
Abstract
Introduction
Robotic pancreaticoduodenectomy (rPD) is a complex operation with a reported learning curve of 80 cases. Two recent graduates of a formal robotic complex general surgical oncology training program have been performing rPD at our institution since 2016, which had no previous institutional experience with rPD.
Objective
To evaluate the learning curve associated with developing a new robotic pancreaticoduodenectomy (rPD) program by fellowship trained surgeons with institutional support.
Methods
Sixty patients undergoing rPD from 2016 to 2022 were reviewed for and compared with proficiency benchmarks set by the University of Pittsburg experience.
Results
By 30 cases, operative time met the proficiency benchmark of 391 minutes. Additionally, the entire cohort had comparable rates of clinically relevant postoperative pancreatic fistula (6.7% vs 3%, P = .6), 30-day mortality (0% vs 3%, P = .18), major complications (Clavien >2; 23% vs 17%, P = .14), and length of stay (6 vs 7 days, P = .49) when compared to the benchmark.
Conclusion
Perioperative outcomes were comparable to proficiency benchmarks from initiation of the new rPD program, and operative time reached proficiency benchmark by 30 cases. This data suggests that graduates of formal rPD training programs can safely establish new minimally invasive pancreas programs at sites with no previous institutional rPD experience.
Keywords
Introduction
Since being first described in 2003, adoption of the robotic pancreaticoduodenectomy (rPD) is increasing worldwide.1-3 Retrospective analyses have shown that perioperative outcomes of rPD are noninferior to open PD, and some studies even suggest a benefit in select populations when specifically comparing operations performed by surgeons past the learning curve of rPD.4-7 Thus, it is important to understand the learning curve of rPD to fully characterize the potential benefits of this approach.
Previous work performed at a single institution has defined the learning curves of rPD for 3 “generations” of rPD surgeons.8,9 The first generation, defined as early adopters of rPD with no mentorship or formal curriculum, had a learning curve of 80 cases. The second generation, defined as those with mentorship but no curriculum, had a greatly reduced learning curve of ∼20 cases. Finally, the third generation, fellows that underwent formal curriculum and mentorship, had too few cases to define a true curve, but was projected to be approximately 10-20 cases. The generalizability of this model is limited due to several reasons: (1) the first and second generation surgeons were already highly experienced in open PD, (2) the first generation model included “self-training” cases as the optimal rPD approach and setup were still being developed, and (3) second and third generations had the support of available experienced mentors and institutional familiarity with rPD. The more pertinent learning curve of developing a new rPD program by newly fellowship trained surgeons, in which graduates must overcome institutional-level factors as well as surgeon-specific factors, remain unknown.
Two recent graduates of a formal robotic training program have been performing rPD at our institution since 2016, which had no previous institutional experience with rPD. We report our experience with our first 60 consecutive cases and evaluate the learning curves associated with establishing a new rPD program by formally trained surgeons.
Methods
Patients
Sixty consecutive patients that underwent rPD at our institution from March 2016 to August 2022 were included in the study and retrospectively reviewed for clinicopathologic characteristics and perioperative outcomes. To analyze change in variables through time, the first 30 patients were compared to the second 30.
Institution
Prior to implementation of the rPD program, the institution already had in place Da Vinci Si systems with trained ancillary staff proficient in standard robotic surgery. During the study period, the institution added additional Da Vinci Xi systems which were used for rPD. Additionally, the institution was already a high-volume (>100 cases/year) PD center accustomed to PD postoperative care and with experienced open PD surgeons available.
Surgeons
All surgeries were performed jointly by M.D.G. and J.C.K. Both surgeons underwent formal robotics curriculum as described previously.9,10
Proficiency Benchmarks
Proficiency benchmarks for rPD were determined by the University of Pittsburgh experience as recently described in their last 100 of 500 rPD operations. 3 Operative time of 391 minutes, length of stay (LOS) of 7 days, and rates of major complications (Clavien >2) at 17%, 30-day mortality at 3%, and clinically relevant postoperative pancreatic fistula (CR-POPF) at 3% were considered as proficient in the study. Outcomes at our institution were compared to these proficiency benchmarks.
Statistical Analysis
Summary statistics were obtained using established methods. Categorical variables were compared using χ2 test. Continuous variables were compared using the Mann-Whitney U test. LOESS modeling was used for operative time learning curves. All tests were two-tailed and P-value of less than .05 was considered significant. Analysis was conducted in R (version 4.2.2).
Results
Patient Demographics
Cohort Demographics.
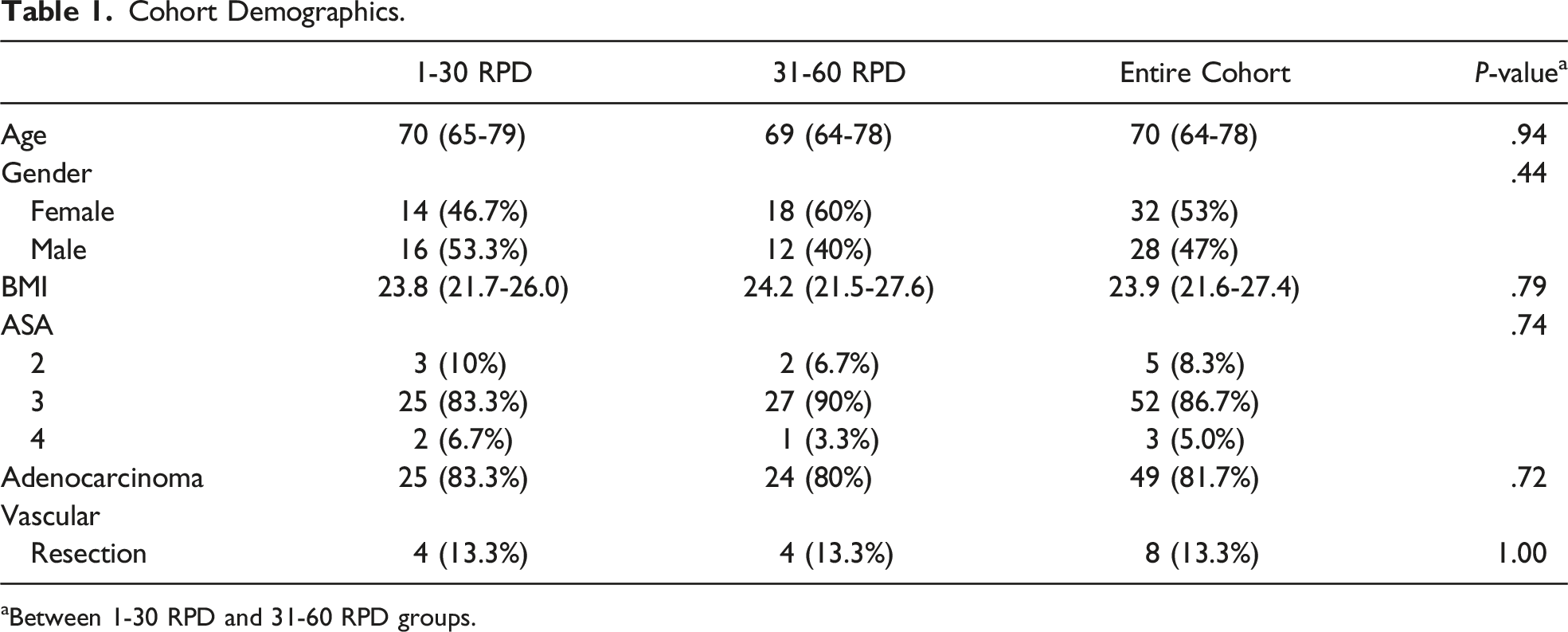
aBetween 1-30 RPD and 31-60 RPD groups.
Optimization of Perioperative Outcomes
Perioperative Outcomes.
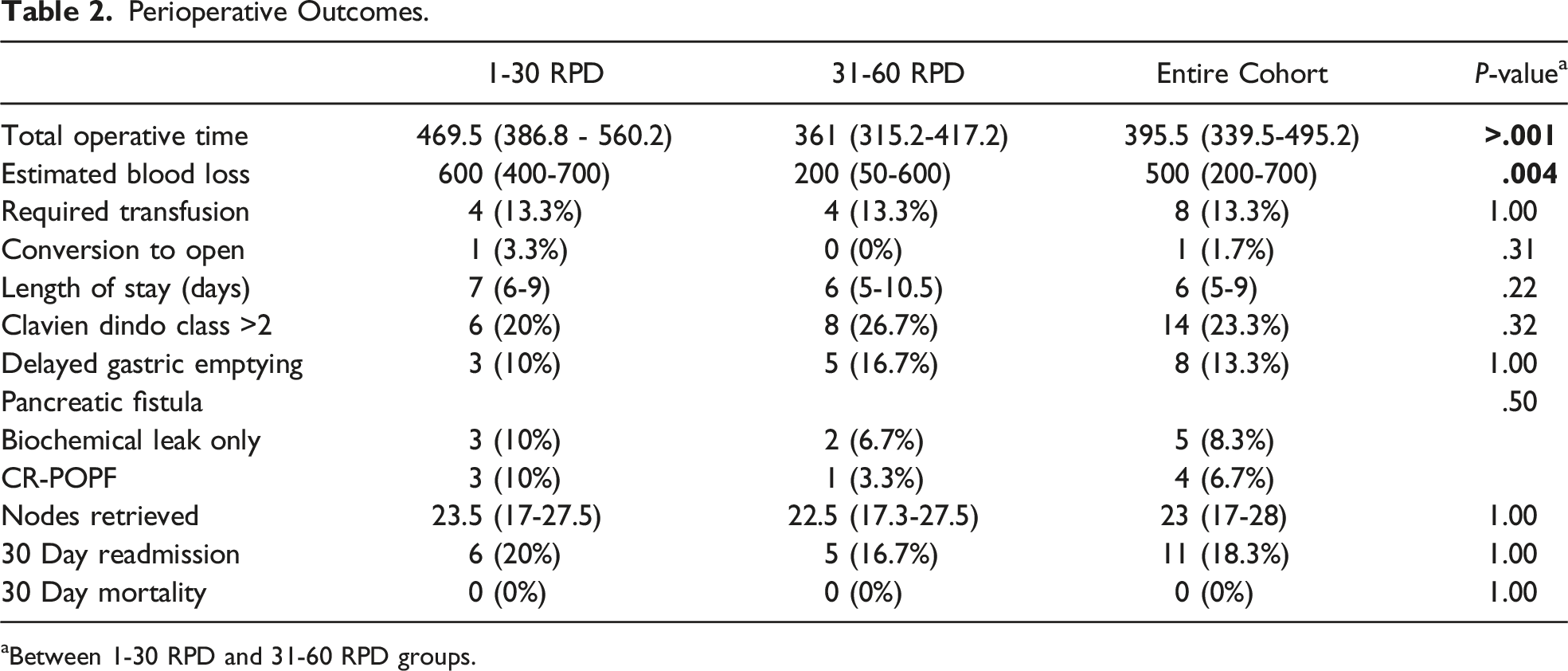
aBetween 1-30 RPD and 31-60 RPD groups.
Comparison to Proficiency Benchmarks
By 30 cases, operative time was comparable to the proficiency benchmark of 391 minutes and continued to improve until 40 cases where operative time plateaued at 332 minutes (Figure 1). Since the other benchmarks did not improve over time, the outcomes of the entire cohort were compared with the proficiency benchmarks. Rates of CR-POPF (6.7% vs 3%), conversion to open (1.7% vs 5%), major complications (Clavien >2; 23% vs 17%), and length of stay (6 vs 7 days) were all comparable between this cohort vs benchmarks (Table 3). Operative time by case number. Benchmark Comparisons of Perioperative Outcomes.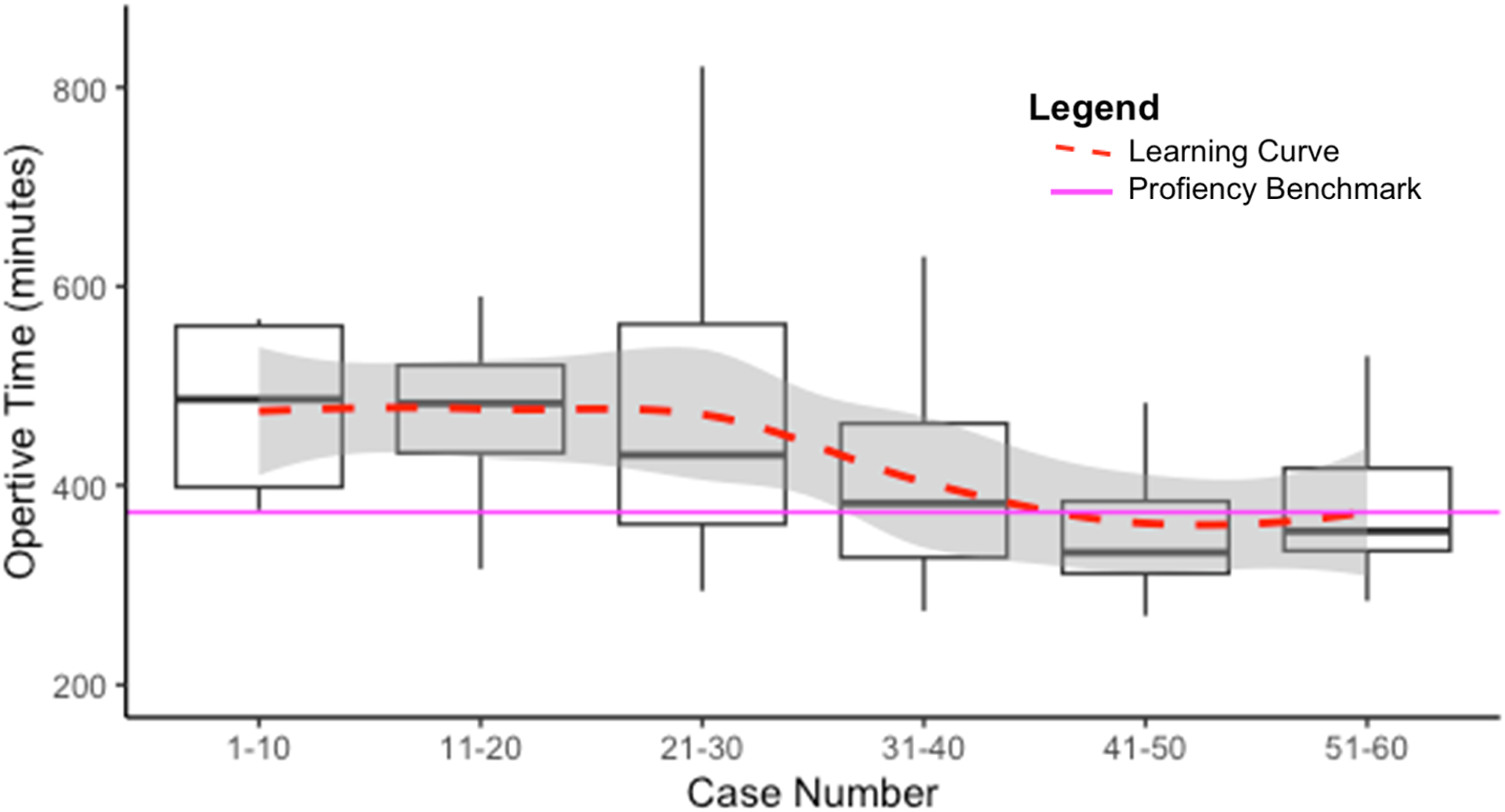

Discussion
This work represents the first to analyze the learning curve of establishing a new rPD program by formally trained robotic surgical oncologists. Our data demonstrates that technical proficiency, as measured by operative time, was comparable to benchmark standards by the 30th case at our institution. Importantly, perioperative safety outcomes of LOS and rates of CR-POPF, 30-day mortality, and major complications (Clavien >2) did not change over time and were comparable to proficiency benchmarks from the initiation of the rPD program.
The development and safety of a formal robotic training curriculum have been well described; however, the performance of these surgeons in independent practice following training is not known. 9 A standard framework defines the 3 phases of a surgical learning curve as follows: (1) A rapid ascent to independent competence to an acceptable standard from commencement of training, (2) Small incremental gains until a plateau of mastery is reached, and (3) A fall in performance due to multifactorial causes including age, dexterity, and cognition. 11 Our findings confirm that the robotic training curriculum as previously described adequately propels graduates through the first phase of the learning curve to establish new rPD programs without compromising patient safety or outcomes, even at institutions without prior rPD experience. Additionally, while there are many factors to consider in mastery, when measured by strictly operative time alone, a plateau was reached soon after at 30 cases.
Beyond perioperative outcomes and operative time, there are several other factors to consider in technical adequacy of PD. Unplanned conversion to open is an important metric in minimally invasive pancreatectomy as it has been associated with worse overall outcomes. 12 Despite this cohort’s case complexity as measured by vascular resection rates mimicking national averages and the case series establishing the proficiency benchmarks, rates of unplanned conversion remained low throughout the study. Notably, contrary to prior observation, adoption of the Da Vinci Xi system did not affect our rate of conversion to open. 3 Additionally, number of lymph nodes harvested is an important surrogate of optimal oncologic resection with the International Study Group on Pancreatic Surgery recommending a minimum of 15 nodes for adequate pathologic staging of disease, which was well exceeded throughout the study. 13
Previous literature assessing rPD learning curves have had important limitations that hinder their generalizability. The initially described 80-case threshold included a pioneering discovery phase in which the surgeons had to develop optimal surgical technique and institutional procedures for rPD. 8 Subsequent follow-up studies performed at the same institution, which reduced the learning curve to 10-40 cases, had the unique advantage of institutional familiarity with rPD including trained operative staff, appropriate equipment, and, most importantly, mentorship of proficient rPD surgeons.3,9 Other reported studies of adopting rPD in different institutions were all of surgeons already experienced in open PD.1,2 To our knowledge, this is the first study to look at the outcomes of a new rPD program by recent graduates of a formal robotic curriculum.
This study has several limitations. Although all patients evaluated by the operative surgeons in this study were offered rPD without any exclusion criteria, the retrospective and unblinded nature of this study has inherent selection biases. Additionally, though our institution had no previous experience with rPD, it was experienced in open PD and had trained ancillary staff proficient in standard robotic surgery, therefore our findings may not be applicable to low volume centers. We also did not control for trainee involvement which could influence operative time and perioperative outcomes. Finally, we did not consider long-term outcomes following rPD in this study.
In conclusion, our findings suggest that graduates of formal rPD training programs can safely establish new minimally invasive pancreas programs at sites without previous rPD experience. These results have important implications in the dissemination of this new approach to PD in a world where outcomes are appropriately under increasing scrutiny.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.