
Abstract
While early gastrostomy tube placement (GTP) may decrease hospital length of stay and facilitate disposition, GTP may be unnecessary as some patients regain the ability to eat earlier than expected. No guidelines currently exist regarding optimal GTP timing or minimum duration of need indicating appropriateness of GTP. This retrospective (9/2017-12/2019) single center study evaluated the incidence of adequate (>75%) oral caloric intake (ACI) after GTP during index hospitalization and associated characteristics before discharge. Bivariate analyses were performed to compare patients achieving ACI and patients not achieving ACI at discharge. By discharge, 10 (12.5%) patients achieved ACI and 6 (7.5%) had their GT removed prior to discharge suggesting many patients undergo unnecessary GTP. Also, 6 (7.5%) patients suffered GTP-related complications. Future multicenter studies are needed to corroborate these findings and establish GTP guidelines for trauma patients to avoid unnecessary GT procedures and associated morbidities.
Keywords
Gastrostomy tube placement (GTP) is most commonly used for patients with neurological diseases, cancer, and traumatic injuries such as traumatic brain injury (TBI). Gastrostomy placement is well established as a treatment for prolonged or permanent dysphagia to ensure adequate enteral nutrition. Though nutritional optimization is crucial for acute management of patients with TBI, the recovery following TBI and the resumption of oral intake after GTP is variable and difficult to predict. 1
Currently there are no well-established or widely used guidelines to help providers determine the optimal timing for placement of gastrostomy tubes for trauma patients. From the authors’ experience, there may be a population of trauma patients that are able to resume oral intake prior to discharge. This may be due to prolonged hospital stay or more expeditious than expected convalescence. Regardless, this suggests some patients receive an unnecessary surgical intervention, which poses risk of gastrostomy-related complications including gastrointestinal bleeding, infection, peritonitis, dislodgment, fistula, and hollow viscus perforation. 2 Therefore, this study sought to determine the rate of trauma patients who received GTP but achieved adequate (>75%) oral caloric intake (ACI) prior to discharge. If substantial, this would suggest a need to further refine criteria for GTP in trauma patients.
This study was approved and deemed exempt by the Institutional Review Board, and a waiver of informed consent was granted. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. All adult (>18 years-old) trauma patients at a single Level-I trauma center between September 2017 and December 2019 (prior to the SARS-CoV-2 pandemic) who underwent GTP were included. Patients who underwent gastrostomy placement via the following methods were included: interventional radiology (IR), percutaneous endoscopic gastrostomy (PEG), and laparoscopic assisted or open surgery. Patients who died before discharge or were younger than 18 years old, pregnant, or incarcerated were excluded.
The primary outcome was achieving ACI at discharge. Patients who achieved ACI were compared to patients who did not achieve ACI. Demographics, comorbidities, injury profile, discharge disposition, complications, Glasgow Coma Scale score, Rancho Los Amigos scores, and procedures done during hospitalization were recorded. To test for the association of patient demographics and clinical characteristics with the outcome of achieving ACI, bivariate analyses were performed with categorical variables using chi-square tests, and continuous variables using Mann-Whitney U tests due to their skewed distributions. Two-tailed P-values were calculated and P-values less than alpha = .05 were considered statistically significant. Analyses were performed using Stata (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC).
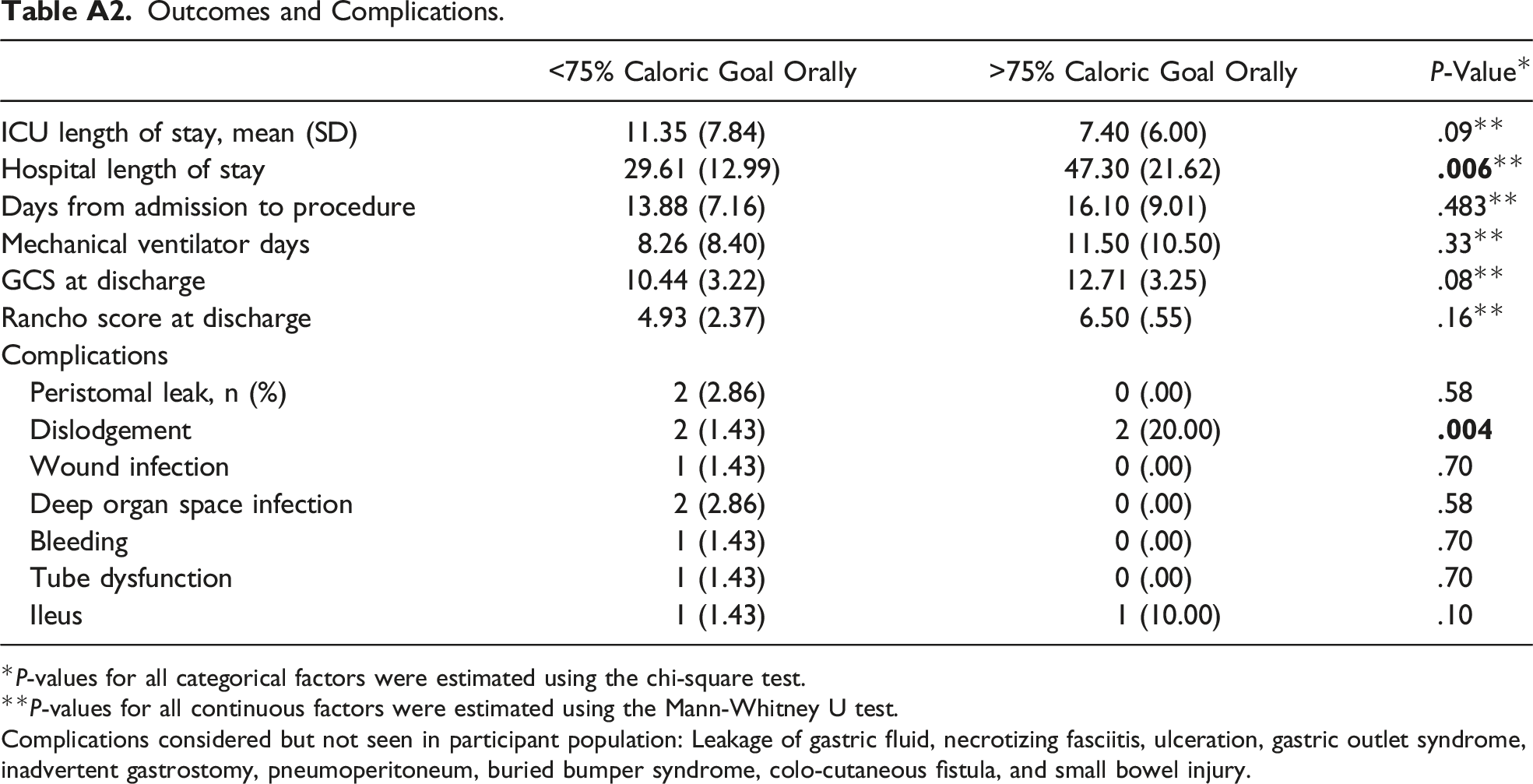
A total of 80 patients (.84% of all trauma patients) underwent GTP. There was no difference between cohorts regarding demographics and insurance status (Table A1). At discharge, 22 (27.5%) patients tolerated some ACI, with 10 patients (12.5%) achieving ACI by discharge. An additional 2 patients (total of 12 patients) achieved at least 50% of caloric intake goal. Furthermore, 6 (7.5%) patients had their gastrostomy tube removed before discharge and an additional 6 patients (7.5%) suffered at least one GTP-related complication including dislodgment, wound infection, deep organ space infection, tube dysfunction, and ileus (Table A2). Of the 80 participants, 4 (5%) had a gastrostomy tube dislodgment complication associated with the procedure. Interestingly, ACI patients had an increased rate of tube dislodgement (ACI: 20.0%, non-ACI: 1.43%, P = .004) compared to non-ACI patients (Table A2). All other complications were similar between cohorts (all P > .05). Also, ACI patients had increased length of stay compared to those not achieving ACI (47.3 days vs 29.6 days, P = .006) (Table A2).
This retrospective study found that over 12% of trauma patients who underwent GTP achieved ACI by time of discharge. In addition, nearly 8% suffered a gastrostomy related complication during index hospitalization. A third of these patients who suffered a complication were able to achieve ACI prior to discharge and thus represent potentially avoidable complications.
Improvement of dysphagia is not uncommon after traumatic injury. In fact, Ward et al found that 75% of 117 patients who suffered TBI requiring speech pathology intervention for dysphagia commenced oral intake by 17 days with nearly 50% returning to normal diet by 3 weeks. 3 In support, more than 12% of this current single center study population achieved ACI before discharge from the hospital suggesting concern for patient selection or premature performance of GTP.
This study found the hospital length of stay was significantly longer for patients achieving ACI. The longer duration of stay was likely valuable for the recovery of swallowing function. Also, the group not achieving ACI by discharge had a relatively increased number of additional procedural interventions compared to the group achieving ACI. The addition of more surgical interventions often leads to slower recovery and more complications. 2 The ability to predict length of stay and relative severity of injury that would require multiple procedures might be helpful in creating a guide for optimal timing of GTP.
While the technical performance of a gastrostomy tube may not be challenging, these procedures carry significant risk. Prior studies have demonstrated the risk of morbidity associated with a minimally invasive GTP (eg, PEG) to be as high as 26.2%. 1 This study found a complication rate of nearly 8%. Additionally, a recent study found that surgical feeding tubes have been associated with a 3 times higher rate of in-hospital adverse events than with natural orifice (nasal or oral) feeding. 4 Given this significant morbidity associated with patients receiving gastrostomy tubes, it is important for all health care providers to recognize that while common, GTP is not benign.
There are several limitations to this study. First, the limitations of sample size and the retrospective design result in a lack of generalizability and inability to establish causal relationships between potential predictors and early return to ACI. Furthermore, as there are no current established guidelines or benchmarks for what is considered ACI, our use of 75% of caloric intake goal was chosen based of the American Society of Parenteral and Enteral Nutrition guideline for weaning off total parental nutrition. In addition, while some patients were found to likely not require GTP, this study does not record what complications of temporary nasoenteral tube feeds they might have endured instead.
This single center study of trauma patients who had GTP demonstrated over 12% achieved ACI during index hospitalization. Patients who achieved ACI, especially patients who had their gastrostomy tube removed before discharge, likely did not need GTP and the associated risks. This demonstrates a need to identify predictive factors for requiring long-term enteral access and GTP to improve patient selection. To achieve this goal, prospective multicenter studies are likely needed to develop guidelines for early GTP in trauma patients. Additionally, future studies should follow patients post hospital discharge to fully understand the need for GTP and/or long-term complications in this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
Demographics of Adult Trauma Patients Who Underwent Gastrostomy Tube Placement. *P-values for all categorical factors were estimated using the chi-square test. **P-values for all continuous factors were estimated using the Mann-Whitney U test. Outcomes and Complications. *P-values for all categorical factors were estimated using the chi-square test. **P-values for all continuous factors were estimated using the Mann-Whitney U test. Complications considered but not seen in participant population: Leakage of gastric fluid, necrotizing fasciitis, ulceration, gastric outlet syndrome, inadvertent gastrostomy, pneumoperitoneum, buried bumper syndrome, colo-cutaneous fistula, and small bowel injury.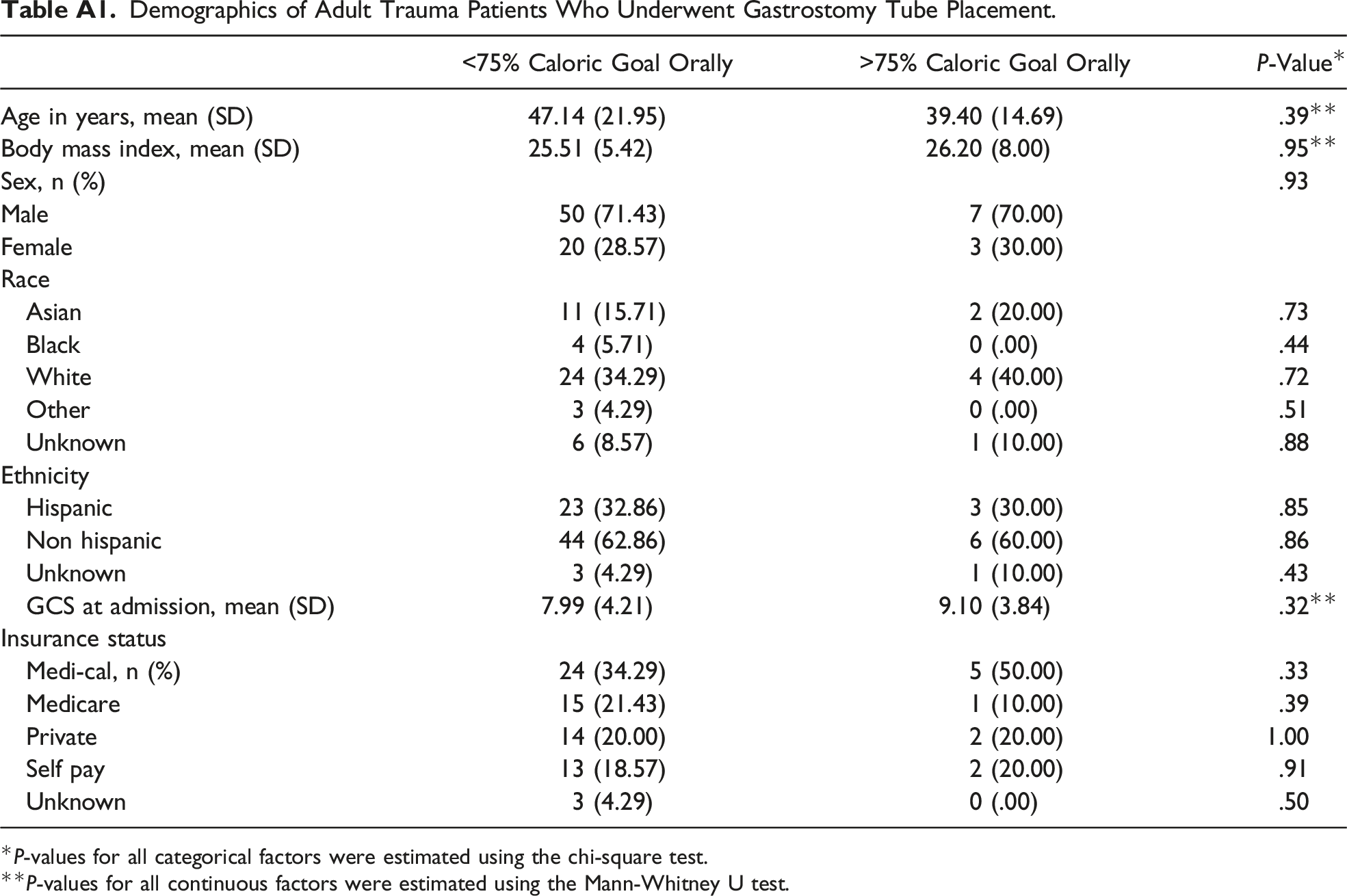
<75% Caloric Goal Orally
>75% Caloric Goal Orally
P-Value*
Age in years, mean (SD)
47.14 (21.95)
39.40 (14.69)
.39**
Body mass index, mean (SD)
25.51 (5.42)
26.20 (8.00)
.95**
Sex, n (%)
.93
Male
50 (71.43)
7 (70.00)
Female
20 (28.57)
3 (30.00)
Race
Asian
11 (15.71)
2 (20.00)
.73
Black
4 (5.71)
0 (.00)
.44
White
24 (34.29)
4 (40.00)
.72
Other
3 (4.29)
0 (.00)
.51
Unknown
6 (8.57)
1 (10.00)
.88
Ethnicity
Hispanic
23 (32.86)
3 (30.00)
.85
Non hispanic
44 (62.86)
6 (60.00)
.86
Unknown
3 (4.29)
1 (10.00)
.43
GCS at admission, mean (SD)
7.99 (4.21)
9.10 (3.84)
.32**
Insurance status
Medi-cal, n (%)
24 (34.29)
5 (50.00)
.33
Medicare
15 (21.43)
1 (10.00)
.39
Private
14 (20.00)
2 (20.00)
1.00
Self pay
13 (18.57)
2 (20.00)
.91
Unknown
3 (4.29)
0 (.00)
.50
<75% Caloric Goal Orally
>75% Caloric Goal Orally
P-Value*
ICU length of stay, mean (SD)
11.35 (7.84)
7.40 (6.00)
.09**
Hospital length of stay
29.61 (12.99)
47.30 (21.62)
Days from admission to procedure
13.88 (7.16)
16.10 (9.01)
.483**
Mechanical ventilator days
8.26 (8.40)
11.50 (10.50)
.33**
GCS at discharge
10.44 (3.22)
12.71 (3.25)
.08**
Rancho score at discharge
4.93 (2.37)
6.50 (.55)
.16**
Complications
Peristomal leak, n (%)
2 (2.86)
0 (.00)
.58
Dislodgement
2 (1.43)
2 (20.00)
Wound infection
1 (1.43)
0 (.00)
.70
Deep organ space infection
2 (2.86)
0 (.00)
.58
Bleeding
1 (1.43)
0 (.00)
.70
Tube dysfunction
1 (1.43)
0 (.00)
.70
Ileus
1 (1.43)
1 (10.00)
.10