
Abstract
Key Takeaways
• The HVI score has high negative predictive ability at the low-risk (HVI score ≤5) and high-risk (HVI score ≥10) cutoff points, with a helpful 50% positive predictive value for high-risk patients. • Patients at moderate or high risk for HVI may benefit from earlier identification and management of HVI with use of the HVI score.
Introduction
The proper use of a seatbelt reduces the overall morbidity and mortality of injuries caused by motor vehicle collisions (MVCs). 1 However, seatbelt use has also introduced a unique pattern of intra-abdominal injuries, often marked by the presence of an abdominal seat belt sign (SBS). An abdominal SBS, defined by abrasions or contusions on the anterior abdomen after a collision, has been correlated with an increased risk of hollow viscus injury (HVI). 2 HVI encompasses enteric injuries ranging from partial thickness damage to full thickness perforation of the stomach, small intestine, or large intestine. Previous historical reports have indicated a wide range of HVI incidence rates following SBS, varying from 15% to 64%.2-4 More contemporary studies, however, have found incidence rates between 5% and 9% in patients with an abdominal SBS.5-7
Despite their overall rare occurrence, HVIs can result in significant complications and may become life-threatening if diagnosis and intervention are delayed. A 2018 systematic review conducted by Harmston et al demonstrated that morbidity significantly increased with longer delays in diagnosing and treating HVIs, while an early operation significantly decreased the mortality rate of patients with HVIs. 8 Similarly, Mingoli et al emphasized that delays beyond 6 h between presentation and surgical intervention were independently associated with worse clinical outcomes. 9 Despite this, trauma surgeons have been challenged by the difficulty in diagnosing HVI after blunt trauma. The clinical presentation can be variable, and mesenteric injuries may occur without immediate physical signs of peritoneal irritation.
The Hollow Viscus Injury Prediction Score.
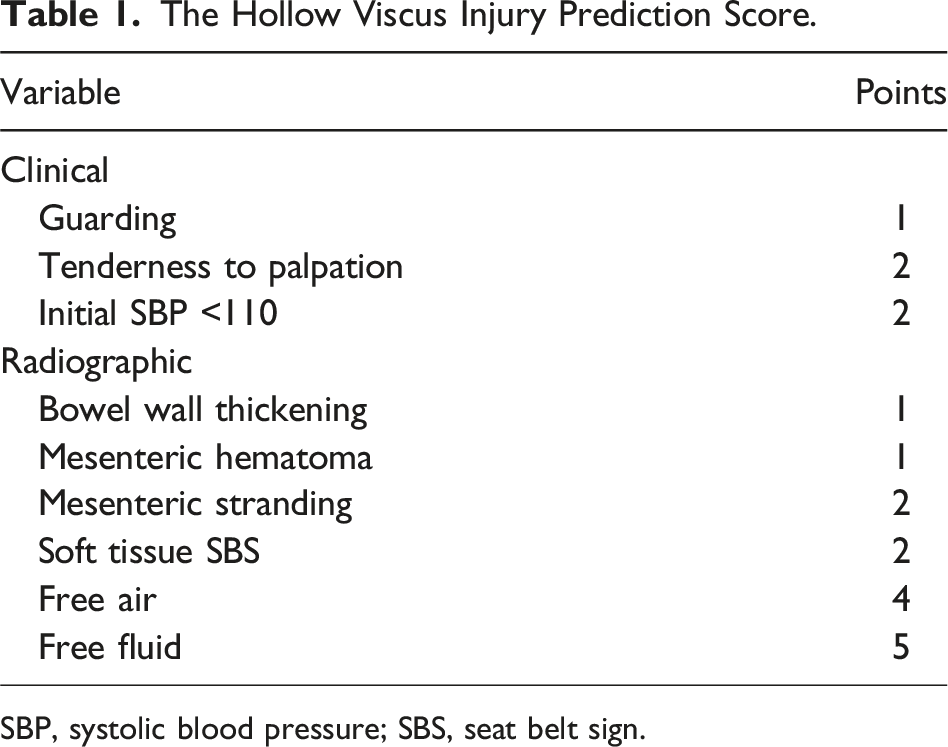
SBP, systolic blood pressure; SBS, seat belt sign.
However, it remains unclear whether applying this novel scoring system would significantly alter clinical decision-making in practice. Therefore, the objective of this retrospective, single-center study was to evaluate how the use of the HVI score would influence clinical management in trauma patients with an abdominal SBS. We hypothesized that the HVI score would lead to changes in management, particularly for higher risk patients, by prompting repeat imaging or earlier surgical intervention in cases of suspected HVI.
Methods
Institutional Review Board approval was obtained, and a waiver of informed consent was granted for this single-center retrospective study conducted between August 2020 and October 2021. This study included adult trauma patients (18 years of age and older) presenting with an abdominal SBS following an MVC. Abdominal SBS was defined as a skin abrasion and/or contusion located on the anterior abdomen, including the anterior superior iliac spine, identified during physical examination by the treating trauma surgeon. All patients were required to have undergone a contrast-enhanced CT scan of the abdomen and pelvis before any abdominal surgical intervention. Pregnant patients and those under the age of 18 were excluded from the study.
Charts of all patients were reviewed to ensure each of the following variables from the HVI score were documented: initial systolic blood pressure upon emergency department (ED) arrival, the presence or absence of guarding and tenderness to palpation on physical examination, and the presence or absence of CT findings including bowel wall thickening, mesenteric hematoma, mesenteric stranding, soft tissue SBS, free air, and free fluid. In total, 6 patients were excluded due to missing data, which led to a final analysis cohort of 239 patients.
Patients in the final cohort were stratified into 3 risk categories based on their calculated HVI risk score: low risk (scores 1-5), moderate risk (scores 6-9), and high risk (scores 10-17). These cohorts were compared for demographics, CT findings, and clinical outcomes. Management recommendations for each risk group were derived from the HVI score, with low-risk patients recommended for observation, moderate-risk patients recommended for repeat CT imaging or diagnostic laparoscopy/laparotomy, and high-risk patients recommended for diagnostic laparoscopy/laparotomy.
The primary objective of the study was to assess how frequently the use of the HVI score would have altered management for this retrospective cohort of trauma patients with abdominal SBS. The patients’ initial management was compared to the management recommended by the HVI score. A deviation from recommended management was defined as a failure to implement the suggested intervention within 6 h of ED arrival. For low-risk patients, deviation was defined as failure to undergo observation within the first 6 h of arrival. For moderate-risk patients, deviation included the absence of a repeat CT scan or diagnostic laparoscopy/laparotomy within the specified six-hour timeframe. For high-risk patients, failure to perform diagnostic laparoscopy/laparotomy within 6 h was considered deviation from recommended management.
For patients whose management deviated from HVI score recommendations, the presence of HVI was confirmed intraoperatively based on a partial or full thickness enteric injury (this did not include isolated mesenteric injuries without partial or full thickness enteric injury). Patients who did not undergo surgery were considered negative for HVI. Since the HVI score mandates specific management at low-risk and high-risk scores, but only strongly recommends either a repeat CT or diagnostic laparoscopy/laparotomy for moderate-risk scores, cutoff HVI scores ≤5 (low risk) and ≥10 (high risk) were used to calculate negative predictive value (NPV) and positive predictive value (PPV) at both of these points. Statistical analyses were performed using IBM SPSS Statistics Version 26.0 and included mean, standard deviation, Kruskal-Wallis tests, chi-square tests, one-way analysis of variance (ANOVA), negative predictive value, and positive predictive value. Statistical significance was defined as a P value <.05.
Results
A total of 239 trauma patients with abdominal SBS following an MVC were included in the analysis. Among the total patient population, 51.9% (n = 124) were female and 48.1% (n = 115) were male. The median age was 35 years old (interquartile range 25-55). There were no significant differences in age (P = .36) or sex distribution (P = .09) between the 3 risk groups (low risk, moderate risk, and high risk).
As anticipated, patients in the high-risk cohort had increased rates of abnormal vitals, physical exam, and CT findings compared to the low-risk and moderate-risk cohorts. Specifically, patients with high-risk HVI scores had lower mean systolic blood pressures (high risk 123.5 mmHg vs moderate-risk 144.7 mmHg vs low-risk 145.2 mmHg, P = .001) and increased findings of tenderness to palpation (high risk 87.5% vs moderate risk 79.4% vs low risk 19.5%, P < .001).
Patient Characteristics and Predictor Variables for Hollow Viscus Injury.
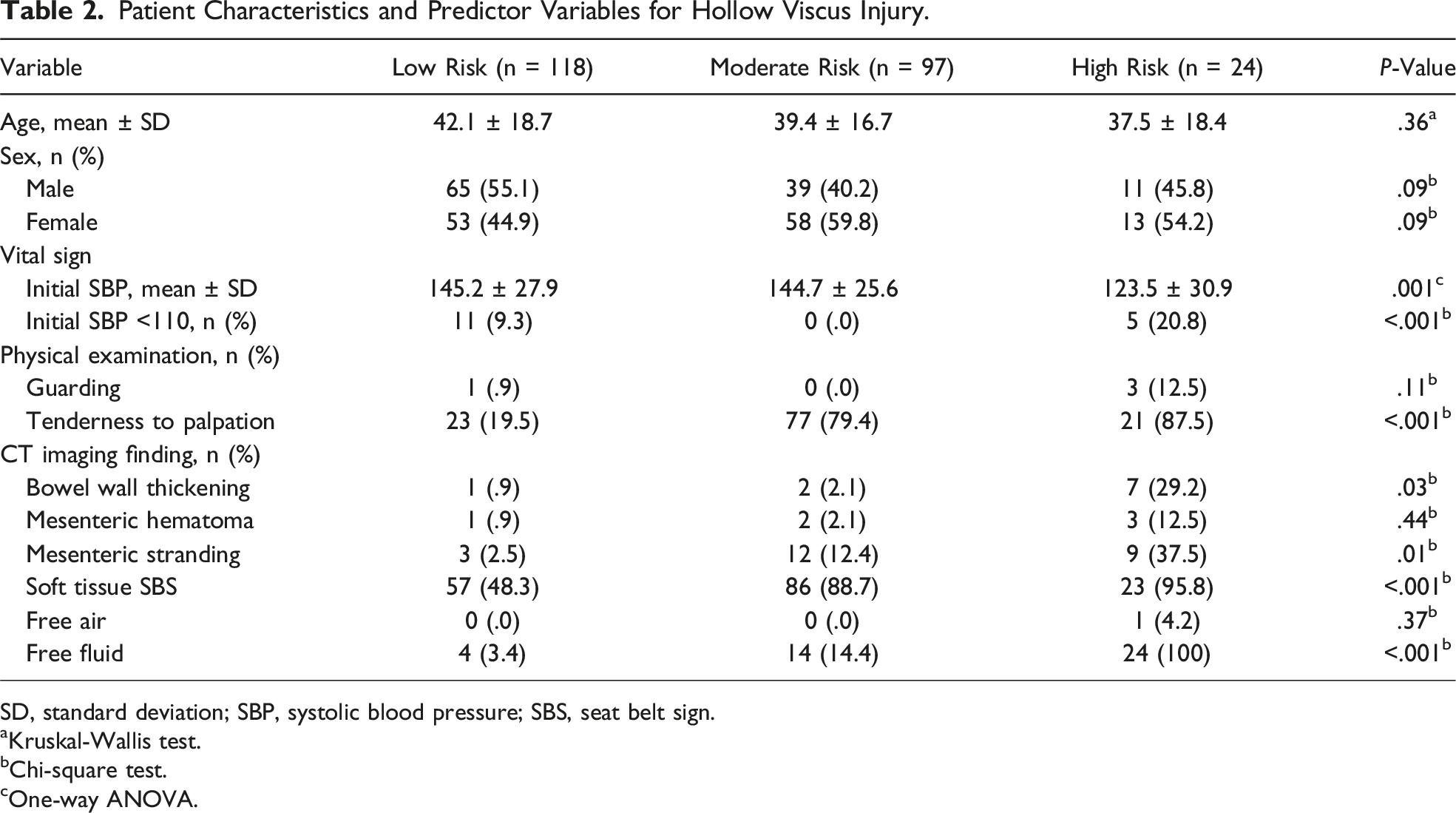
SD, standard deviation; SBP, systolic blood pressure; SBS, seat belt sign.
aKruskal-Wallis test.
bChi-square test.
cOne-way ANOVA.
Overall, a total of 20 patients (8.4%) underwent an abdominal operation (laparoscopy/laparotomy), and 17 patients (7.1%) were found to have an intraoperative HVI. HVI incidence was 1.7% in the low-risk cohort, 3.1% in the moderate-risk cohort, and 50% in the high-risk cohort. The 3 patients that underwent operation but were not found to have an intraoperative HVI had evidence of solid organ injury, diaphragm injury, and mesenteric injury with uninjured bowel, respectively.
Change in Management and Incidence of Hollow Viscus Injury.
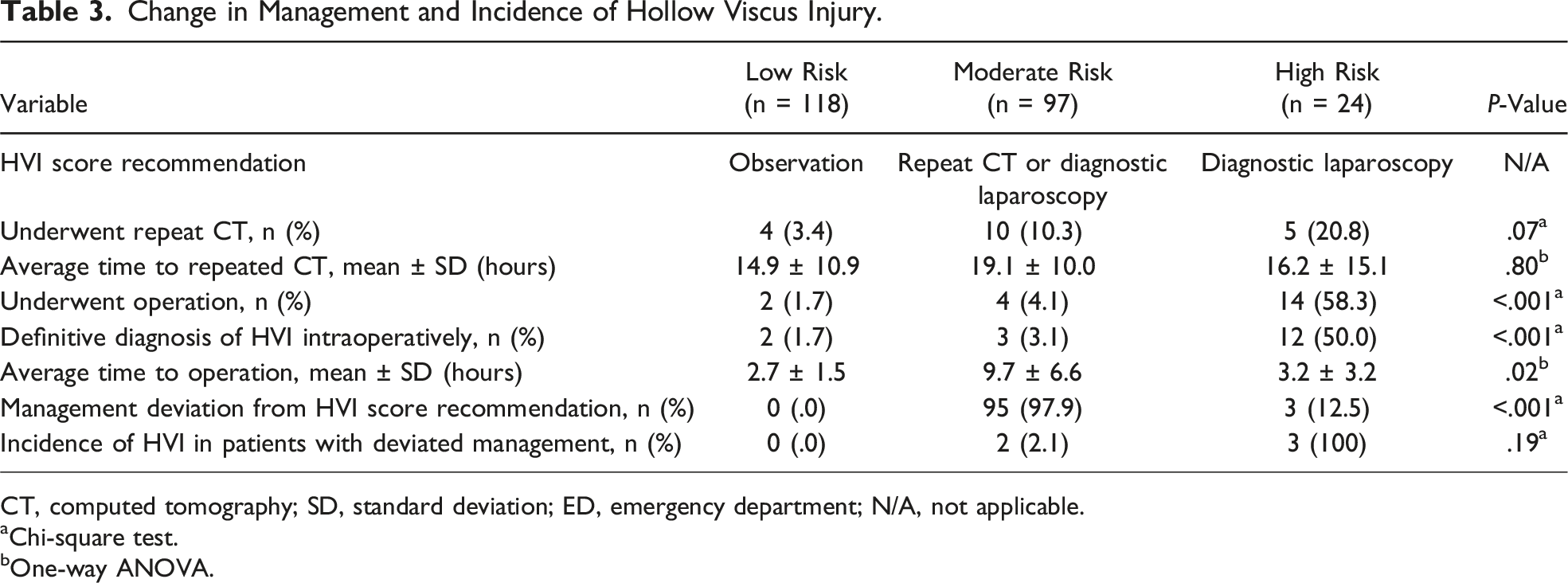
CT, computed tomography; SD, standard deviation; ED, emergency department; N/A, not applicable.
aChi-square test.
bOne-way ANOVA.
Negative Predictive Value and Positive Predictive Value for Low-Risk and High-Risk Cutoffs.
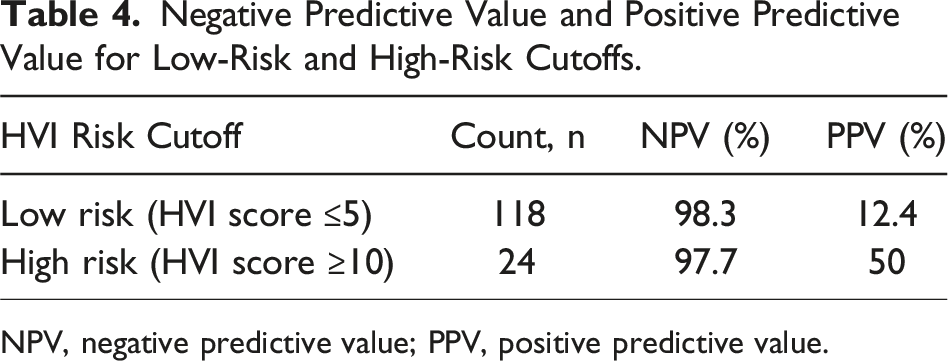
NPV, negative predictive value; PPV, positive predictive value.
Discussion
The detection and treatment of HVI remains an important yet challenging aspect in the management of blunt trauma patients with abdominal SBS. This clinical dilemma often complicates decision-making regarding the need for operative intervention. In this retrospective study of 239 trauma patients with abdominal SBS, the HVI score was applied to assess its predictive value and potential impact on clinical management. The HVI score demonstrated a high NPV at both the low-risk and high-risk cutoffs, while the PPV of 50% for the high-risk patients suggests its utility in identifying patients who may benefit from earlier intervention. Importantly, 5 patients from the moderate-risk and high-risk categories (2.1% of all patients) experienced delayed HVI diagnoses, all of whom would have likely benefited from earlier intervention guided by the HVI score.
Interestingly, this study demonstrated that 1.7% of low-risk patients suffered an HVI. On further analysis of these charts, it was found that these patients shared a common thread of having multiple CT findings in the setting of abdominal pain (eg, abdominal tenderness plus bowel wall thickening and mesenteric stranding). This led our group to make a modification to the HVI score, where patients with certain CT imaging findings (ie, bowel thickening or hypoenhancing bowel) or multiple findings such as free fluid and mesenteric contusion would undergo at least repeat laboratory and CT imaging. This suggested clinical algorithm for the management of HVI is outlined in Figure 1. While the use of repeat CT imaging has not been demonstrated to prevent missed HVI, in a study of 754 patients with abdominal SBS, Delaplain et al reported that the use of repeat CT imaging identified 15 additional patients requiring an operation, of which 8 of those were found to have an HVI.
7
The consequences of a missed HVI can lead to significant morbidity and an increased risk of mortality;8,9 thus, repeat CT imaging may offer additional guidance for management, including the decision to forego surgery. Suggested clinical algorithm for management of hollow viscus injury. SBS, seat belt sign; CT, computed tomography; ED, emergency department; Obs, observation; CBC, complete blood count; IV, intravenous; PO, per os; WBC, white blood cell count.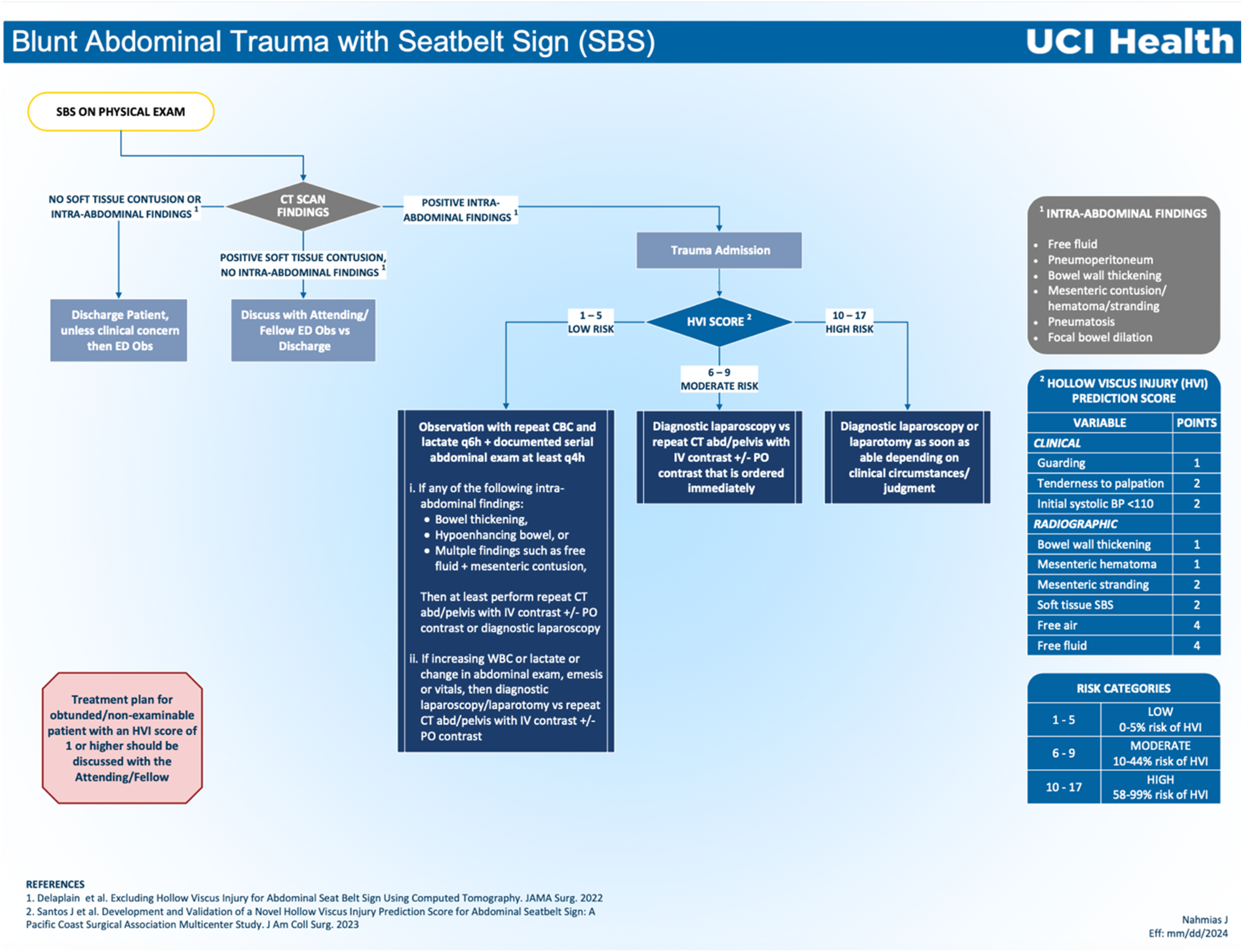
Due to the non-specific clinical picture of traumatic HVIs early on, delays to operative management have occurred. A 2024 large database study found that the average latency between admission and the time of surgery for HVI cases is approximately 26 h. 11 Our study even demonstrated a mean time to operation of over 9 h for moderate-risk patients, which is alarming considering previous studies have demonstrated that even a 6-h delay is independently related to increased mortality.9,12 This lethal delay in management further supports the creation of a reliable risk scoring tool to expedite diagnosis and potentially inform clinical practice. In our study, 5 patients had delayed surgical intervention, although only 3 (60%) of these patients had a definitive diagnosis of HVI compared to the 93.3% of patients with earlier operation. Due to this small number of patients with delayed operation, we are unable to perform meaningful analyses to compare early vs delayed operations, but future prospective research is needed to ascertain how time to surgical management specifically affects clinical outcomes. Ultimately, our study showed that the high-risk cutoff value for the HVI score appears to help predict need for operation for high-risk patients in a timelier manner, as it would have helped 12.5% of the population in this cohort receive earlier management.
Various risk prediction tools already exist for trauma and have been evaluated to predict overall outcomes, including the Trauma and Injury Severity score (TRISS) and the National Surgical Quality Improvement Program (NSQIP) Risk Calculator, but none of these can reliably help with the prediction of HVI.13-15 While there have also been previous attempts to specifically predict HVI,16-18 these tools lack predictive ability and are not widely used due to their impractical application. The Bowel Injury Prediction Score (BIPS) is one such tool and consists of 3 predictors (admission CT Grade ≥4, WBC count ≥17,000, and abdominal tenderness) for blunt HVI, but its CT grading system is institution-specific and only includes the finding of mesenteric contusion/hematoma. 16 Thus, it lacks incorporation of other known secondary signs for HVI including bowel thickening and focal bowel dilation. 19 In addition, when prospectively validated, BIPS performed inferior to the HVI score (BIPS AUROC .75 vs HVI score AUROC .94).10,20 This is likely due to the fact that the HVI score has a more nuanced evaluation of CT findings and incorporates other factors including vitals and physical exam findings.
Our study has notable limitations including those inherent to its retrospective single-center design (ie, generalizability and power). Another limitation of this study is the fact that there is no standardized definition for an abdominal SBS, although this reflects real world clinical practice. Additionally, the application of the study findings and the proposed clinical algorithm may not be generalizable to intubated and/or non-examinable patients (ie, patients with severe traumatic brain injuries) as there was a paucity of these categories of patients in this current study. Finally, the overall low incidence of HVI should be noted.
In conclusion, this single-center study found that the use of the HVI score would lead to changes in management of blunt trauma patients with an abdominal SBS. This includes earlier detection and management in moderate-risk and high-risk patients for HVI. Future prospective multicenter research is needed to ascertain if widespread adoption of the HVI score leads to improved patient outcomes.
Supplemental Material
Supplemental Material - A Single-Center Evaluation of a Novel Hollow Viscus Injury Prediction Score for Abdominal Seatbelt Sign
Supplemental Material for A Single-Center Evaluation of a Novel Hollow Viscus Injury Prediction Score for Abdominal Seatbelt Sign by Elaha Noori, Alexander T. Lee, Jeffrey Santos, Areg Grigorian, Matthew O. Dolich, Sigrid K. Burruss, Catherine M. Kuza, and Jeffry Nahmias in Journal of the American Surgeon™.
Footnotes
Author Contributions
Conceptualization: Santos, Grigorian, Nahmias. Data curation: Noori, Lee, Santos, Grigorian, Dolich, Burruss, Kuza, Nahmias. Formal analysis: Noori, Lee, Santos. Methodology: Noori, Lee, Santos, Nahmias. Project administration: Noori, Lee, Santos, Nahmias. Writing – original draft: Noori, Lee. Writing – review and editing: Noori, Lee, Santos, Grigorian, Dolich, Burruss, Kuza, Nahmias. Supervision: Nahmias.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available on reasonable request from the corresponding author, EN. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.