
Abstract
Background
Complex, minimally invasive hepatopancreatobiliary surgery (MIS HPB) is safe at high-volume centers, yet outcomes during early implementation are unknown. We describe our experience during period of rapid growth in an MIS HPB program at a large regional health system.
Methods
During an increase in MIS HPB (60% greater from preceding year), hospital records of patients who underwent HPB surgery between 1/1/2019 and 12/31/2020 were reviewed. Operative time, estimated blood loss (EBL), conversion rates, length of stay (LOS), and perioperative outcomes were assessed.
Results
267 patients’ cases were reviewed. The population was 62 ± 13 years, 50% female, 90% white. MIS was more frequently performed for hepatic than pancreatic resections (59% vs 21%, P < .001). Open cases were more frequently performed for invasive malignancy in both pancreatic (70% vs 40%, P < .018) and hepatic (87% vs 70%, P = .046) resections. There was no difference in operative time between MIS and open surgery (293[218-355]min vs 296[199-399]min, P = .893). When compared to open, there was a shorter LOS (4[2-6]d vs 7[6-10]d, P < .001) and lower readmission rate (21% vs 37%, P = .005) following MIS. Estimated blood loss was lower in MIS liver resections, particularly when performed for benign disease (200[63-500]mL vs 600[200-1200]mL, P = .041). Overall 30-day mortality was similar between MIS and open surgery (1.0% vs 1.8%, P = 1.000).
Discussion
During a surgical expansion phase within our regional health system, MIS HPB offered improved perioperative outcomes when compared to open surgery. These data support the safety of implementation even during intervals of rapid programmatic growth.
Key Takeaways
• Minimally invasive hepatopancreatobiliary surgery (MIS HPB) is safe during the growth phase of implementation and show similar outcomes to those previously published. • MIS HPB has comparable, if not improved, perioperative outcomes compared to open approaches at experienced HPB centers. • Further studies are needed to elicit the full impact of an MIS HPB practice on patient outcomes.
Introduction
Minimally invasive surgery (MIS) is increasingly utilized as a standard of care for numerous conditions.1-3 For many procedures, MIS has been shown to reduce postoperative pain, decrease blood loss, have fewer complications, and shorten hospital stay.4-6 Initially, MIS was used exclusively for benign conditions due to concerns regarding perioperative risk and oncologic adequacy. Nonetheless, an extensive body of literature now supports the validity of MIS approaches in a number of malignancies.4,6-8 However, due of the degree of technical skill required for safe hepatopancreatobiliary (HPB) surgery, the adoption of MIS techniques has lagged behind those for other organ sites.9,10
Thus, the role of MIS in HPB is still evolving, even in large referral centers. The MIS HPB is becoming more frequently utilized as studies continue to demonstrate comparable complication rates and improved intraoperative metrics.11-15 This is especially true in large referral centers with surgeons experienced in complex HPB surgery. There is evidence to support that high-volume HPB centers are associated with improved clinical outcomes due to experience gained from a hospital systems standpoint, as well as surgeon-specific experience. 9 With increased use of the robotic platform, there has been a resulting increase in the complexity of cases treated using MIS techniques.16,17 While previous studies have compared the outcomes of MIS to the outcomes of open approaches for HPB cases at these large referral centers, there is a scarcity of data describing perioperative outcomes during MIS adoption and growth.12,14,18-21
As MIS techniques are becoming the standard of care for more pathologies and more complex MIS HPB surgeries are being performed, an evaluation of the safety during increased implementation is necessary. We assess the safety of MIS HPB during the growth phase of a program in our large regional health network.
Methods
Demographics of Patients That Underwent Hepatopancreaticobiliary Surgery, Procedures Performed, Minimally Invasive Surgery (MIS) vs Open Cases (n = 267).
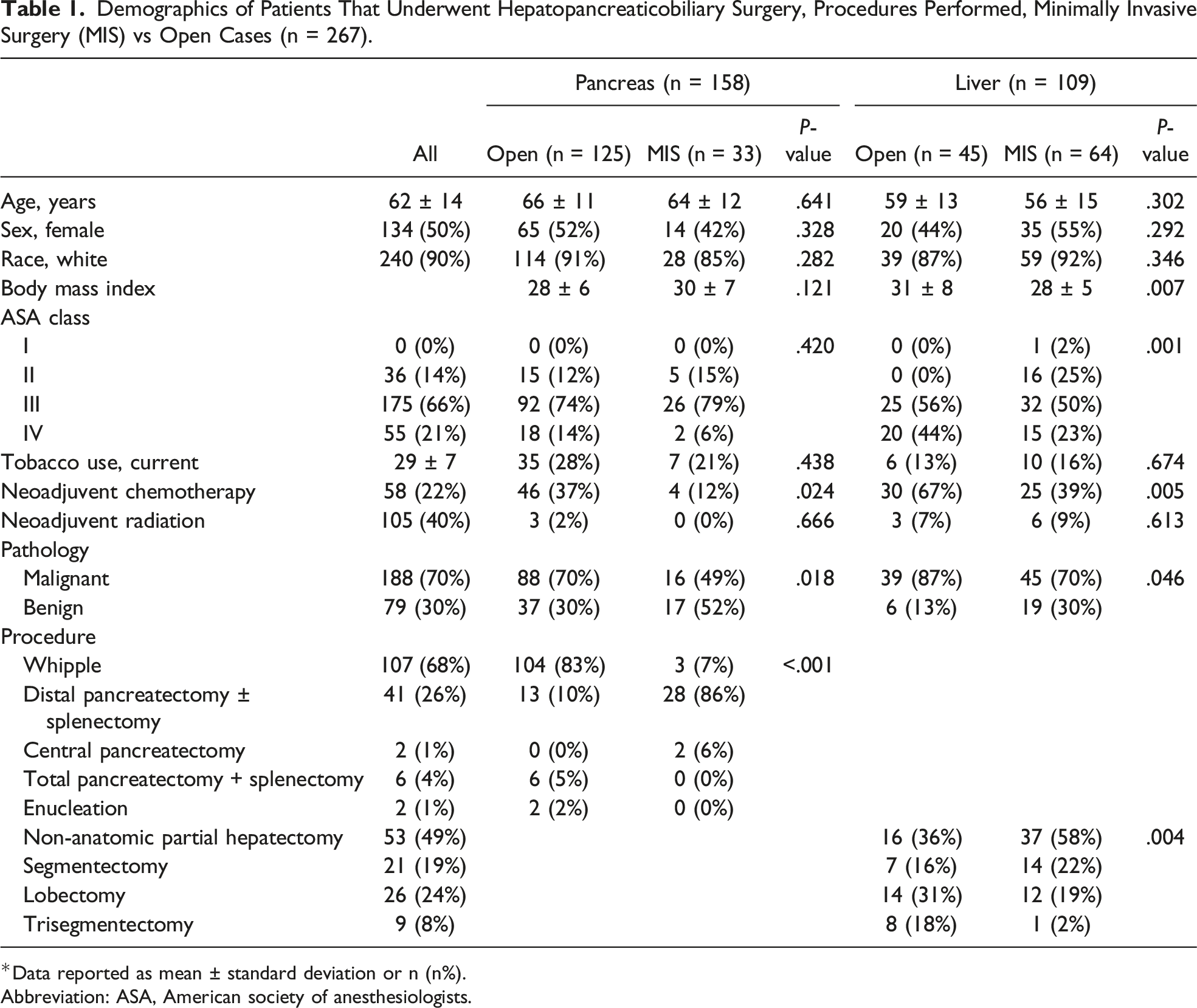
*Data reported as mean ± standard deviation or n (n%).
Abbreviation: ASA, American society of anesthesiologists.
Statistical Analysis
Data are reported as mean ± standard deviation if normally distributed, or median (interquartile range) if not. To test univariate associations, differences between treatment groups were compared using the Student t test for parametric data and the Mann-Whitney U test for nonparametric data. Categorical data were compared using Pearson chi-square; if cell counts were <5, the Fisher exact test was used. Statistical analyses were performed using SPSS version 28 (IBM Corporation; Armonk, NY).
Results
The full patient demographic breakdown is shown in Table 1. 267 patients’ cases were reviewed. Of the patients that underwent surgery, 97 (36%) underwent an MIS procedure, 15 (15%) laparoscopic and 82 (85%) robotic, and 170 (64%) underwent an open procedure. These patients were age 62 ± 13 years, 50% were male, and 90% were white. Of the entire cohort, 188 (70%) patients underwent resection for malignancy, and the remaining 79 (30%) were for benign indications.
Of the resections performed, 61 (32%) of malignant resections and 36 (46%) of benign diseases were performed via MIS, respectively. A breakdown of cases is shown in Table 1. MIS was more frequently performed for hepatic than pancreatic resections (59% vs 21%, P < .001). Of patients that underwent MIS, 64 (66%) underwent hepatectomy, 61 (63%) had invasive malignancy, 29 (30%) underwent neoadjuvant CT, 6 (6%) underwent neoadjuvant CRT, and 60 (62%) subsequently underwent an anatomical resection. Laparoscopic patients underwent mostly distal pancreatectomy and splenectomies (11, 73%), but also included central pancreatectomies (2, 13%), liver wedge resections (1, 6.7%), and segmentectomies (6.7%). Robotic patients underwent a wider variety of cases including whipples (3, 3.7%), distal pancreatectomies with or without splenectomy (17, 21%), and a full range of liver resections including wedge resections (36, 44%), segmentectomy (13, 15.9%), lobectomy (12, 12.6%), and trisegmentectomy (1, 1.2%). Of patients that underwent open surgery, 125 (74%) underwent pancreatectomy, 127 (75%) had invasive malignancy, 76 (45%) received neoadjuvant CT, 6 (4%) neoadjuvant CRT, and 152 (89%) underwent an anatomical resection. When compared to MIS, open cases were most frequently performed for invasive malignancies in both pancreatic (70% vs 40%, P < .018) and hepatic (87% vs 70%, P = .046) resections.
Intraoperative and Post-Operative Outcomes by Organ (n = 267).
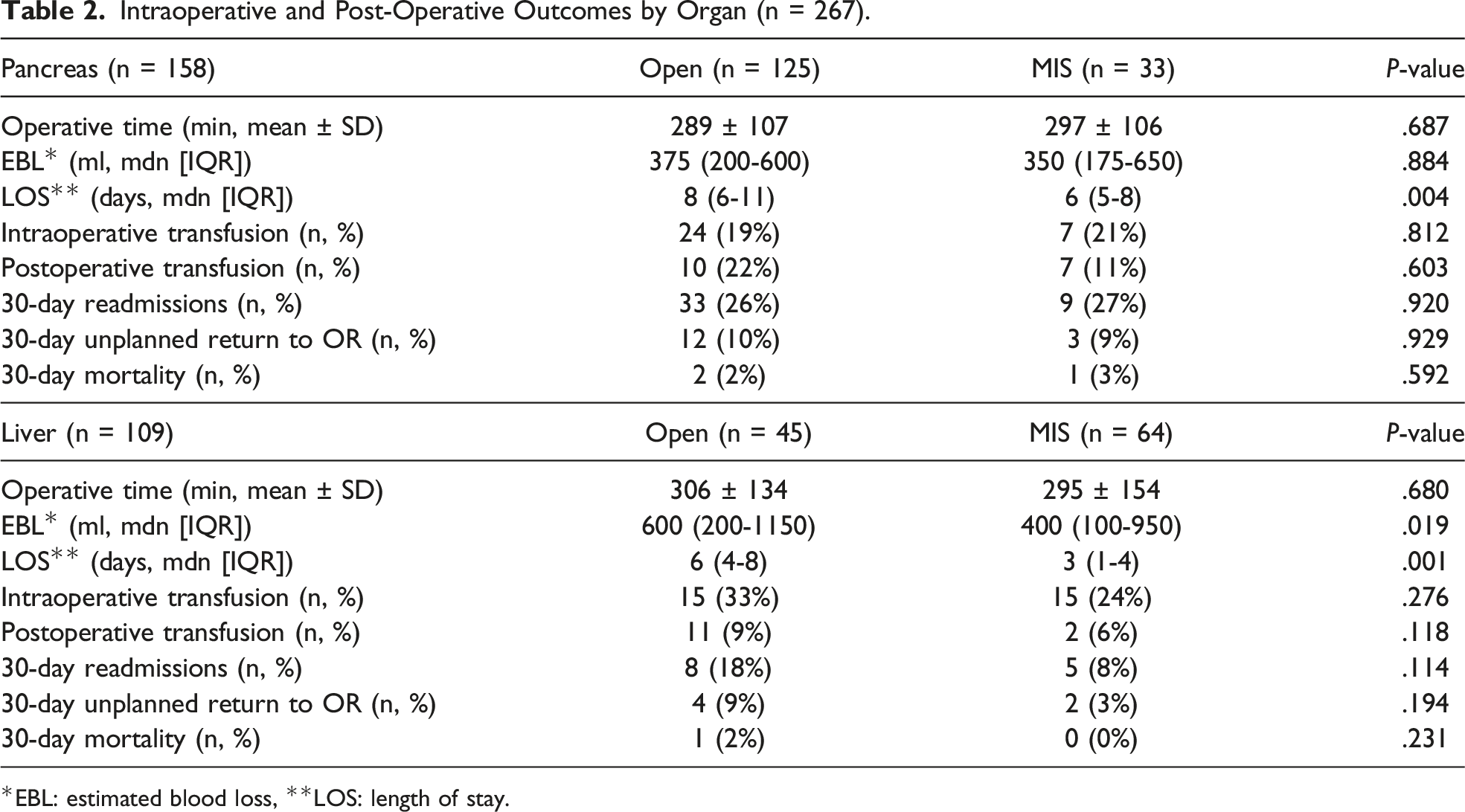
*EBL: estimated blood loss, **LOS: length of stay.
Discussion
With comparable perioperative outcomes, our analysis demonstrates safety during a phase of increased implementation of MIS HPB within a large regional health network.
The complexity of HPB surgeries has made surgeons cautious about adopting MIS approaches for these HPB cases. With increased coalescence of HPB surgery to high-volume centers and the increased use of the robotic platform, the adoption of MIS for HPB pathology has been proven to be safe. Overall, our center had a comparable performance to those previously studied. An important factor in evaluating expertise in MIS is conversion rate. Our conversion rate for pancreatic cases was 30%; other high-volume centers have reported conversion rates from 10-30% for laparoscopic cases and 0-10% for robotic cases.22-27 The conversion rate for hepatic cases was 25%, exclusively occurring during oncologic resections. This rate is higher than other studies, which have reported conversion rates of 0-12% for laparoscopic and 0-20% for robotic hepatic resections.28-34 It should be noted that several of the studies listed did not specify the indication for resection, only laparoscopic vs robotic, when comparing conversion rates. Conversion to open resection typically occurs due to uncontrolled hemorrhage, difficulty achieving adequate oncologic resection, or general lack of progress in performing the procedure. In our early implementation, it is likely that patient selection and surgeon comfortability with specific procedures, such as whipples and lobectomies or trisegmentectomies, contributed to an increased overall conversion rate compared to more experienced centers.
Other studies have reported a learning curve of approximately 60 cases for laparoscopic liver resections. 28 In our experience, we were able to demonstrate comparable complication rates and significantly shorter hospital stays for the 64 cases reviewed. These results are similar to those previously reported at other high-volume centers.18,28-30,32 Given the anticipated further learning curve, we would expect these metrics to continue to improve. We did not observe the changes in MIS for pancreatic cases, as these cases are likely more technically challenging and potentially involve a greater learning curve than the 33 cases reported here. Braga et al. demonstrated a reduction in conversion rate, operative time, and operative blood loss after their first 10 procedures yet did not report significant differences in blood loss after 30 consecutive MIS pancreas cases. 15 It is unclear how this change with the continued use of laparoscopic and robotic surgery at our institution and improved proficiency with these techniques. Though not abundant, there are randomized trials that have already begun to demonstrate noninferiority of MIS HPB.35,36
The primary limitations of this study stem from the retrospective design that was undertaken. We recognize there was significant selection bias in patients undergoing MIS compared to open techniques. Surgical approaches were tailored based on case complexity and surgeon preference. Overall, operative techniques are still surgeon-dependent, considering that the National Comprehensive Cancer Network (NCCN) and other organizations have been slow to address the role of MIS in HPB cancer surgery. Decisions regarding surgical approach are dependent on a number of factors, including tumor-related variables, patient preference, patient financial or logistical factors, physician preference, and other reasons that could not be captured via retrospective data collection. Therefore, substantial differences between patients who underwent MIS and those who underwent open HPB surgery are likely. The immeasurable confounders and vastly different patient populations, including the surgeries performed, thus could not be accounted for utilizing a multivariate analysis. We were also unable to utilize propensity score matching due to this variability and our small sample size. Additionally, treatment regimens, including perioperative management strategies, were not standardized, and likely impacted outcomes between groups.
Lastly, this study does not represent the immediate commencement of MIS HPB surgery in our institution. However, due to the low number of cases performed prior to the dates of this analysis, we feel this study is more indicative of the true transition to a high-volume MIS program. Throughout the course of this study, we were unable to account for the sudden increase in MIS cases during this time period or the preparations, if any, that were made by the health system to handle the increase in cases. We did not incorporate the cost of implementing the MIS program within our health system as this study looks at cases performed by multiple surgeons at multiple hospitals. The focus of this study was the safety of the program, though these questions are important to address and would be worthwhile to investigate in a future study. Due to our small sample size, our analysis combines laparoscopic and robotic approaches into the aggregate of MIS and, although there are likely differences in outcome measures within these populations, they are unlikely to affect the conclusions within the context of our study. This would be a valuable area for a future study looking at the program several years out from inception and comparing the outcomes and case complexity as the program has evolved, as well as how the health system has been affected.
In the context of these limitations, these data support the safety of implementation of MIS HPB. With appropriate expertise, we expect reproducibility of these outcomes at other centers.
Footnotes
Author’s Note
Portions of these data were presented at the 2022 American College of Surgeons Quality and Safety Conference, Chicago, IL, July 15-18, 2022.
Acknowledgments
The authors thank Sarah Carey, MS, Jade Chang, and Jacalyn Newman, PhD, of Allegheny Health Network’s Health System Publication Support Office (HSPSO) for their assistance in editing and formatting the manuscript. The HSPSO is funded by Highmark Health (Pittsburgh, PA, United States of America) and all work was done in accordance with Good Publication Practice (GPP3) guidelines (![]() ).
).
Author Contributions
SJF was directly responsible for all aspects of the study. She participated in the collection, analysis, and interpretation of data and drafting and revision of the manuscript, figures, and tables. CM, DK, and SD participated in the analysis and interpretation of data and drafting and revision of the manuscript, figures, and tables. PR, SCS, PLW, and DLB participated in the review and revision of the manuscript, figures, and tables. CJA had overall responsibility for the study, including conception and experimental design, analysis and interpretation of data, drafting and revision of the manuscript, obtaining funding for the project, and supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.