previous studies, this analysis did not reveal a significant difference in terms of rate or associated risk of mortality between pregnant and non-pregnant patients, even when performing a propensity-matched analysis.
Pregnancy may impact the injury pattern and severity of injury after trauma. This study found a lower rate of BSOI in PTPs involved in MVC which invites further exploration into the dynamics of bodily protection and its effect on injury. Recent studies have debated the role of protection provided by subcutaneous fat against injury after MVC. The concept of the “cushion effect” proposed by Arbabi et al 6 in 2003, which suggests that subcutaneous fat acts as a protective buffer, reducing injury severity, is particularly relevant here. 6 This effect is reportedly more pronounced in women due to their naturally higher subcutaneous fat depth compared to men. 7 However, during pregnancy, there may be a decrease in subcutaneous fat thickness, attributed to the tension exerted on the abdominal wall. 9 This might initially suggest a reduced cushion effect in PTPs. Additionally, other unique anatomic changes during pregnancy, such as the upward displacement of organs by an expanding uterus may explain the decrease in BSOI observed in this study. 10 This displacement potentially alters the distribution and absorption of traumatic forces, thereby altering the likelihood or severity of organ injury. The anatomic changes of pregnancy may also explain the lower rate of small intestinal injuries found in PTPs. The displacement caused by an expanding uterus could potentially move parts of the small intestine out of the primary zone of impact in lower abdominal trauma, reducing the likelihood of injury. Furthermore, PTPs may instinctively adopt protective postures during a vehicle accident, such as leaning back further in their seat or holding the steering wheel in a way that minimizes direct abdominal impact. Moreover, pregnant drivers or passengers might inherently drive more cautiously or choose vehicles and seating positions that offer better protection in case of a crash, indirectly reducing the risk of severe abdominal injuries.
Although the rate of BSOI was lower in PTPs vs non-PTPs, we found a higher rate of serious and severe abdominal injury. Similarly, previous authors have shown increased risk of splenic rupture and retroperitoneal hemorrhage in pregnant patients after blunt abdominal trauma.11-14 One potential explanation for this 15 trend could be the augmented pelvic blood flow seen in pregnancy, which may predispose to more severe hemorrhagic complications upon injury. 13 This increased blood flow is not only confined to the pelvic region but is part of a broader circulatory system adaptation where overall blood volume increases by approximately 50% during pregnancy. This expanded blood volume, necessary for fetal support, also means that any vascular injury can lead to more substantial and rapid blood loss, potentially escalating the severity of any hemorrhagic injury. However, this study found no difference in transfusion rates despite increased injury severity in pregnant trauma patients, suggesting other factors may be at play (ie, hormonal, inflammatory, or coagulopathy related), which merits future research. Additionally, TQIP only records blood product transfusions within the first four hours of arrival. This time frame may not fully capture the extent of transfusion requirements, especially for severe injuries that might necessitate ongoing management beyond the initial hours. Thus, while our study did not find a statistically significant difference in early transfusion rates, it is plausible that differences in transfusion needs could emerge when considering a longer period post-admission. And finally, while PTPs did have a higher rate of seat-belt use, there remains room for improvement in promoting consistent restraint use among all pregnant drivers and passengers. More consistent seat-belt use may help decrease the higher rate of severe abdominal injuries observed in PTPs in this study. However, future studies are needed to validate these findings.
The combination of physiological and anatomical changes in pregnancy highlights the difficulty in diagnosing and managing PTPs. It also reinforces the importance of using accurate and effective imaging modalities for timely diagnosis and management. Both the focused assessment with sonography for trauma (FAST) and computed tomography of the abdomen/pelvis (CTA/P) are common imaging modalities to evaluate for intra-abdominal injury in trauma patients. However, CT imaging may be underutilized out of fear of risk of fetal radiation exposure. Currently, imaging protocols for PTPs are not standardized (15). A review of the literature cites an acceptable level of fetal irradiation in the first trimester up to 50 mGy or 5 rad.16,17 Most imaging modalities used as part of the trauma work-up, including CTAP, have fetal radiation well below these levels. 18 While there are no consensus guidelines defining when to perform CT imaging in PTPs, Advanced Trauma Life Support recommends that pregnant patients should be treated the same as non-gravid patients. Our findings demonstrating higher rates of severe abdominal injury in PTPs involved in MVC support the use of CTA/P in this vulnerable patient population as the risk of missed maternal injury and its complications outweigh the small risks of fetal radiation exposure.
The relationship between trauma and maternal mortality, particularly in PTPs, is complex and not yet fully understood, with existing studies presenting conflicting results. Some research, like the Deshpande et al 2019 study, indicates higher mortality rates in PTPs, potentially influenced by their study’s inclusion of a broad range of trauma types and more severe cases. 2 In contrast, studies such as the one by John et al in 2011 suggest lower mortality rates in PTPs, attributed to protective hormonal and physiological changes during pregnancy. 19 Our national analysis, focusing specifically on PTPs presenting after MVC aligns with another database study, which found no significant difference in mortality between PTPs and non-pregnant patients, regardless of the trauma mechanism. 20 These varying findings highlight the need for continued research to better understand and manage trauma outcomes for pregnant women.
There are several limitations to this study, including those inherent to a retrospective database study. These include reporting bias, misclassification, and missing data. In addition, pertinent missing variables include pregnancy trimester and pregnancy related complications. Additionally, the lack of data on post-discharge and patient centric outcomes limits our ability to understand the long-term impact of trauma on both the mother and the fetus. Similarly, the absence of detailed maternal-fetal outcomes/complications in the database restricts our understanding of the direct effects of maternal trauma on fetal health and development. There is also a lack of granular information in the database regarding traumatic abdominal wall hernias, resuscitative efforts, and imaging modalities used in the initial trauma work-up. With lack of specific imaging data, it is possible that injuries were underreported in the pregnant cohort who may have undergone CTAP at lower rates.
Conclusions
While we observed a lower incidence of BSOI in pregnant patients compared to their non-pregnant counterparts, there was a notable increase in the rate of severe abdominal injuries. This finding challenges the notion of any “cushion effect” in pregnant trauma patients and highlights the complexity and unique nature of trauma in pregnancy. While nothing should replace clinical judgment, there are a variety of factors that should be considered when considering the appropriate initial trauma work-up (ie, CT imaging) including the dynamic physical exam and hemodynamic stability. However, our study highlights the necessity of not allowing the fear of radiation to deter essential diagnostic evaluations in PTPs, particularly when we observed a higher rate of severe abdominal injuries in PTPs presenting after a MVC.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.