
Abstract
Background
Our objective was to evaluate differences in baseline characteristics, complications, and mortality among patients receiving a gastrostomy tube (GT) by surgical or non-surgical services.
Methods
We performed a retrospective analysis of adult patients who underwent GT placement from 2014 to 2017 at a single institution. Using bivariate and multivariable analyses, we compared baseline characteristics, complications, and overall 30-day mortality of patients undergoing GT placement with surgical or non-surgical services.
Results
Of the 1339 adults who underwent GT placement, surgical and non-surgical services performed 45% (n = 609) and 55% (n = 730) procedures, respectively. Gastrostomy tube-related complications were similar (29.6% surgical vs 28.8% non-surgical, P = .76). Thirty-day mortality was higher among non-surgical services (23.7% vs 16.5%, P = .004). On multivariable analysis, this was not significant (OR 1.21, 95% CI 0.83; 1.77).
Conclusion
Surgical and non-surgical service placement of GTs had equivalent GT-related mortality and complication rates.
Key Takeaways
Short-term complications after gastrostomy tube (GT) placement were common. Gastrostomy tube complications/mortality did not differ by placement service (surgical and non-surgical). Need for GT likely a proxy indicator for frailty/increased short-term mortality.
Introduction
In patients who are unable to tolerate oral intake, at risk of malnutrition, and those requiring long-term nutrition support, gastrostomy tube (GT) placement is indicated. 1 The underlying etiology mandating the indication for GT placement includes traumatic brain injury, respiratory failure, head and neck cancer, and esophageal disease, among many others. Conventional modalities for GT placement include percutaneous endoscopic gastrostomy (PEG), surgical (laparoscopic and open techniques), and radiologic-guided placement. Percutaneous endoscopic gastrostomies are often preferred as they are less expensive and can be efficiently placed by either a surgical team or medical proceduralists. 2 However, some patients may require an operative approach for GT placement due to special anatomic considerations such as prior abdominal surgery, esophageal obstruction, or colonic interposition. 3 Previous studies demonstrate no difference in morbidity or mortality between PEG and operative gastrostomy.2,4
While previous studies have focused on GT outcomes by placement modality (PEG vs radiologic-guided and laparoscopic vs open), there is a paucity of data regarding differences in the prevalence of complications based on the characteristics of procedural service, specifically medical proceduralists such as gastroenterologists compared to surgical teams. Though experienced endoscopists and surgeons may not differ in technical ability to place a GT, they may draw from different patient populations with different underlying risk profiles, or they may have differences in post-procedural care that can lead to differences in post-procedure outcomes. Therefore, the primary aim of this study was to describe baseline patient characteristics, complications, and mortality among patients who have had GTs placed by either a surgical or non-surgical team. Our null hypothesis was that GT outcomes would be equivalent between surgical and non-surgical services.
Methods
The University of North Carolina Institutional Review Board reviewed the study protocol and approved this study, and informed consent was waived given the retrospective nature of the study (IRB No. 17-3075).
We performed a retrospective descriptive cohort study of all patients who underwent GT placement between March 2014 and July 2017 at a single institution, an academic tertiary care level 1 trauma center with a comprehensive cancer hospital. We identified patients in the electronic medical record system based on ICD-9 and 10 codes. We excluded children (<18 years) and duplicate patients who had their GT replaced for dislodgement or leaking, or those who had procedures aborted and never had a GT placed. We did include patients with aborted procedures that subsequently underwent GTs placed by another service line. We included 1339 patients in our analysis (Figure 1). We also collected the following demographic and health data for each patient: sex, age at placement, BMI, tobacco use (never, former, and current), and discharge disposition {home with self-care, home with home health, facility (transfer to another hospital including long-term acute care hospitals [LTACH] and skilled nursing facilities), inpatient rehab, inpatient death, or hospice}. Cohort selection for gastrostomy procedures.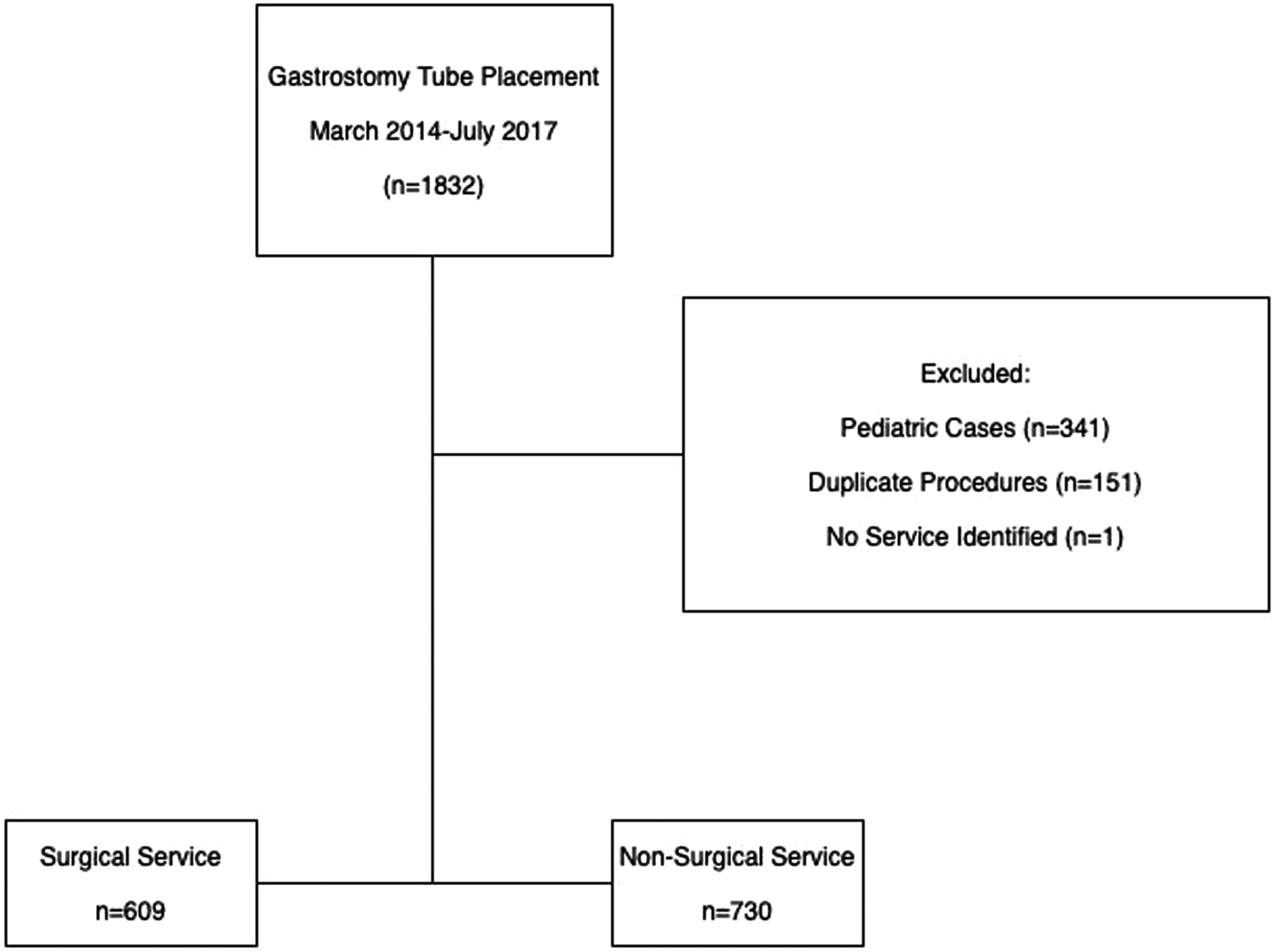
We dichotomized the performing service into surgical and non-surgical. Surgical services that place GTs in adults at our institution include trauma/critical care surgery, surgical oncology, gastrointestinal surgery, minimally invasive surgery, transplant surgery, burn surgery, cardiothoracic surgery, and gynecologic-oncologic surgery. Non-surgical services included pulmonary critical care, gastroenterology, and vascular interventional radiology. We classified the GT placement technique as percutaneous, laparoscopic, or open. Those placed by radiology were classified as percutaneous. Therefore, those classified as “percutaneous” and performed by a surgical service were all PEGs, and those classified as percutaneous on a non-surgical service could be either a PEG placed by a medical proceduralist team or a radiologic-guided placement.
We performed a manual chart review for each patient. Comorbidities were identified, including diagnosis of any congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), dementia, and acute or chronic renal failure. We classified the primary indication for GT placement as malnutrition (including failure to thrive and short gut syndrome), neurologic (including traumatic brain injury, cerebrovascular disease, psychomotor, other neurologic), anatomic (including congenital anomalies, intraoperative/structural reasons [eg, as gastropexy with hiatal hernia repair]), and cancer or palliative (including non-palliative esophageal or head and neck cancers and any palliative decompression).
The primary outcome was all-cause 30-day mortality. We additionally examined 30-day mortality attributable to GT placement. Gastrostomy tube complications included mechanical (dislodgement without need for operation, leakage, pressure wound, and clogging), infectious (cellulitis and abscess), and minor bleeding, and we defined significant complications as any complication potentially requiring operative intervention (eg, necrotizing soft tissue infection [NSTI], peritonitis, organ injury, gastrocutaneous [GC] fistula requiring reoperation, and significant bleeding) or a GT-related death. We chose not to use the Clavien-Dindo scale 5 as we wanted to be more specific about the complication profile rather than use a summary measure of complication severity. To ensure consistency of the chart review process, we randomly selected 200 charts for reviewers by 2 independent reviewers, and we compared their results.
We calculated descriptive statistics using frequency and percentage for categorical variables, mean and standard deviation for normally distributed continuous variables, or median and interquartile range (IQR) for non-normally distributed variables. As determined by cell size, we used chi-square or Fisher’s exact tests to evaluate statistical differences for categorical variables. Likewise, we used the t-test to compare means and the Wilcoxon test to compare medians. We utilized multivariable logistic regression to examine the odds of any complications and 30-day all-cause mortality by service, respectively. We adjusted for baseline demographic variables as well as those that may influence short-term mortality. These were chosen a priori and included age, sex, indication for placement, and comorbidities. We also performed a subgroup analysis where we limited the analyses to only PEG procedures in order to compare surgical and non-surgical teams to a single procedure. We used SAS statistical software v9.4 (Cary, NC) for all statistical analyses, and two-sided P-values <.05 were considered statistically significant.
Results
Baseline Characteristics and Complications by Performing Service.
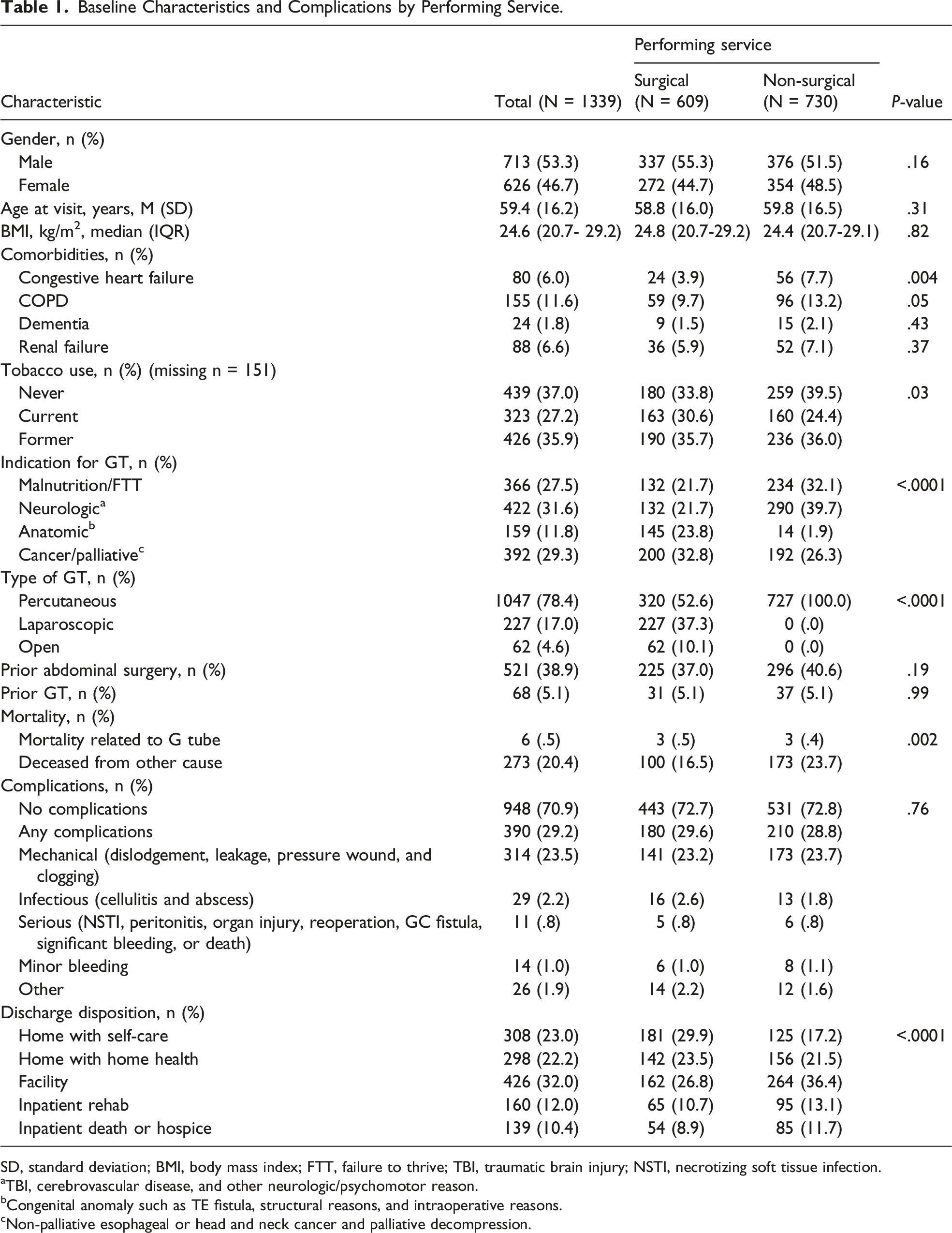
SD, standard deviation; BMI, body mass index; FTT, failure to thrive; TBI, traumatic brain injury; NSTI, necrotizing soft tissue infection.
aTBI, cerebrovascular disease, and other neurologic/psychomotor reason.
bCongenital anomaly such as TE fistula, structural reasons, and intraoperative reasons.
cNon-palliative esophageal or head and neck cancer and palliative decompression.
Disposition from the hospital was most commonly to another facility, such as a skilled nursing facility (32.0%) followed by home with self-care (23.1%), home with home health nursing (22.4%), and inpatient rehabilitation (12.0%). The most common disposition among surgical services was home with self-care (29.9%) and to another facility (36.6%) among non-surgical services (Table 1).
Odds of Gastrostomy Tube Complications and Mortality by Placement Service.
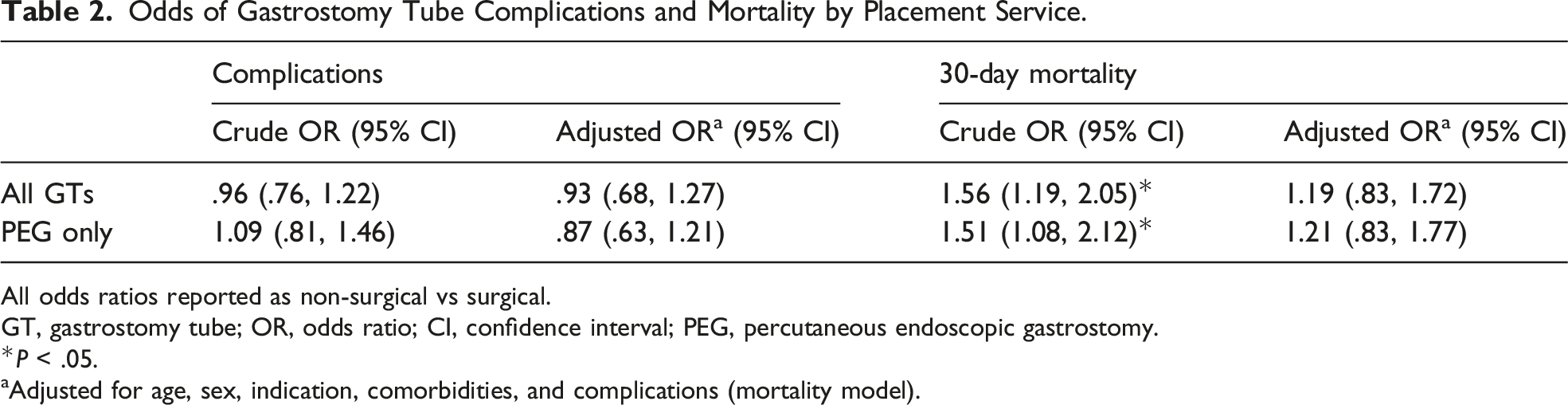
All odds ratios reported as non-surgical vs surgical.
GT, gastrostomy tube; OR, odds ratio; CI, confidence interval; PEG, percutaneous endoscopic gastrostomy.
*P < .05.
aAdjusted for age, sex, indication, comorbidities, and complications (mortality model).
Gastrostomy Tube Population Characteristics by 30-Day Overall Mortality and Cause of Mortality.
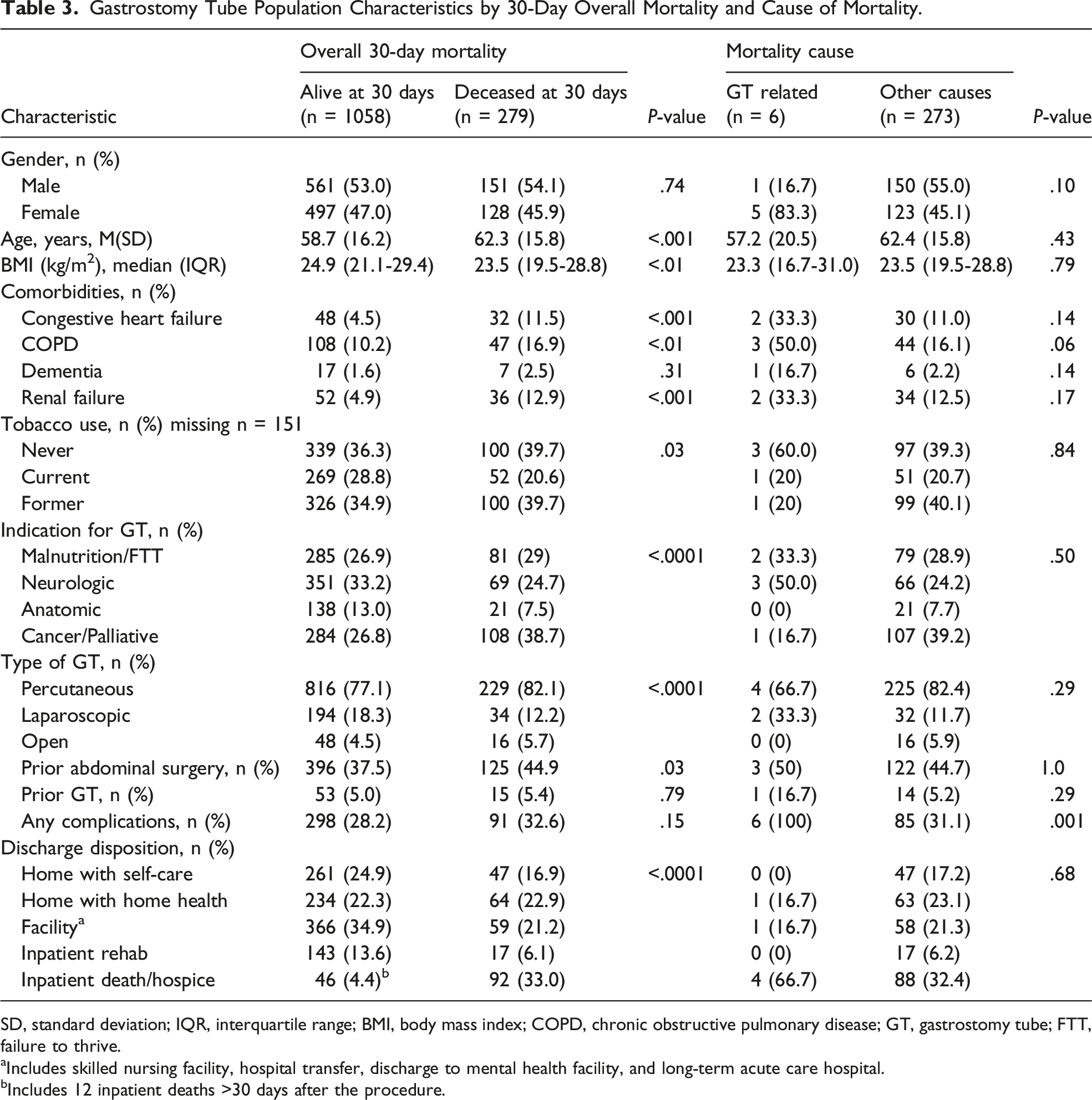
SD, standard deviation; IQR, interquartile range; BMI, body mass index; COPD, chronic obstructive pulmonary disease; GT, gastrostomy tube; FTT, failure to thrive.
aIncludes skilled nursing facility, hospital transfer, discharge to mental health facility, and long-term acute care hospital.
bIncludes 12 inpatient deaths >30 days after the procedure.
When stratified by placement service, there was no difference in GT-related mortality frequency between surgical and non-surgical services (surgical .6% vs non-surgical .5%, P = 1.0). Overall, 30-day mortality was lower among surgical as compared to non-surgical services (16.5% vs 23.7%, respectively, P = .004) (Table 1). While the crude odds of all-cause 30-day mortality were significantly higher among non-surgical services (OR 1.56, 95% CI 1.19, 2.05), there was no difference after adjustment (OR 1.19, 95% CI .83, 1.72) (Table 2).
Patient Characteristics by Placement Service, PEG Placement Only.
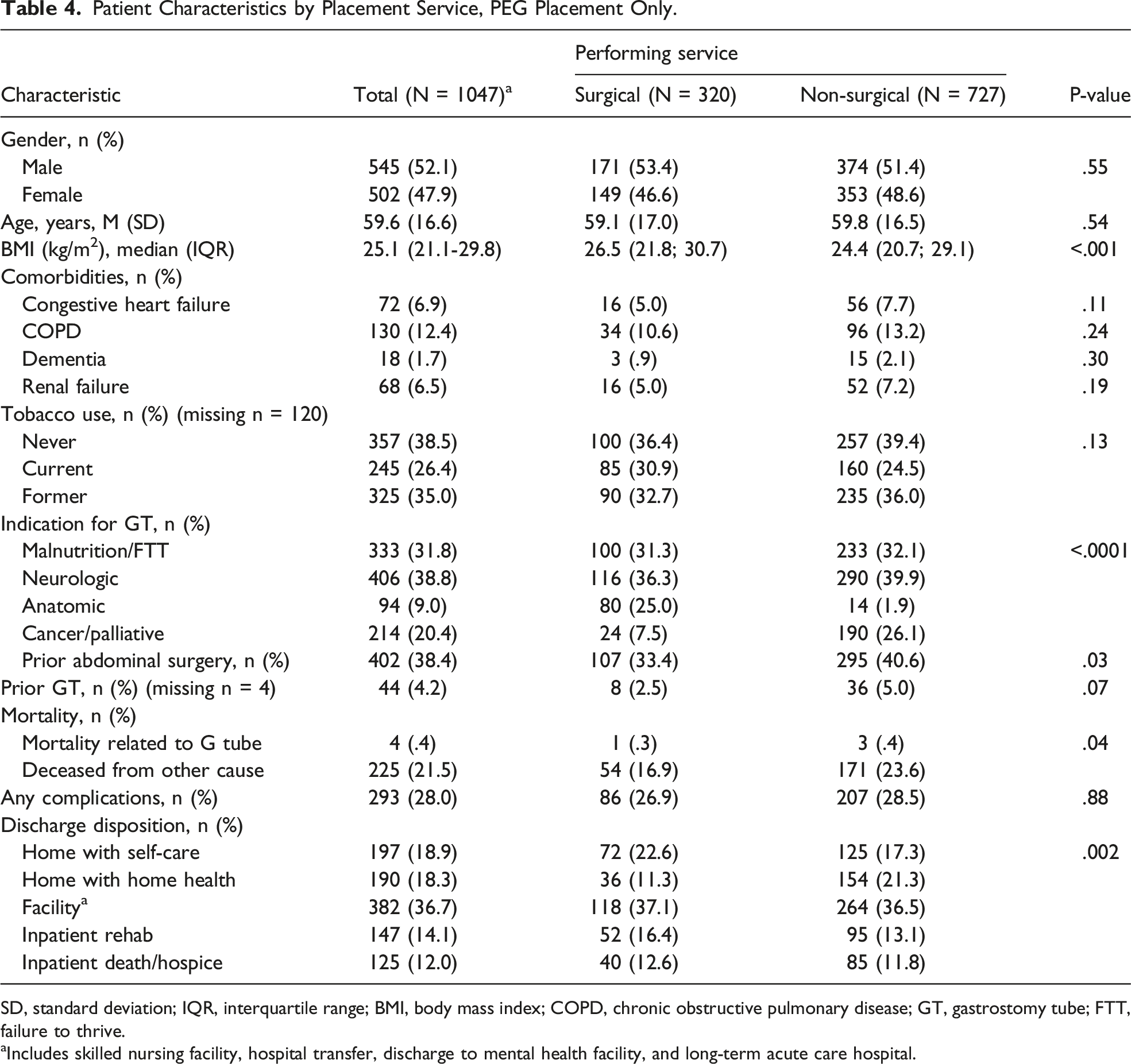
SD, standard deviation; IQR, interquartile range; BMI, body mass index; COPD, chronic obstructive pulmonary disease; GT, gastrostomy tube; FTT, failure to thrive.
aIncludes skilled nursing facility, hospital transfer, discharge to mental health facility, and long-term acute care hospital.
Discussion
In this study, we described outcomes in patients who had GTs placed by surgical vs non-surgical services and demonstrated that these teams had similar complication rates and mortality. All-cause patient mortality was high at 20%, with .5% attributable to GT placement. Although complication rates were similar between services, roughly 1 in 4 patients experienced a complication in our analysis.
To our knowledge, this is the first study examining GT outcomes by surgical or non-surgical placement services. Prior studies of overall complications in GT placement have demonstrated widely variable complication rates between 10 and 88%.6-10 This variation may be due to several factors, including differences in morbidity definitions and study populations. While the data are inconsistent, those with higher rates of complications were older or had more comorbid conditions, particularly cancer or cirrhosis.6,7,10,11
The overall complication rate in this study is within reported ranges. The vast majority of complications were minor mechanical complications such as blockage requiring replacement, pressure injuries, dislodgement, and leakage. Even though these procedures are generally well-tolerated, any complication can lead to infections and the need for further procedures (such as tube studies/exchanges), which can increase hospital length of stay and increase health care costs. These complications, however minor, highlight the need for optimal patient selection.8,12 While close monitoring and education of bedside staff and patients in the initial postoperative phase by procedural team members may help prevent some common complications, this study demonstrates no evidence that the complications are affected by whether a surgical or non-surgical service is placing the GT.
Some data show no differences in complication rates by placement technique. 13 In contrast, an investigation of 91 patients assessing PEG vs laparoscopic vs open placement found significantly lower complications in the PEG and open group compared to the laparoscopic group. 14 While differences in complications between placement techniques may exist in other studies, our data indicate these differences are likely not due to placement service. Even with a more direct comparison of PEGs only, there were still no differences.
Overall mortality after GT placement ranges from 6% to 52%, while GT-specific mortality is lower and ranges from 0% to 2%.9,15-18 Other studies have identified several patient characteristics related to increased 30-day mortality including acute illness, pulmonary cachexia, neurological debilitation, and head and neck cancers.16,19
Consistent with these data, procedural mortality was low, but overall mortality was relatively high in this study. Thirty-day mortality, but not GT-related mortality, was higher in non-surgical services; however, this difference resolved with adjustment, likely accounting for some of the comorbid conditions that were higher among patients receiving GTs by non-surgical services. These findings again highlight the importance of optimal patient selection for these procedures. Additionally, these findings hint at the underlying need for a GT as a harbinger of either frailty or a significantly morbid medical issue that places the patient at risk for mortality.
Not surprisingly, discharge to a skilled nursing facility was common. The frequency of discharge to nursing homes has important implications for discussions with patients and their families in terms of future prognosis and the likelihood of going home. While the presence of a GT itself is unlikely to be the principal reason for these discharge outcomes, if a patient is ill to the point of needing a GT, it may be an indicator of higher short-term mortality and a non-home discharge disposition. Furthermore, patient selection for GT may be problematic as GT is often placed to facilitate discharge from the hospital. Proper patient selection for GT placement is essential, though it is often difficult to anticipate feeding needs in a complicated operative or medical patient. 20
This study has several limitations. This is a single institution study which limits generalizability and statistical power. However, this study included a large sample of patients, the findings are generally consistent with other work, and the indications for GT placement are widely accepted. We did not delineate patients who had an operative GT placement as the primary procedure vs secondarily as part of a larger procedure, nor did we account for other feeding tubes placed simultaneously, such as feeding jejunostomy tubes. This could affect overall 30-day mortality rates, but we also examined GT-specific mortality. Given the retrospective methodology of this study, we cannot account for all possible confounders. Additionally, the degree of post-procedural surveillance, feeding regimens, and tube care was difficult to ascertain in both service types. We did not evaluate the subset of patients who had aborted procedures that subsequently underwent GT placement by another service line; these data may have been relevant given potential increased difficulty and risk of complication in these patients.
Gastrostomy tubes placed by surgical and non-surgical services have equivalent mortality and complication rates. The high overall mortality and complications associated with placement underscore the need for careful patient selection. Patients and families should be aware of the prognostic implications of the need for GT placement, including the potential for a non-home discharge and the fact that patients who require GT often have significant 30-day mortality related to their underlying conditions. Further studies evaluating long-term outcomes are needed to help direct full informed procedural consent and decision-making.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Research Service Award Pre-Doctoral/Post-Doctoral Traineeship from the Agency for Healthcare Research and Quality sponsored by the Cecil G. Sheps Center for Health Services Research, University of North Carolina at Chapel Hill, Grant No. 5T32 HS000032 partially supported Josh Herb.