
Abstract
Background
Blunt splenic injuries are common traumatic injuries. Severe injuries may require blood transfusion, procedural, or operative intervention. Conversely, patients with low-grade injuries and normal vital signs frequently do not require intervention. The level and duration of monitoring required to safely manage these patients are unclear. We hypothesize that low-grade splenic trauma has a low rate of intervention and may not require acute hospitalization.
Methods
This retrospective descriptive analysis included patients admitted to a level I trauma center with low injury burden (injury severity score <15) and The American Association for the Surgery of Trauma (AAST) grade 1 (G1) and 2 (G2) splenic injuries between January 2017 and December 2019 using the Trauma Registry of the American College of Surgeons (TRACS). The primary outcome was the need for any intervention. Secondary outcomes included time to intervention and length of stay.
Results
107 patients met inclusion criteria. 87.9% required no intervention . 9.4% required blood products, with a median time to transfusion of 7.4 hours from arrival. All patients receiving blood products had extenuating circumstances such as bleeding from other injuries, anticoagulant use, or medical comorbidities. 2 patients required splenic artery embolization, one presenting with return precautions 9 days post-injury and 1 with significant comorbidities. One patient with concomitant bowel injury required splenectomy.
Conclusions
Low-grade blunt splenic trauma has a low rate of intervention, which typically occurs within the first 12 hours of presentation. This suggests that outpatient management with return precautions may be appropriate for select patients after a short interval of observation.
Key Takeaways
• Low-grade, blunt splenic trauma in patients with low injury burden (ISS <15) has a low rate of intervention. • The median time to intervention is short for low-grade splenic injuries, and those requiring intervention typically have extenuating circumstances. • Due to the low rate and short time to intervention, outpatient management with return precautions for select patients after a period of observation may be appropriate.
Introduction
Splenic injuries are among the most common abdominal injuries from blunt trauma. While patients with severe blunt organ injury and hemodynamic instability often require blood transfusion, splenectomy, or other intervention to stop bleeding, patients whose imaging studies show isolated, low-grade, blunt solid organ injuries with normal vital signs frequently do not require intervention. The Eastern Association for the Surgery of Trauma (EAST) practice management guidelines recommend the nonoperative management (NOM) of patients with blunt splenic injuries who are hemodynamically stable and without peritonitis, 1 and many additional studies support these findings, describing the feasibility of NOM in adult2-5 and pediatric patients.6,7
These patients are often observed with serial abdominal examination, hemodynamic monitoring, and laboratory studies to evaluate for ongoing hemorrhage or other complication following the injury that would require intervention. Delayed hemorrhage, especially in the outpatient setting, is a feared complication of NOM of blunt splenic injury (BSI). However, the literature demonstrates a low failure rate of nonoperative management of splenic injuries, particularly those which are low grade.4,5,8,9 While NOM has been established as the standard management for blunt, low-grade splenic injuries, 1 there is little quality data or consensus on the optimal duration or intensity of clinical observation following blunt solid organ injuries.
Given the insufficient data to support whether these patients can be safely managed in an outpatient setting, we aim to address these gaps in knowledge with a retrospective study of patients with low-grade splenic injury. We hypothesize that non-severe, low-grade splenic trauma has a low time to intervention and does not require acute hospitalization.
Methods
This study was approved by the institutional review board. We conducted a retrospective descriptive analysis of patients with low-grade BSI at a level I trauma center between January 1st, 2017 and December 31st, 2019. Patients were identified from the Trauma Registry of the American College of Surgeons (TRACS) database. Clinical data were obtained from the electronic health record.
Patients were included if they had American Association for the Surgery of Trauma (AAST) grade I (G1) and II (G2) splenic injuries,
10
injury severity score (ISS) less than 15, and blunt mechanism of injury. Previous literature has identified ISS less than 15 as the cutoff between major and minor traumas.
11
Patients who were pregnant, incarcerated, experienced penetrating trauma, died in the emergency department (ED), or who did not have radiographic documentation of splenic injury were excluded from the study (Figure 1). Inclusion and exclusion criteria.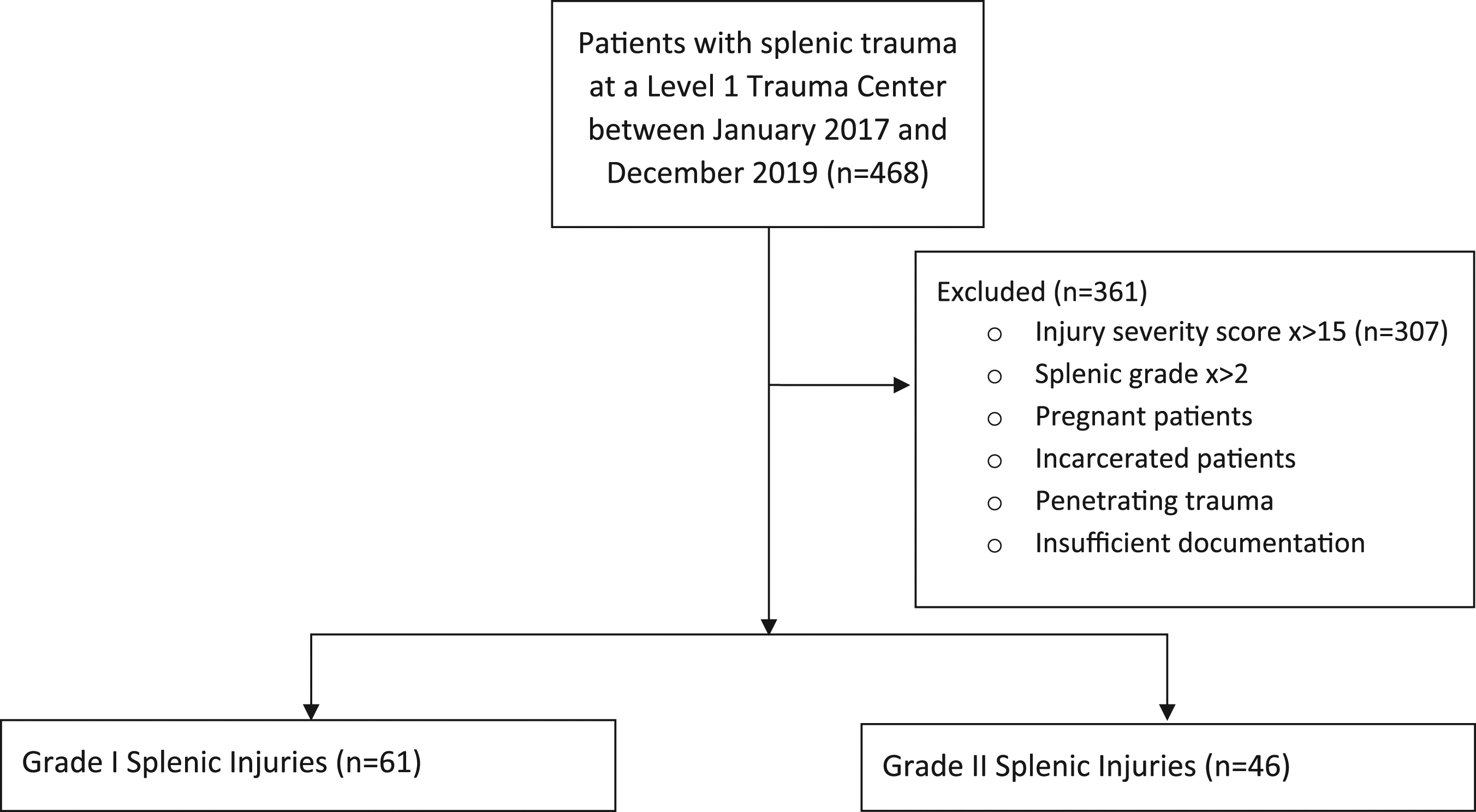
Demographic Data.
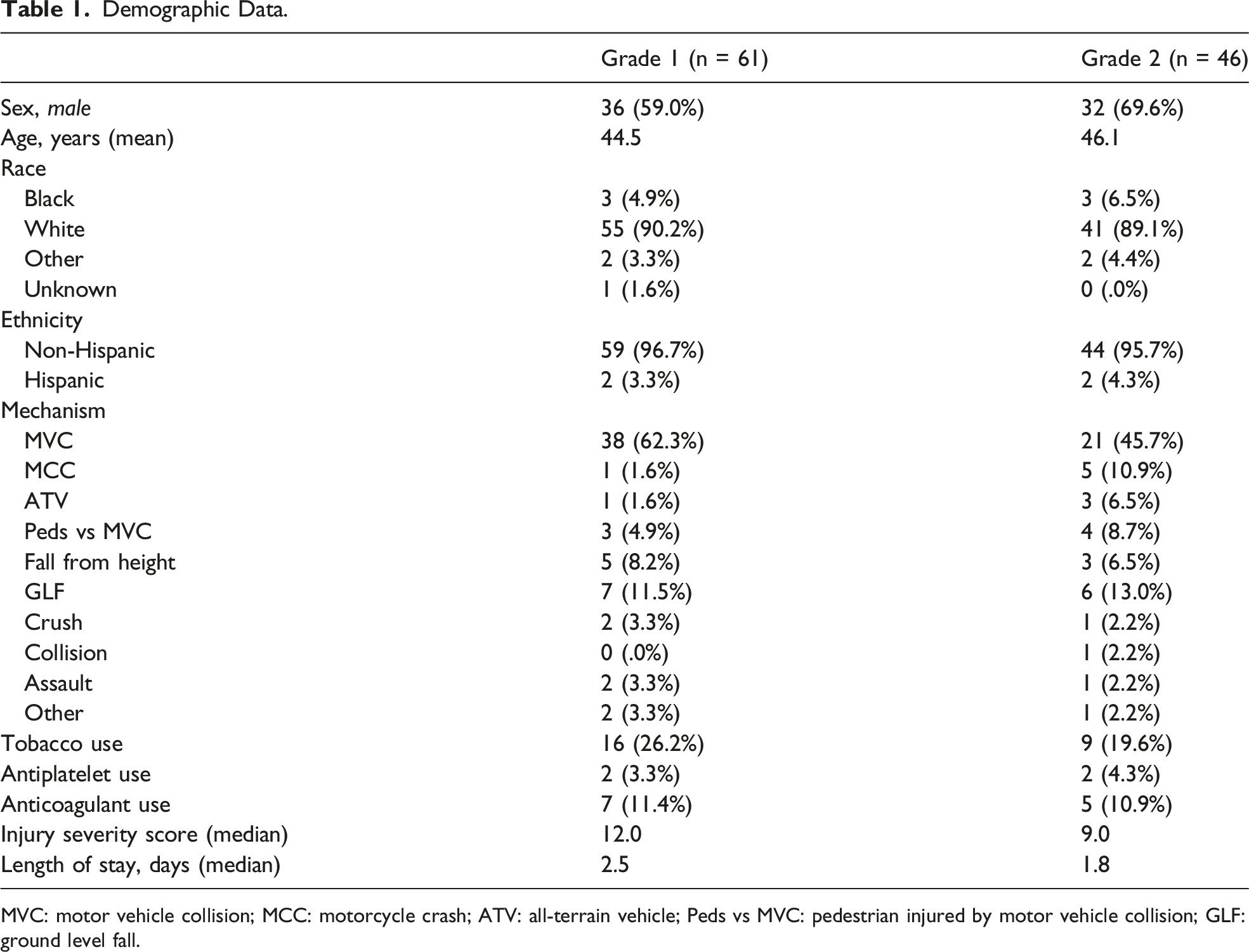
MVC: motor vehicle collision; MCC: motorcycle crash; ATV: all-terrain vehicle; Peds vs MVC: pedestrian injured by motor vehicle collision; GLF: ground level fall.
American Association for the Surgery of Trauma grading of the splenic injury was determined based on the radiologist’s interpretation of the patient’s imaging. If a grade was not provided, a senior trauma surgeon graded the splenic injury. Patients who had outside imaging with no documentation of grade of injury or measurements of the injury were excluded due to insufficient data.
The primary outcome of intervention was defined as the need for blood products, including the type and volume of blood products administered, splenic artery embolization, or splenectomy. Secondary outcomes included length of stay, which was calculated from ED arrival time to discharge time, and time to intervention, which was defined as ED arrival time to time of first blood product, embolization, or operation.
Results
Interventions Required for Low-Grade Splenic Injuries.
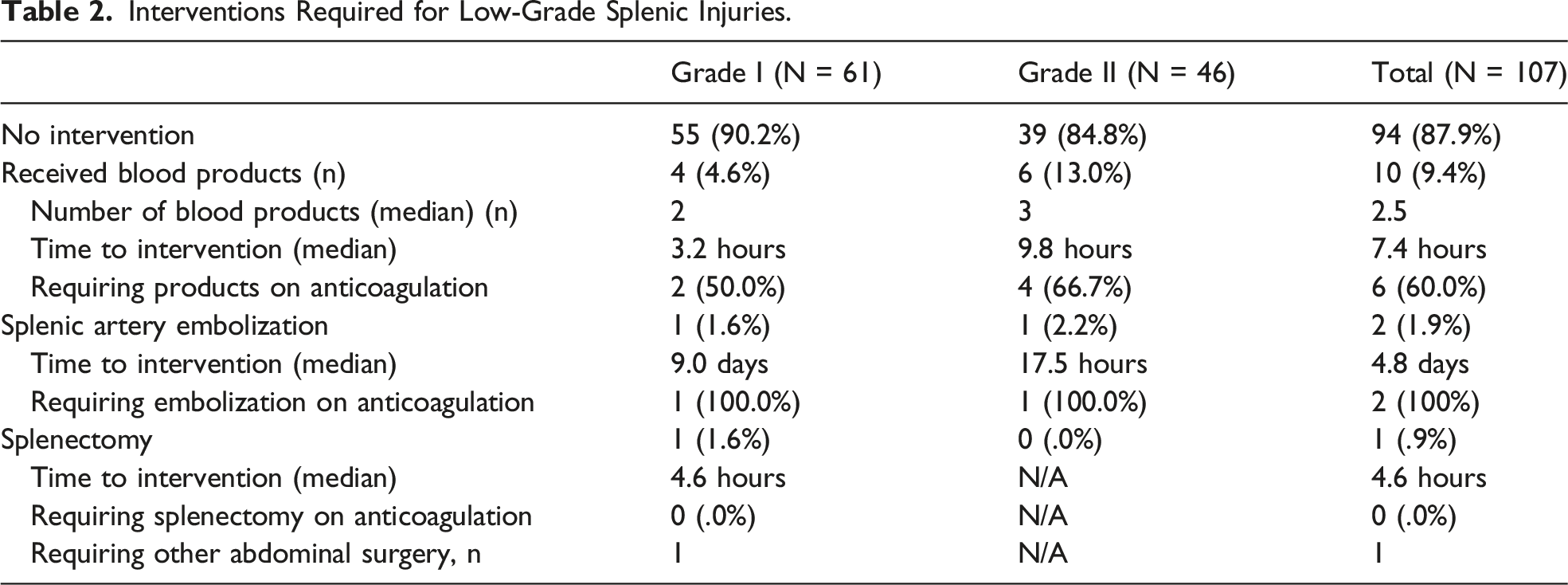
4 (4.6%) G1 patients required a median of 2 blood products while 6 (13.04%) G2 patients required a median of 3.0 units of blood products. Median times to transfusion for G1 and G2 injuries were 3.2 and 9.9 hours, respectively. Of the 10 patients who received blood products, 4 (40.0%) had significant bleeding from other injuries, 4 (40.0%) received plasma only for warfarin reversal, and the remaining 2 (20.0%) had significant medical comorbidities. The time to transfusion was lower in patients who were not on anticoagulation, with a median time to transfusion of 4.0 hours overall (n = 4), in comparison to 7.4 hours with the 2 groups combined (n = 10).
One patient from each group, G1 and G2, required splenic artery embolization with median time to intervention of 9.0 days and 17.5 hours, respectively. Both patients requiring embolization were on an anticoagulant. The patient with G1 injury who underwent splenic artery embolization was discharged in stable condition 2 days post-injury with return precautions. The patient represented 9 days post-injury with new abdominal pain and underwent embolization at that time. The patient with G2 injury requiring embolization presented with a concurrent NSTEMI, hemoperitoneum, but no active extravasation on imaging. One patient with G1 injury had a concomitant hollow viscous injury as the primary surgical indication before also undergoing splenectomy.
Discussion
Blunt splenic trauma is a common frequent diagnosis with a robust body of the literature supporting nonoperative management of such injuries. Our data exemplify that splenic trauma has a low rate of intervention, with only 12.1% of all patients needing any intervention. It is important to note the natural history of splenic injuries. While is it well documented that patients fail nonoperative management at low rates,4,5,8,9 patients may experience the formation or bleeding of a pseudoaneurysm or delayed splenic rupture, illustrating the importance of return precautions in the safety of outpatient management. Notably, only 1 patient in our cohort returned with a complication 9 days post-injury with new abdominal pain. This illustrates both the low rate of complications and the importance of return precautions in these patients. Patients with new or worsening abdominal pain, signs of hypotension like dizziness or syncope, and new or worsening fatigue should have a low threshold to return to care.
Our study has several limitations. This study is retrospective and relies on what is documented in the electronic health record. Tangibly, 26 patients were excluded from the study due to a lack of documentation of splenic grade if the original radiographs were unobtainable. Further, many patients in our data pull had splenic grades higher than grade II, suggesting that we may have alternatively not have captured all the grade I and grade II injuries during this time frame.
Given this restricted availability of data, our sample size is small, and we recognize this as a limitation of this study. Despite this, we posit that the data from this descriptive study are generalizable given that we used measurements common among most trauma centers such as ISS and AAST grading scales.
We defined time to intervention as ED arrival time to time of first blood product or procedure and not the time of injury to time of intervention. We recognize that time of initial injury to intervention time would be a helpful data point as patients with varied geographical distances from our center have different transport times and this may impact the time to intervention once patients reach the hospital. Unfortunately, this information is often unavailable and/or unreliable.
Ultimately, our data illustrate that low-grade blunt splenic trauma has a low rate of intervention, with any intervention typically within the first 12 hours of presentation. Patients with an ISS <15, an AAST splenic grade of I or II, and who do not have significant concomitant medical ailments, such as an NSTEMI, may be appropriate for discharge with return precautions after a short period of observation. Our study bolsters the existing data supporting NOM as feasible in blunt splenic trauma and while adding an important glance into the time to intervention for these injuries. Preventing unnecessary hospitalization, transfers to tertiary care centers, and undue hospital bills can positively impact the hospital system, decrease cost, and keep hospital bed capacity available for patients needing life-saving intervention. To achieve this, additional work in this field is necessary. Studies to further this research may include performing a multicenter retrospective study to determine if results remain consistent across health systems. Additional research to identify a prospective prediction model for necessary observation intervals and interventions may allow trauma surgeons to refine outpatient follow-up recommendations to have patients with low-grade, blunt splenic injuries to be safely discharged with return precautions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.