
Abstract
Nutcracker syndrome (NCS) is the clinical manifestation of unilateral renal venous hypertension. It develops secondary to the nutcracker phenomenon caused by compression of the left renal vein between the superior mesenteric artery and the aorta. We present the case of a 43-year-old female with a history of left flank pain, pelvic congestion, and hematuria secondary to NCS. The patient frequently required high-dose non-steroidal anti-inflammatory medications with minimal relief. She initiated a kidney donor evaluation after electing to undergo a nephrectomy for the possible long-term resolution of NCS symptoms. If diagnosed early, NCS does not generate pathology within the kidney. This finding allows an individual with medically refractory NCS to avoid the morbidity of a complex surgical procedure by instead donating their kidney. Attention to this treatment modality could provide individuals with NCS resolution of symptoms while providing someone with end-stage renal disease with a life-saving organ.
The nutcracker phenomenon (NCP) is an anatomical finding of the left renal vein (LRV) compressed between the abdominal aorta and the superior mesenteric artery (SMA). The result is stenosis of the LRV and dilation of the distal end. The clinical presentation that describes patients with NCP is nutcracker syndrome (NCS), also known as left kidney vein entrapment syndrome. 1 Prevalent clinical manifestations include left flank pain, hematuria, proteinuria, varicocele in male patients, and ovarian vein out-flow obstruction in female patients. 2 The NCP appears to provoke these symptoms in some patients but not others, for reasons that remain unclear. Nonetheless, the pathophysiology behind a decreased aortomesenteric distance is contingent on weight loss that results in loss of retroperitoneal fat. 1
Without uniform guidelines for NCS, treatment approaches vary widely. Conservative management emphasizing weight gain is recommended for cases presenting with mild to tolerable symptoms, especially for individuals with low BMIs and under the age of eighteen. NCS pharmacological interventions include angiotensin converting enzyme (ACE) inhibitors, preferably Alacepril, and aspirin. 2 Vascular treatment modalities involve external vascular stenting with ring reinforced polytetrafluoroethylene grafts around the LRV between the inferior vena cava and the gonadal and adrenal branches of the LRV. 1 Alternatively, intravascular options offer both balloon-expandable and self-expanding stents. 1 Surgical interventions for treating the entrapment produced by a decreased aortomesenteric angle include LRV transposition, gonadal vein transposition (GVT), and renal autotransplantation (RAT). 2 Due to the morbidity of these procedures, patients with an adequate renal function that do not respond to medical treatment may elect to undergo a left nephrectomy. 2
There are currently 97,362 people on the kidney transplant waiting list in the United States. 3 On average, 140 people were added daily to the kidney waiting list in the last 30 days (05/01/2022). 3 In 2021, OPTN data recorded 24,671 kidney transplants performed with only 5,972 from living donors. 3 It is in this context that a patient with medically refractory NCS and a kidney poised for discard might provide a lifesaving organ for someone with end-stage renal disease (ESRD) awaiting transplant.
A 43-year-old female with a BMI of 23.1 kg/m2 and no prior abdominal surgeries presents to our transplant surgical clinic with a history of left flank pain, pelvic congestion, and hematuria secondary to NCS. The patient initially underwent computed tomography (CT) scan which revealed a 1-2 mm non-obstructing kidney stone and a small renal cyst. Seven months later, the patient presented to the ER with pain primarily adjacent to her upper lumbar spine that radiated around her left flank with associated nausea, vomiting, and hematuria. The patient noted that the hematuria worsened with exercise. She intermittently required high-dose non-steroidal anti-inflammatory medications. A contrast-enhanced CT abdomen and pelvis was performed showing images compatible with anterior NCS (Figure 1). Stenting was not a possible treatment option due to a significant allergy to nickel. Surgical options were discussed and the patient preferred nephrectomy over autotransplantation and other complex in-situ vascular revision due to the early post-surgical recovery difference. Representative images of CT body scan showing NCS. 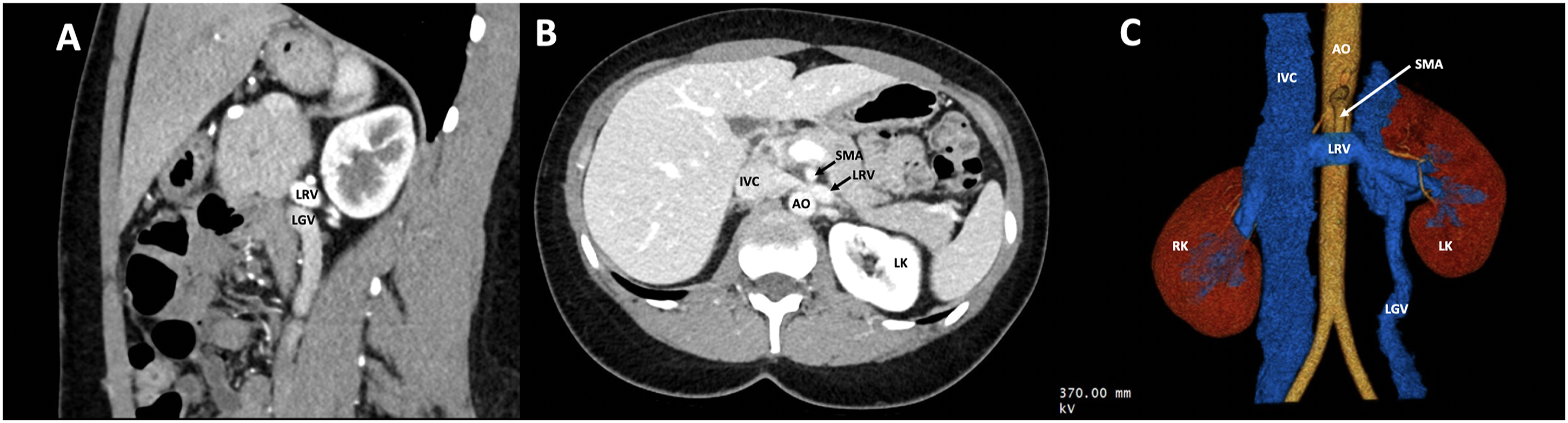
At this juncture of the evaluation of her left kidney, she explored donation and was evaluated at our institution. The patient underwent a thorough work-up, which included a CT body scan (Figure 1), unremarkable laboratory studies, and a glomerular filtration rate (GFR) of 115 mL/min when corrected, with a 47% (left) 53% (right) split. The patient was extensively assessed during the kidney donor evaluation and noted to have no apparent medical contraindication. After careful consideration, the risk of donation for the patient with NCS was calculated to be the same as any other donor. The patient met all institutional medical, surgical, and psychosocial criteria and then underwent a laparoscopic left nephrectomy without complications. Due to the size of the gonadal vein, it was stapled with an endoGIA. Zero-hour biopsy revealed 35 glomeruli, 0% sclerosed, no significant intimal sclerosis in arteries or hyalinosis in afferent arterioles, minimal interstitial fibrosis, no significant inflammation or cellular infiltration, and minimal tubular atrophy. The donor was discharged on post-op day 2. The kidney recipient remains off dialysis almost 3 years later, and the donor experienced resolution of the pain, hematuria, and other symptoms she suffered before the nephrectomy.
NCS is a rare anatomical condition. It can present at any age, but there is a peak in young and middle-aged adults. 2 Diagnostic imaging techniques include contrast-enhanced CT or magnetic resonance imaging (MRI). With a sagittal view, the aortomesenteric angle (AMA) or the angle between the SMA and aorta can be measured abnormally low in NCS. Additionally, axial CT imaging can display stenosis of the LRV within the AMA, and an engorged left gonadal vein. First line management should include observation, weight gain, aspirin, or ACE inhibitors. 2 If the pain is unresponsive to conservative options, surgical treatment can be discussed. Long term data on stent efficacy in the NCS population is unavailable, but potential risks include stent migration, in-stent restenosis, deformities, and erosion of the placement site. 1 Furthermore, stenting, and surgical therapies, do not offer a definitive resolution of flank pain. Currently, nephrectomy is the most successful line of treatment for NCS and can potentially be made more difficult by previous stenting interventions.
These concerns and the inability to successfully manage her symptoms medically led our patient to seek a nephrectomy. She refused autotransplantation and vascular reconstruction to avoid the morbidity of more complex and perhaps unnecessary surgery, given her more than adequate renal function. The unique aspect of our patient’s history is that she initiated a kidney donor evaluation once she chose to proceed with nephrectomy for the possible relief of NCS symptoms. People with NCS can be eligible for kidney donation because the entrapped LRV does not generate pathology within the glomeruli or renal tubules in the short term. After graft nephrectomy, the donor should find relief of symptoms from NCS, while the recipient’s graft begins to function effectively within hours.
Kidney donation can save one of the 97,362 people currently on the kidney transplant waiting list in the United States 3 and simultaneously relieve the symptoms of the donor experiencing the painful effects of NCS. Successful living kidney donations have been performed on initially undiagnosed or asymptomatic NCS patients whose decreased AMA is discovered during the preoperative donor evaluation. 4 It is important to note that these patients initially donated their kidneys to a loved one and not as a treatment option for NCS. It is difficult to determine how many nephrectomies are performed annually for NCS or other similar conditions, but attention to this phenomenon in the surgical and urologic community could help other ESRD patients given the great unmet need for kidneys worldwide.
The nephrectomy benefits a patient with pain, hematuria, and other symptoms secondary to NCS. The otherwise healthy and available kidney offers greatly improved survival and quality of life to a patient mired on dialysis. A further and distant third benefit of the transplant is a cost-savings vs continued dialysis for the healthcare system. Our case truly highlights an example of a win-win in modern medicine.
We propose that medically refractory NCS individuals eligible for autotransplantation be considered as possible candidates for living kidney donation and presented with this option during treatment and management consultations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.