
Abstract
Aim
To ascertain the safety and feasibility of robotic simultaneous resection of synchronous colorectal cancer and liver metastases.
Methods
A PRISMA-compliant systematic review with proportion meta-analysis was conducted. All retrospective or prospective observational studies including patients aged ≥ 18 with synchronous colorectal cancer and liver metastases undergoing robotic simultaneous resection were eligible. The outcomes included conversion to open, operative time, intraoperative blood loss, Clavien-Dindo ≥ III complications, 30-day mortality, anastomotic leak, R0 resection, and length of hospital stay.
Results
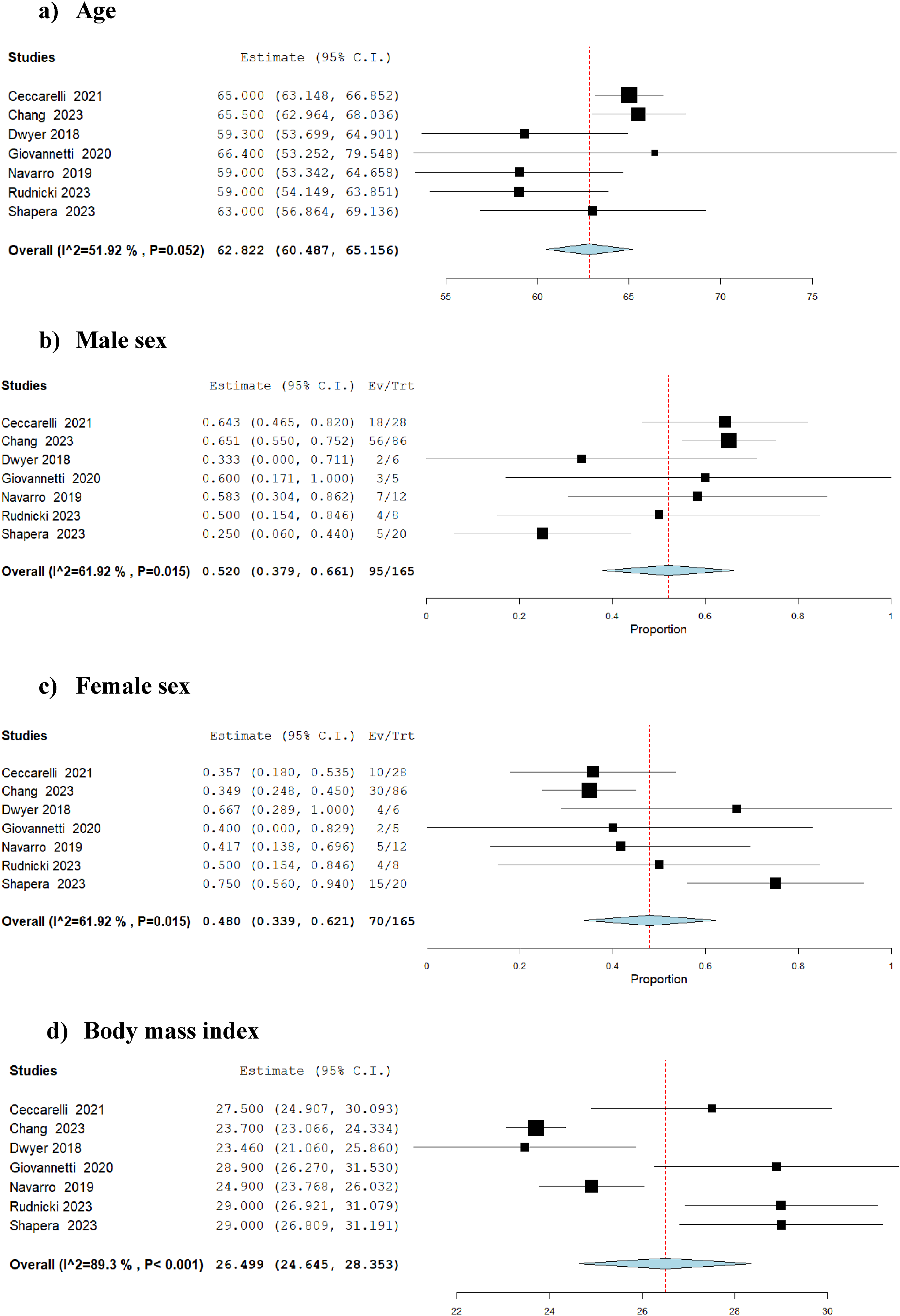
Seven eligible studies including 165 patients were identified. The mean age was 62.8 years (95% CI: 60.5-65.2), mean body mass index was 26.5 (95% CI: 24.6-28.4), and 52.0% (95% CI: 37.9-66.1) were male. The mean operative time was 406.5 min (95% CI: 358.2-454.7) and mean intraoperative blood loss was 150.0 mL (95% CI: 124.5-175.6). Conversion to open occurred in 3.9% (95% CI: 1.0-6.8), Clavien-Dindo ≥ III complications in 9.3% (95% CI: 4.7-13.8), 30-day mortality in 0.9% (95% CI: 0.0-2.4), and anastomotic leak in 4.3% (95% CI: 0.9-7.6). R0 resection was achieved in 99.0% (95% CI: 97.5-100), and the mean length of hospital stay was 6.7 days (95% CI: 5.5-7.9).
Conclusions
Single-arm meta-analysis suggests that robotic simultaneous resection of synchronous colorectal cancer and liver metastases may not only be feasible and safe but also may be advantageous in terms of conversion avoidance, complexity handling, and perioperative recovery. More studies with larger sample size are required to inform long-term oncological outcomes and selection criteria and to provide comparative evidence.
Introduction
Colorectal cancer is a major contributor to cancer mortality and ranks as the third most commonly diagnosed malignancy worldwide, with 25-30% of those affected developing liver metastasis.1,2 The gold standard treatment remains surgical resection with curative intent for long-term survival. 3 Advances in diagnostic modalities, introduction of modern chemotherapy and biological agents, improvement in perioperative care, and advances in operative techniques have pushed the limits of surgical resection of colorectal liver metastasis. 4 Consequently, simultaneous resection of synchronous colorectal cancer and liver metastases is being practiced more frequently with comparable outcomes to the conventional staged resection approach. 5
In parallel to the expanding indications for surgical resection of synchronous colorectal cancer and liver metastases, the indications for minimally invasive techniques for resection of synchronous colorectal cancer and liver metastases are expanding. 6 While the feasibility and safety of laparoscopic simultaneous resection of synchronous colorectal cancer and liver metastases have been demonstrated, 7 the feasibility and safety of robotic approach remain poorly understood. Therefore, we aimed to conduct a systematic review and meta-analysis to assess the feasibility and safety of robotic simultaneous resection of synchronous colorectal cancer and liver metastases.
Methods
Methodological and Reporting Compliance
This study was designed and documented following the guidelines outlined in the Cochrane Handbook of Systematic Reviews (version 6.4) 8 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. 9
Registration and Protocol
This study complied with the predefined protocol as registered in PROSPERO, a transparent international database for prospectively registered systematic reviews.
Eligibility Criteria
Study Design
All retrospective and prospective studies (case-control studies, case series, cohort studies, and randomized control trials) were eligible for inclusion. Correspondences, letters, case reports, scoping reviews, systematic reviews, and meta-analyses were excluded.
Population
All patients aged 18 and older with synchronous colorectal cancer and liver metastases were eligible for inclusion.
Intervention and Comparison
Robotic simultaneous resection of synchronous colorectal cancer and liver metastases was the intervention of interest. The study was single-arm meta-analysis with no comparison arm.
Outcomes
The outcomes of interest included conversion to open, operative time, intraoperative blood loss, complications (Clavien-Dindo ≥ III), 30-day mortality, anastomotic leak, R0 resection, and length of hospital stay.
Information Sources and Search Strategy
A thorough search strategy was designed and applied across multiple electronic databases using relevant keywords, filters, thesaurus terms, and Boolean operators to ensure comprehensive results. PubMed, Embase, MEDLINE, and Scopus were utilized. Two authors with experience in evidence synthesis developed and executed the search strategy, applying no language limitations, on the 9th of April 2025. The search strategy is shown in Supplemental Table 1.
Study Selection, Data Collection, and Data Items
Two authors independently reviewed the titles and abstracts of the identified studies using the predefined eligibility criteria to identify potentially eligible studies. Following this step, the full texts for articles deemed potentially relevant were obtained and reviewed. The articles that conformed to the eligibility criteria were selected. When discrepancies arose between the two authors concerning study selection, a third author was consulted to provide an independent judgment. The data items were chosen by authors experienced in evidence synthesis during the protocol development stage through the pilot testing technique on randomly selected articles. These were recorded on an electronic data sheet by two authors and subsequently reviewed by an independent author. The data items included bibliometric parameters, type of study design, demographics of the population, body mass index, conversion to open, operative time, intraoperative blood loss, complications (Clavien-Dindo ≥ III), 30-day mortality, anastomotic leak, R0 resection, and length of hospital stay.
Study Risk of Bias and Evidence Certainty Assessments
Joanna Briggs Institute (JBI) Critical Appraisal tool was used for risk of bias assessment, and the GRADE system was used to assess the certainty of evidence. 10 Both steps were conducted by two independent authors; when discrepancies arose between the two authors, a third author was consulted to provide an independent judgment.
Effect Measures and Synthesis Methods
OpenMeta[Analyst] software was used for single-arm meta-analysis. The DerSimonian-Laird random-effects method (confidence level: 95%; correction factor: 0.5) was used to calculate the weighted pooled summary measures for baseline characteristics (age, sex, and body mass index) and outcomes (conversion to open, operative time, intraoperative blood loss, Clavien-Dindo ≥ III complications, 30-day mortality, anastomotic leak, R0 resection, and length of hospital stay). The unit of analysis was individual patient, and intention-to-treat data were used for the analyses. Statistical heterogeneity was measured as I2 using Cochran’s Q test (χ2), and heterogeneity was classified as low when I2 was 0-25%, moderate when I2 was 25-75%, and high when I2 was 75-100%. Separate analyses for studies with low overall risk of bias and leave-one-out analysis were performed as sensitivity analyses.
Assessment of Reporting Bias
As per the protocol, in order to assess the risk of reporting bias, we intended to develop a funnel plot if an outcome was reported by at least 10 studies; however since this was not the case, reporting bias could not be examined.
Protocol Compliance
The study strictly complied with the registered protocol.
Results
Study Selection
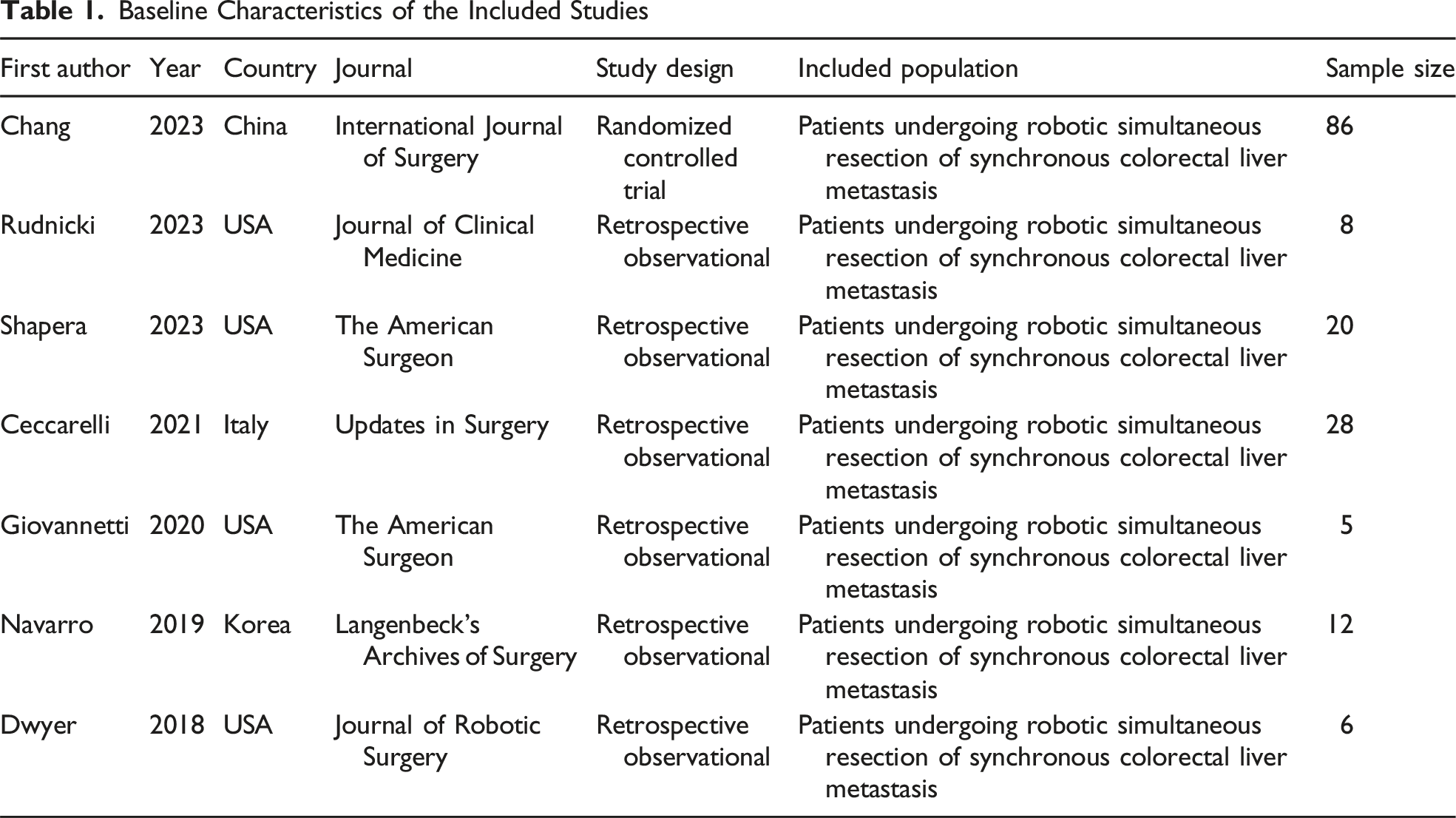
The selected search strategy described above yielded 125 articles (PubMed: 19, Embase: 55, MEDLINE: 23, and Scopus: 28). After elimination of duplicates and screening process of title and abstract, 118 articles were excluded directly as they did not meet the principal eligibility criteria. The remaining seven studies11-17 satisfied inclusion criteria and were confirmed for inclusion after full-text review. A total of 165 patients with a mean age of 62.8 years (95% CI: 60.5-65.2) were included; 52.0% (95% CI: 37.9-66.1) were male and the mean body mass index was 26.5 (95% CI: 24.6-28.4). Figure 1 demonstrates study flow chart, Table 1 shows the baseline characteristics of the eligible studies, and Figure 2 demonstrates meta-analysis of the available baseline characteristics. Study PRISMA Flow Diagram Baseline Characteristics of the Included Studies Forest Plots for Proportion Meta-Analysis of Available Baseline Characteristics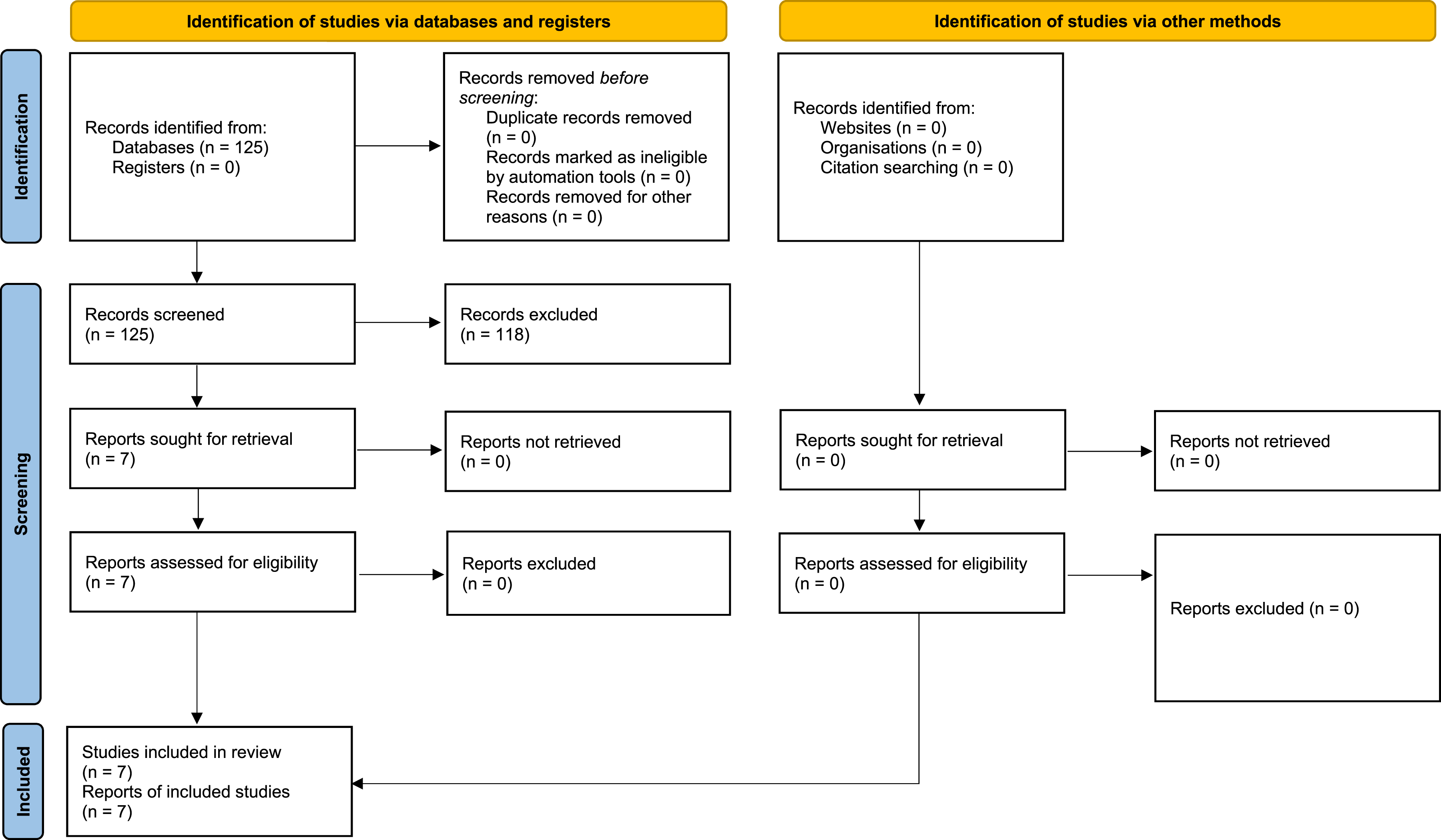
Risk of Bias
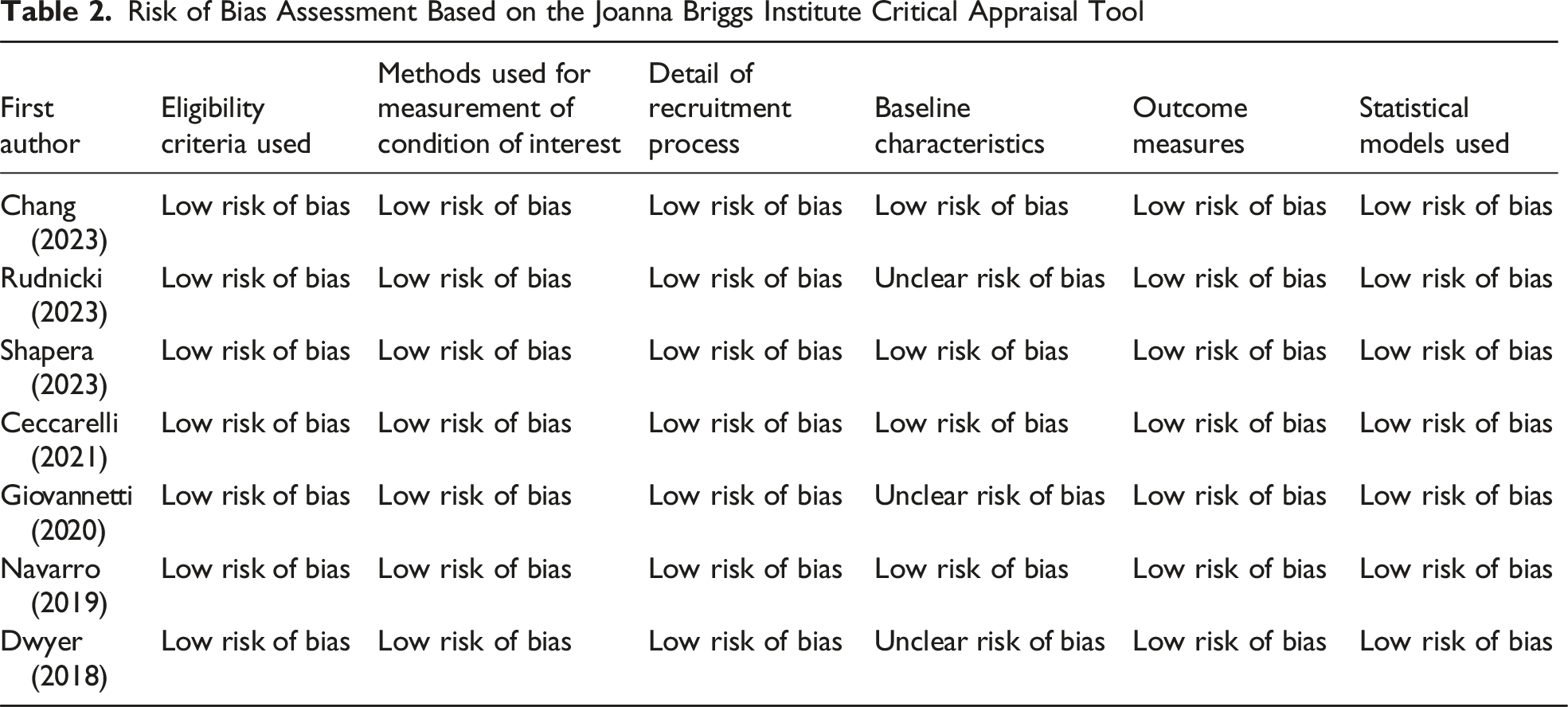
Risk of Bias Assessment Based on the Joanna Briggs Institute Critical Appraisal Tool
Type of Liver and Colorectal Resections
Detail of Liver and Colorectal Resections Performed
*Major liver resection was defined as resection of ≥ 3 liver segments.
Outcomes
Conversion to Open
Pooled analysis of 165 patients from seven studies showed that the likelihood of conversion to open surgery was 3.9% (95% CI: 1.0-6.8%) with a low level of statistical heterogeneity (I2 = 0%) (Figure 3). The GRADE certainty was high. Forest Plots for the Outcomes of Robotic Simultaneous Resection of Synchronous Colorectal Liver Metastasis
Operative Time
Pooled analysis of 165 patients from seven studies showed that the mean operative time was 406.4 min (95% CI: 358.2-454.7) with a high level of statistical heterogeneity (I2 = 95%) (Figure 3). The GRADE certainty was moderate.
Intraoperative Blood Loss
Pooled analysis of 165 patients from seven studies showed that the mean volume of intraoperative blood loss was 150.0 mL (95% CI: 124.5-175.6) with a moderate level of statistical heterogeneity (I2 = 66%) (Figure 3). The GRADE certainty was moderate.
Complications (Clavien-Dindo ≥ III)
Pooled analysis of 154 patients from five studies showed the risk of Clavien-Dindo ≥ III complications was 9.3% (95% CI: 4.7-13.8) with a low level of statistical heterogeneity (I2 = 0%) (Figure 3). The GRADE certainty was high.
30-Day Mortality
Pooled analysis of 165 patients from seven studies showed that the risk of 30-day mortality was 0.9% (95% CI: 0-2.4) with a low level of statistical heterogeneity (I2 = 0%) (Figure 3). The GRADE certainty was high.
Anastomotic Leak
Pooled analysis of 137 patients from six studies showed that the risk of anastomotic leak was 4.3% (95% CI: 0.9-7.6%) with a low level of statistical heterogeneity (I2 = 0%) (Figure 3). The GRADE certainty was high.
R0 Resection
Pooled analysis of 165 patients from seven studies showed that R0 resection was achieved in 99.0% (95% CI: 97.5-100) with a low level of statistical heterogeneity (I2 = 0%) (Figure 3). The GRADE certainty was high.
Length of Hospital Stay
Pooled analysis of 165 patients from seven studies showed that the mean length of hospital stay was 6.7 days (95% CI: 5.5-7.9) with a high level of statistical heterogeneity (I2 = 88%). The GRADE certainty was moderate.
Sensitivity Analyses
The results of the analyses for all the outcomes remain consistent when studies with a low overall risk of bias were analyzed separately and through leave-one-out analysis.
Discussion
This systematic review and meta-analysis assessed the feasibility and safety of robotic simultaneous resection of synchronous colorectal cancer and liver metastases. Analysis of seven studies (165 patients) showed that robotic simultaneous resection of synchronous colorectal cancer and liver metastases was feasible as indicated by acceptable operative time, conversion to open rate, and R0 resection rate and it was safe as indicated by acceptable risks of major morbidity and mortality. The GRADE certainty of evidence was moderate.
The results of current study have external validity. Machairas et al 18 conducted a narrative systematic review of 29 patients which concluded that robotic simultaneous resection of synchronous colorectal cancer and liver metastases may be safe and feasible in selected patients. The evidence provided by the study was limited to six case reports and three case series, and the authors were not able conduct formal statistical analyses due to the limited sample size. The current study included a total of seven case series and excluded case reports; the study has a larger sample size with formal statistical analyses including assessment of heterogeneity and certainty of the available evidence. Therefore, while the results of the current study support the findings of the study by Machairas et al, 18 the current study provides more robust evidence with a lower likelihood of type 2 error.
In another study, Radomski et al 19 compared outcomes of 79 patients who underwent robotic simultaneous resection of synchronous colorectal cancer and liver metastases with 266 laparoscopic and 1376 open cases; the authors concluded that robotic approach is associated with a lower conversion to open and length of hospital stay in comparison with the laparoscopic approach and a lower risk of postoperative ileus compared with open approach. 19 Moreover, the randomized controlled trial conducted by Chang et al 11 showed that robotic simultaneous resection of synchronous colorectal cancer and liver metastases was associated with fewer complications, less blood loss, faster bowel function recovery, and shorter hospital stay in comparison to open approach without compromising oncological outcomes. 11 All of the above may suggest that not only robotic simultaneous resection of synchronous colorectal cancer and liver metastases is safe and feasible but also it may provide advantages in comparison with laparoscopic and open approaches.
In addition to the studies conducted in robotic setting, the results of current study can be compared with previous reviews which evaluated outcomes of laparoscopic approach. Morarasu et al 7 evaluated outcomes in 620 patients undergoing laparoscopic simultaneous resection of synchronous colorectal cancer and liver metastases and reported an R0 resection rate of 93%, major complication rate of 11%, and anastomotic leak rate of 4%. In another study, Pan et al 20 evaluated 273 patients undergoing laparoscopic simultaneous resection of synchronous colorectal cancer and liver metastases which confirmed feasibility and safety of laparoscopic approach. Although the studies by Morarasu et al 7 and Pan et al 20 did not evaluate robotic technique, due to the technical similarities between the robotic and laparoscopic approaches the results of both studies may be used to support the external validity of the findings of current study.
The safety and feasibility of robotic surgery have been demonstrated in liver surgery21,22 and colorectal surgery23-25 which may explain why it is also safe in simultaneous resection of synchronous colorectal cancer and liver metastases. Meta-analysis of six studies (295 patients) showed that robotic radical resection of hilar cholangiocarcinoma is safe and feasible in selected patients. 21 Moreover, meta-analysis of seven studies (319 patients) confirmed safety and feasibility of robotic lateral hepatic sectionectomy. 22 The safety and feasibility of robotic approach in colorectal setting have also been demonstrated in several meta-analyses.23-25 Consequently, provided that appropriate cases are selected, robotic simultaneous resection of synchronous colorectal cancer and liver metastases is safe and feasible.
Although the findings of this current study highlight that robotic simultaneous resection of synchronous colorectal cancer and liver metastases is safe and feasible, we must accept that the available evidence is limited. The available evidence is derived mainly from retrospective studies with a small sample size. This would subject the available evidence to type 2 error and inevitable selection bias. On the other hand, lack of adequate comparative studies would make it impossible to identify potential benefits of robotic approach in comparison with alternative approaches such as laparoscopic or open techniques in this setting. Absence of comparison arm in the current study may not facilitate decision making in terms of selection of most effective approach; therefore, until robust comparative evidence is available, the decision about the most effective approach should be made based on patient’s characteristic, surgeon’s experience, and available resources. The included studies provided limited data related to tumor characteristics; therefore, subgroup analysis based on tumor characteristics was not possible. Moreover, only 16% of included patients underwent major liver-major colorectal resections and the available data was not adequate to conduct subgroup analysis based on this cohort of patients. Consequently, although the results of the current study provide a robust basis for hypothesis synthesis and power analysis in future prospective studies, definite conclusions cannot be made.
The limitations of this study are mainly related to the available evidence (as highlighted above) rather than its design. The current study followed a predefined protocol and a systematic approach in evidence synthesis. The quality and certainty of available evidence were evaluated and when applicable, they were downgraded. The between-study heterogeneity was low for most of the outcomes with high GRADE certainty. Moreover, the robustness of the results was evaluated and confirmed by appropriate sensitivity analyses. However, we could not exclude reporting bias because none of the outcomes were reported by more than 10 studies.
Conclusions
Single-arm meta-analysis suggests that robotic simultaneous resection of synchronous colorectal cancer and liver metastases may not only be feasible and safe but also may be advantageous in terms of conversion avoidance, complexity handling, and perioperative recovery. More studies with a larger sample size are required to inform long-term oncological outcomes and selection criteria and to provide comparative evidence.
Supplemental Material
Supplemental Material - Safety and Feasibility of Robotic Simultaneous Resection of Synchronous Colorectal Cancer and Liver Metastases: A Systematic Review and Meta-Analysis
Supplemental Material for Safety and Feasibility of Robotic Simultaneous Resection of Synchronous Colorectal Cancer and Liver Metastases: A Systematic Review and Meta-Analysis by Pablo Suarez Benitez, Anastasia Efstathiou, Muhammed Safiru, Shahin Hajibandeh, Shahab Hajibandeh, and Thomas Satyadas in The American Surgeon
Footnotes
Consent to Participate
Patient consent and approval from Research Ethics Committees were not required in this study because the study design was a meta-analysis which did not have direct involvement of patients and used non-identifiable data.
Author Contributions
Conception and design: TS and Shahab H; data collection and data analysis: AE, PS, and Shahab H; analysis and interpretation: Shahab H and Shahin H; writing the article: AE, PS, and Shahab H; critical revision of the article: all authors; final approval of the article: all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The corresponding author (Shahab H) will provide any additional data related to this study on reasonable request.
PROSPERO Registration Number
The PROSPERO registration number for the protocol was CRD420251070631.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.