
Abstract
Background
Feeding difficulties are common in children with cerebral palsy (CP). The goal of this study was to examine pediatric CP patients undergoing gastrostomy tube (G tube) placement and assess the association between patient characteristics and weight after 3 months, 6 months, and 1 year.
Methods
This was a retrospective study of all pediatric patients with CP who received a G tube placement between April 2014 and December 2017 at a single institution. Bivariate analysis was used to examine association between patient characteristics and the primary outcome of improvement in weight Z score at 3, 6, and 12 months.
Results
Of 63 patients who received a G tube, 81% had an increase in Z score at 3 months, 44% at 6 months, and 64% at 12 months. By 12 months, factors associated with a positive Z score change included moderate and severe malnutrition, lack of prior G tube, and fewer comorbidities. The majority (69.8%) of patients experienced complications. Seven (11%) patients died, with only 1 death related to G tube placement.
Discussion
The use of G tubes in CP patients resulted in an increase in an improvement in nutritional status for the majority of patients over the course of a year. Although most complications were minor, patients had a high complication rate and frequently visited the emergency department, highlighting the need for standardized education and follow-up among this patient population.
Key Takeaways
The use of gastrostomy tubes in children with cerebral palsy leads to increased weight gain over 1 year, with patients who are moderately to severely malnourished, who have not had prior gastrostomy tubes, and who have few comorbid conditions benefitting from the most substantial weight gain. Although most complications are minor, the high complication rate makes education and follow-up very important in this population.
Introduction
Cerebral palsy (CP) represents a group of disorders with deficits primarily in motor function with an incidence of 2 per 1000 live births.1-4 Children with CP are at increased risk of developing malnutrition secondary to oral motor and oropharyngeal dysfunction, hypotonia, motility disorders, as well as poor posture due to unstable trunks, leading to feeding difficulties.5-7
Malnutrition, defined as a severe lack of nutrients resulting in decreased body function, affects multiple organ systems and can lead to significant morbidity, mortality, and failure to thrive in this population.8-13 Studies looking at the use of gastrostomy tubes (G tubes) in children with CP have shown that they lead to increased weight gain.6,14-16 However, studies have also shown that there are complications associated with G tubes, with reported complication rates ranging from 4 to 26%.17-19 Some of these complications are minor, such as dislodgement, leakage, and cellulitis, while others can be more serious, such as bleeding, abscesses, peritonitis, organ injury, and even death.10,20,21
Currently, there are no studies evaluating CP patient characteristics that are associated with successful weight gain in G tubes. Likewise, there are no studies assessing which patient characteristics are associated with complications in G tubes. Ideally, determining these factors would help optimize weight gain and identify patients that are at high risk for complications in order to mitigate that risk. The goal of this study was to examine pediatric CP patients undergoing G tube placement and assess the association between patient characteristics and weight after 3 months, 6 months, and 1 year. Additionally, the study evaluated characteristics associated with complications and mortality in G tube placement.
Methods
This study was approved by the University of North Carolina-Chapel Hill Institutional Review Board. This was a retrospective chart review of all pediatric patients (<18 years) with CP who underwent G tube placement between April 2014 and December 2017 at a single tertiary care institution, with at least 1-year follow-up post-placement. Baseline demographic was collected, as were any use of nasogastric (NG) tube for nutritional support (excluding decompression), length of time of NG tube use in days, and prior G tube placement. Prior G tube placement was defined as a one being placed and removed at any point prior to the study time. Malnutrition status was determined using weight-for-age Z scores. Patients were categorized as mild if Z score was < −1, moderate if Z score was −2 to −3, and severe if Z score was <−3 22 If weight-for-age Z scores were not available on patient charts, they were determined using the Center for Disease Control weight-for-age percentiles calculator, which is the calculator used by our electronic medical record. Comorbidities were classified into categories including cognitive/developmental delay, seizures/epilepsy, cancer, kidney disease, liver disease, heart disease, lung disease, pre-existing reflux, and other digestive disease based on chart documentation. We did not have data on height, skin-fold measurements, mid-upper arm circumference, or Gross Motor Function Classification System.
The primary outcome was weight gain at 3 months, 6 months, and 12 months post-G tube placement. Weight gain was measured by change in Z score from baseline to 3 months, 3 months to 6 months, and 6 months to 12 months and recorded as a decreased/stable or increased change. Secondary outcomes included mortality and complications. Cause of death and whether or not the death was related to G tube placement were recorded. Complications were broken down into functional bowel problems, aspiration/pneumonia, functional tube problems, nutritional abnormalities, infection, major complications, gastrocutaneous fistula, and bleeding. Functional tube problems included dislodgement, clogging, pressure wounds, leakage, and issues with locking in place. As functional tube problems are generally minor problems but are common, chart review determined whether these issues required a telephone call, clinic visit, emergency department (ED) visit, or admission.
Functional bowel problems included diarrhea, constipation, and gastroesophageal reflux (GERD). As these are common issues in CP patients, in order for the complication to be attributed to the G tube, the causality had to be specifically mentioned in patient notes and 2 reviewers evaluated each complication. Nutritional abnormalities mentioned in the notes included hyperglycemia and electrolyte imbalances related to feeds. Infection was defined as cellulitis or abscess around the G tube site that required medical treatment with a procedure or antibiotics. Major complications included reoperation, specifically, necrotizing soft tissue infections, peritonitis, and organ injury related to G tube placement. Bleeding was defined as any bleeding around the site requiring direct medical attention via clinic visit, ED visit, or admission.
Statistical analysis was conducted using Stata/MP (version 12) (Stata Corp, College Station, TX). Patient demographics, stratified by weight gain, complication, and mortality were compared using chi-squared and Fisher’s exact tests, where appropriate. A P-value <.05 was considered significant.
Results
Baseline Characteristics of Patients with Cerebral Palsy Undergoing Gastrostomy.
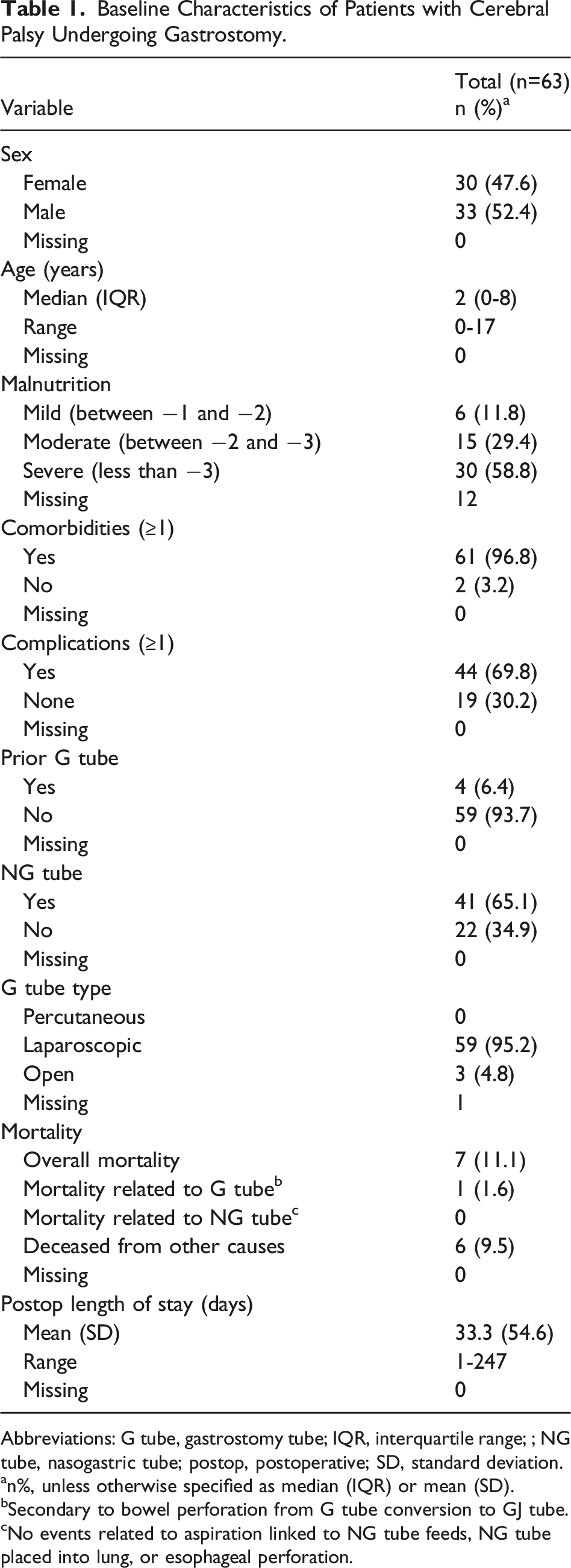
Abbreviations: G tube, gastrostomy tube; IQR, interquartile range; ; NG tube, nasogastric tube; postop, postoperative; SD, standard deviation.
an%, unless otherwise specified as median (IQR) or mean (SD).
bSecondary to bowel perforation from G tube conversion to GJ tube.
cNo events related to aspiration linked to NG tube feeds, NG tube placed into lung, or esophageal perforation.
Fifty-nine (95.2%) patients underwent laparoscopic G tube placement, while 3 (4.8%) had open placement because of adhesions from prior operations. As summarized in Table 1, 69.8% (n = 44) of patients experienced one or more complications. Functional tube problems were the most common complication among 68.3% (n = 43) of patients. Among patients with functional G tube complications, 9.3% (4/43) had families that were able to use only a phone call to solve the issue, while 18.6% (8/43) were able to address the problem at home. However, 55.8% (24/43) of patients required a clinic visit specifically to deal with the issue, while 27.9% (12/43) patients required ER visits and 23.3% (10/43) patients required admission specifically for the functional issue (some patients had multiple admissions.)
Twenty-two percent (n = 14) of patients experienced functional bowel problems, such as diarrhea, constipation, and GERD. Pulmonary aspiration or PNA were present in 4.76% (n = 3) of patients; infections relating to cellulitis, abscess, and necrotizing soft tissue infections were present in 6.3% (n = 4); and bleeding in 4.8% (n = 3). There was one (1.6%) reported major complication relating to organ injury. There was no significant difference in baseline characteristics or diagnosis among patients who had experienced at least one complication vs those who had no complications.
Patient Characteristics by Complication.
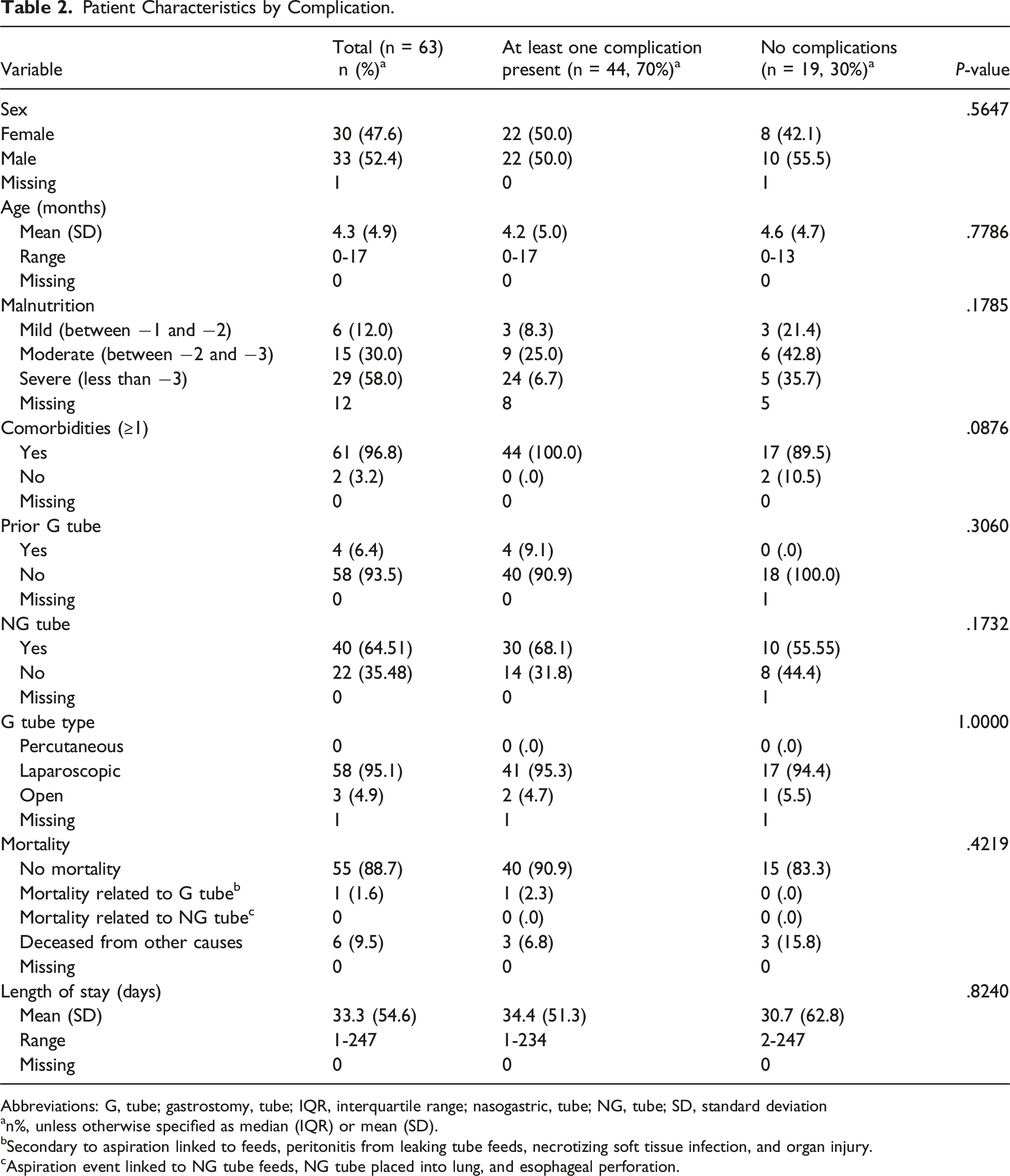
Abbreviations: G, tube; gastrostomy, tube; IQR, interquartile range; nasogastric, tube; NG, tube; SD, standard deviation
an%, unless otherwise specified as median (IQR) or mean (SD).
bSecondary to aspiration linked to feeds, peritonitis from leaking tube feeds, necrotizing soft tissue infection, and organ injury.
cAspiration event linked to NG tube feeds, NG tube placed into lung, and esophageal perforation.
Patient Characteristics by Mortality.
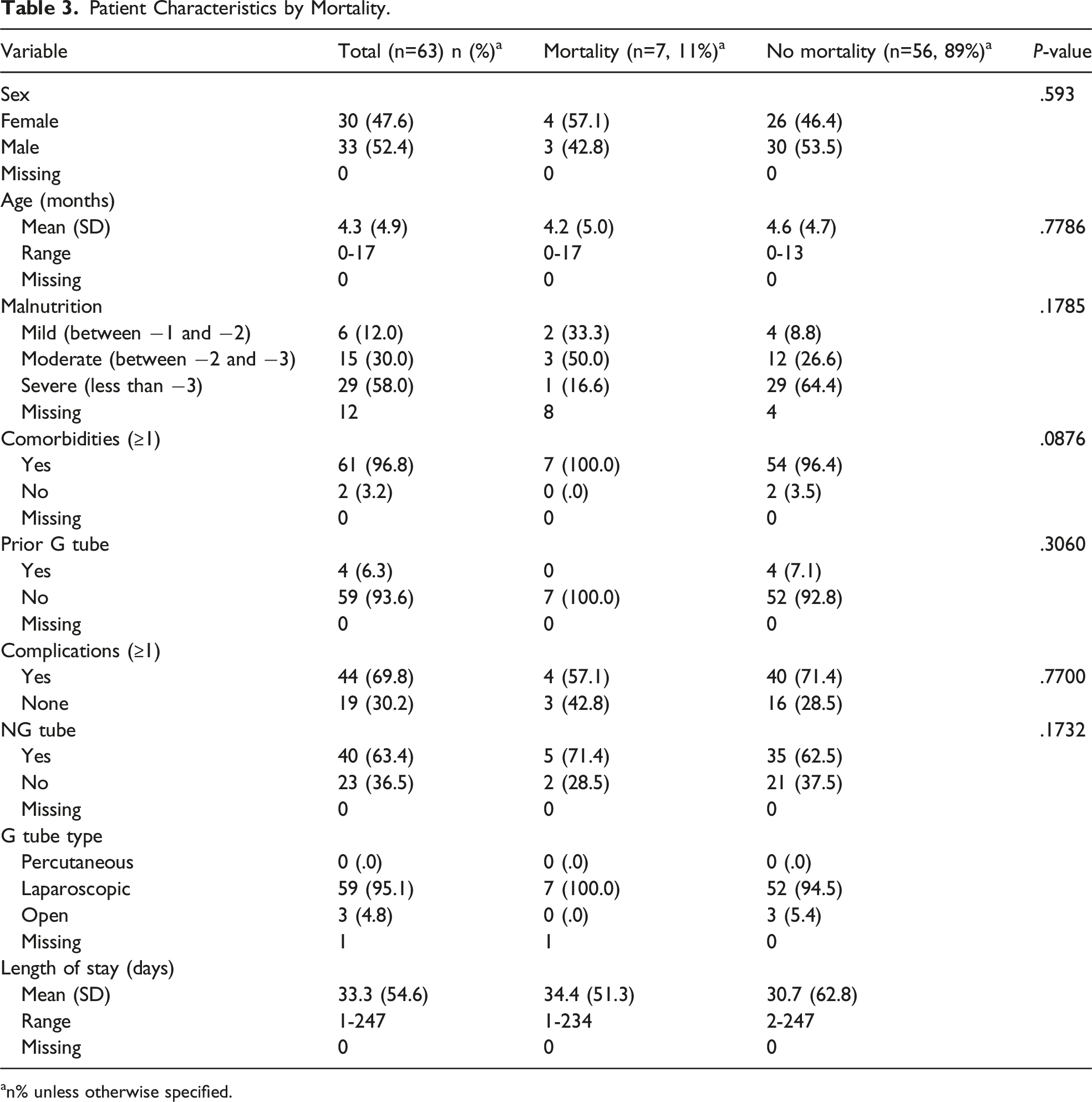
an% unless otherwise specified.
Change in Z Score by Patient Characteristics at 3, 6, and 12 Months.
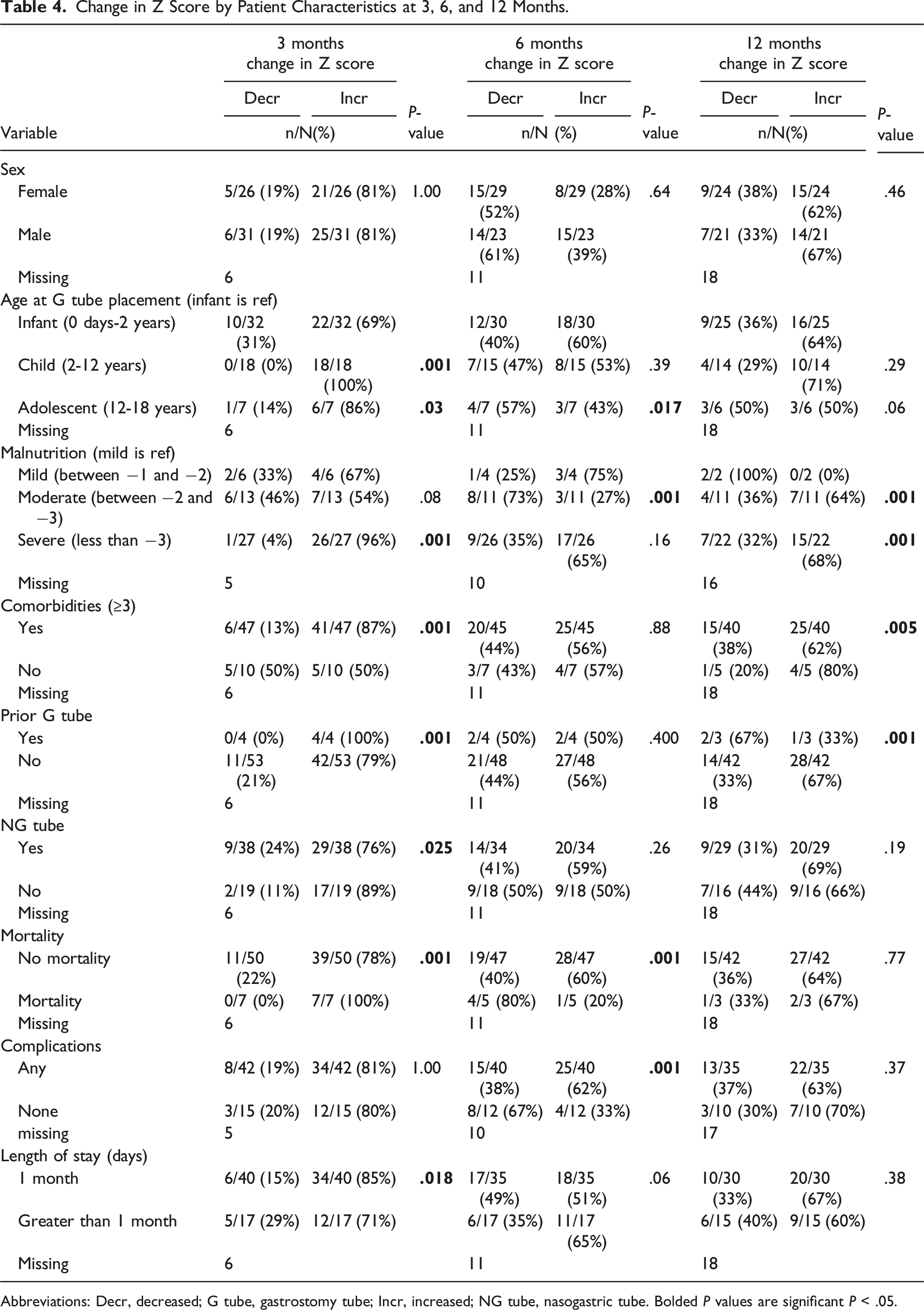
Abbreviations: Decr, decreased; G tube, gastrostomy tube; Incr, increased; NG tube, nasogastric tube. Bolded P values are significant P < .05.
Discussion
Similar to previous studies, G tube feeding was associated with increases in weight gain over time in CP patients.1,6,14-16,23,25 We noted that patient characteristics associated with improved Z score changes varied over the 3, 6, and 12 months post-gastrostomy placement period. Initially at 3 months, older patients with more comorbidities, prior G tubes, and longer LOS were more likely to have positive Z score changes. At 12 months, however, factors such as LOS became less important, as 1 might expect further out from hospitalization. At 12 months, fewer comorbid conditions led to greater weight gain. While patients with more comorbid conditions may have benefited early on from G tube placement, their comorbid conditions may have led to issues maintaining that weight gain at 12 months. Unsurprisingly, patients with malnutrition seemed to gain the most benefit in terms of Z score change at 3, 6, and 12 months. Surprisingly, patients who had NG tube supplementation did not appear to have higher growth rates; this may have been secondary to length of supplementation or the fact that all patients received G tubes and thus were achieving optimal nutrition over the course of the year.
Although the majority of complications were minor in nature with only 1 death related to GJ conversion, the overall rate of complications was high, with almost 70% of patients having some issue related to their G tubes. Past studies have also shown a low rate of serious complications from 4 to 26% with minor complications being more frequent.17,18,24,26,27 A 2004 systematic review found that the proportion of patients with minor complications can be as high as 95%. 6 Variation in complication rate may be affected by differences in definitions and diverse study populations, as well as presence or absence of standardization of care. Possibly due to the sample size and the high percentage of complications, we were unable to find any significant associations between patient characteristics and complications.
The most common complications were functional tube problems such as tube clogging, dislodgement, pressure wound, and leakage. While these concerns are minor, very few families were able to deal with the problem over the phone or at home. Over 50% of the patients required an ER visit or admission to address the complication during the span of 1 year. A recent study looking at 30-day ER visits and readmissions after G tube placement in the United States revealed that 8.6% of children visit the ER and 3.9% are readmitted, most commonly secondary to infection, mechanical complications, and dislodgement. 28 Another recent study showed that a quarter of the patients are responsible for the majority (82%) of ER visits, with non-Caucasian patients at higher risk, highlighting the need for a larger cohort or prospective database of patients to identify further characteristics of high-risk patients and to begin to mitigate risk and disparities. 29
In the face of rising health care costs, the use of resources and financial strain on both the family and the health system should be considered. One study evaluating hospital resource utilization found a decrease in utilization after implementation of a standardized feeding device placement pathway. 30 Another study interviewed surgeons and nurses routinely involved in G tube care at high performing institutions demonstrated that common themes among hospitals with favorable outcomes included family education, provider availability, and family empowerment. 31 Protocols, support systems, and written materials may help to reduce ER visits, and other options such as walk-in clinics and improved 24-hour access to providers could help to alleviate these issues.
Approximately a third of patients had functional bowel issues including diarrhea, constipation, and reflux. The degree to which these problems were related to enteral feeds via G tubes vs the underlying disease process was difficult to delineate. Gastroesophageal reflux is very common among infants, though the majority tend to outgrow it. In CP patients, GERD is found in approximately 15-77% of this population.32-34 Even among 3-month old typical children, GERD can be present 50% of the time, with the percentage of children affected gradually decreasing over time. 35 If the complication of functional bowel issues is removed, 68.3% of patients still had a complication, as the majority of patients had more than one complication. Of note, historically concomitant Nissen fundoplication was performed in many children with CP because of the high rates of GERD. Many centers like ours have moved away from performing Nissens, particularly given growing evidence that the Nissens do not decrease readmissions for GERD and have been associated with the need for additional operations. 36 This study underscores the success of G tubes in nutritional rehabilitation and supports the avoidance of anti-reflux surgery in this population.
The greatest limitation of this study was the small sample size; thus, we were unable to demonstrate significant associations or perform meaningful modeling. The specificity of the subpopulation studied in addition to the inclusion criteria requiring the patient to receive regular follow-up for at least a year greatly limited the number of patients. Missing weights at follow-up and missing nutritional information limit the study as well. When comparing this sample size to other single institution studies on the topic, it is noted that the sample sizes are similar. This was a single institution study, reducing the generalizability. The investigators had to rely on documentation, which may have errors or missing values.
In conclusion, this retrospective study looking at the use of G tubes in pediatric CP patients demonstrated good weight gain, particularly among patients with moderate to severe malnutrition. The overall ease of use of G tubes and the benefits of weight gain do outweigh the complications faced by these patients, given that major complications were rare. Parents should be aware that patients will require close follow-up and easy access to providers as they grow, as there is a high likelihood of minor complications.
Footnotes
Acknowledgments
We would like to acknowledge the Carolina Medical School Research Program for supporting Jihane Jadi during her summer research project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The study complies with ethical standards and was reviewed and granted exemption by the UNC IRB in view of the retrospective nature of the study and all the procedures performed were part of the routine care. IRB# 17-3075.