
Abstract
The paper proposes an optimization model for the allocation of vaccines to a heterogeneous population composed of several subpopulations with different sizes and epidemiological disease transmission parameters. As the objective, an aggregated function combining a standard utilitarian efficiency criterion with a Gini index–related penalty term is considered. Contrary to previous work, we adopt an outcome equity view: The inequity measure is not based on vaccination fractions or other input factors, but on the fractions of individuals escaping infection, as predicted by an susceptible‐infectious‐removed (SIR) model. An adjusted pro rata (APR) policy of vaccine allocation minimizing inequity in this outcome view is introduced, and a numerical procedure for its determination is presented. The concepts are developed both for the case of segregated subpopulations and for that of interactions between the subpopulations. Interestingly, in a large number of instances, the optimal solution under the aggregated objective function turns out to be identical to APR. Whether APR is locally or even globally optimal in a concrete case depends on the relation of an inequity aversion parameter to certain threshold values. While the local optimality threshold can be determined by linear programming, the determination of the global optimality threshold, as the vaccine allocation problem itself, is a problem of nonconvex optimization. We suggest an exact optimization approach for smaller instances, and propose algorithms building on particle swarm optimization for threshold determination and allocation optimization at larger instances. Extensions to alternative outcome measures such as the number of fatalities are presented as well. In addition to the investigation of randomly generated instances, two test cases from the literature are revisited in the context of the present work. Moreover, a new case study based on data from the COVID‐19 outbreak in Austria in 2020 is introduced and analyzed.
INTRODUCTION
The recent worldwide COVID‐19 crisis showed not only the importance of vaccination as a main instrument to mitigate the effect of a pandemic, but also the difficulties in deploying this instrument in an effective way. A main issue in this context is vaccine availability. Due to the limitations in vaccine production and also due to prices that may overwhelm the financial resources of poorer countries, the case where a high demand of vaccine meets a scarce supply is, unfortunately, not rare.
Some articles (for an example, see Keeling & Shattock, 2012) addressed the problem of minimizing the overall size of an epidemic by vaccine allocation under insufficient supply, but admitted that the resulting solution can be highly inequitable and may therefore not be accepted by the society. It has been stated that in the vaccine allocation literature, a reconciliation between equity and efficiency is missing (Duijzer et al., 2018). This paper aims at overcoming this gap by applying, as the objective function for a proposed optimization model, a social welfare function that combines efficiency with equity, a so‐called “inequity‐averse aggregation function” (IAAF) (see Karsu & Morton, 2015).
The envisaged scenario is prophylactic vaccination of a heterogeneous overall population. A model with multiple subpopulations (patches) is used. We start with the situation where the subpopulations are noninteracting (e.g., spatially segregated) in order to obtain a basic insight into the influence of vaccination policies, and relax this assumption then to the case of interaction.
Contrary to some previous works that considered fairness in their vaccine allocation models, usually in the form of equity constraints, this paper aims at health outcome equity rather than at input equity. As to the distinction between these two notions, see Pressman et al. (2021). In our context, the focus on outcome equity means that the ideal state with respect to fairness is not that every person has the same probability of getting vaccinated, no matter whether in their environment, the infection risk is vast or minimal, but rather that everybody has the same chance of not being infected (or, alternatively, of not needing hospitalization, or of not dying from the disease, etc.).
To make the motivation for using outcome equity quite clear, let us take the case of breast cancer as an example. It is well known that this disease primarily affects women, with a lifetime incidence rate of roughly 1/8. In rare cases, also men can be affected; however, their lifetime incidence rate is only about 1/800. Suppose now that a vaccine that permanently protects against breast cancer will be developed in the future, and 10 million doses of this vaccine will be available in a country with 20 million inhabitants, half of whom are women. The solution maximizing input equity would allocate 5 million doses to women (subpopulation 1) and 5 million doses to men (subpopulation 2). As a result, ≈625, 000 women, but only ≈6250 men would still get the disease.
It may be doubted that this is a perfectly fair allocation: Why should it be fair to spend half of the available scarce resource for further improvements in a subpopulation that is much better off anyway with respect to the considered disease? Most healthcare decision makers (DMs) would probably tend in this situation to focus the resource allocation on that subpopulation that more urgently needs it. Short calculation shows that by spending a share of 100/101 on the female group and only a share of 1/101 on the male group, perfect outcome equity is achieved: In both subpopulations, the number of people still getting the disease would be about the same, namely ≈12, 400. This paper adopts the described outcome equity view without claiming that it is the ultimate solution to the difficult fairness quantification problem.
Our basic model follows that in Duijzer et al. (2018), but extends it by the outcome equity feature and by a more explicit consideration of the case of interaction between the patches. Moreover, we assume that the given stockpile of the vaccine is available already before or immediately after the onset of the epidemic outbreak, and that no later replenishment by new supply will take place. This assumption, made in several publications before, opens ample opportunities for generalizations in future research.
As the social welfare function, we employ a linear combination of average benefit and Gini's mean absolute difference of benefits. This measure, termed Gini aggregation function (GAF) in the sequel, is well founded in theory: It is characterized by a set of axioms and has been shown to be a natural extension of the Gini index, the possibly most prominent equity measure in the economic literature, to the simultaneous consideration of equity and efficiency (see Argyris et al., 2022; Porath & Gilboa, 1994). The weight given to the Gini term is an inequity aversion parameter, which can be interpreted and elicited.
In addition to the mentioned Gini‐based measure, we shall also investigate the simpler Rawlsian IAAF, which takes the outcome of the worst‐off individual as its evaluation criterion. It will be shown that the optimal solution under the Rawlsian IAAF typically coincides with a suitable modification of the simple pro rata (PR) vaccine allocation, the allocation applying the same vaccination fraction in each subpopulation. A main topic of our investigation will be when this modification, called adjusted pro rata (APR) allocation in the sequel, is locally or globally optimal under the GAF measure. We answer the question of local optimality by linear programming approach. The question of global optimality is more difficult to address, because it amounts to the solution of a nonconvex optimization problem, which we tackle by using the particle swarm optimization (PSO) metaheuristic.
Surprisingly, it turns out that for regional partition into subpopulations, without or with interaction, APR is typically even globally optimal for a large range of the inequity aversion parameter. Thus, for applications to geographical clusters, a recommendation of using APR can be given independently of the precise degree of inequity aversion, which may vary among DMs, as long as the DMs at least agree on a certain problem‐specific (usually small) minimum weight they are willing to give to the equity objective. For partition into age groups, this conclusion cannot be drawn anymore. We shall also address the case where instead of the number of infected individuals, the number of fatalities is the considered outcome quantity. Again, differences between regional and age‐based stratification can be observed.
Summarizing, the main contributions of this work are the following: A fairness model for vaccine allocation in a pandemic is developed, based on the notion of outcome equity instead of input equity. An objective function aggregating fairness and efficiency by means of the generalized Gini index is proposed, and the resulting optimization problem is analyzed within the context of a multipatch epidemiological model, both without and with interactions between the patches. An APR allocation of vaccine is defined and shown to be a suitable choice especially in typical situations of a geographical segregation of the patches (subpopulations). A new case study referring to the first phase of the COVID‐19 pandemic in Austria is introduced.
The paper is organized as follows: Section 2 shortly reviews related literature. Section 3 introduces the investigated vaccine allocation problem by deriving it from the epidemiological SIR model on the one hand and quantitative approaches to handle the equity issue in optimization on the other hand. In this context, also the APR vaccine allocation is defined. In Section 4, some analytical insights into the structure of the problem are presented. Section 5 deals with numerical methods for solving the problem under consideration. Section 6 extends the multipatch model to the case of interactions between the patches, while Section 7 generalizes it to limited vaccine efficacy and to patch‐specific weights. In Section 8, three case studies are provided. Section 9 discusses the results and limitations of the paper from the viewpoint of application, and Section 10 concludes the paper.
RELATED LITERATURE
There is a broad literature on quantitative approaches to optimal vaccine allocation based on suitable epidemiological models. For general introductions to epidemic modeling, see, for example, Brauer et al. (2019) and Daley and Gani (2001). Let us focus on those papers that are most relevant in the context of this paper, and outline their relations to the latter.
Hill and Longini Jr (2003) deal with the question, which vaccination fractions in a heterogeneous population composed of a certain number of groups are suitable in order to eliminate the possibility of an epidemic in the whole population (in other words, in order to keep the reproduction number below 1). After describing the threshold surface of critical vaccine allocations, they address the optimization problem of minimizing the total required number of vaccinations while remaining at threshold level.
A starting point for this investigation is Keeling and Shattock (2012). The authors ask for the optimal distribution of vaccine over spatially segregated subpopulations without or with interaction in the case of limited supply. They build their model on the classical final epidemic size formula by Kermack and McKendrick (1927), extended to the situation where the total population consists of several subgroups. It is shown that the distribution minimizing the total number of cases depends heavily on the size of the given stockpile. Some of these distribution policies are rather extreme insofar as they drastically advantage certain subgroups at the cost of other subgroups, which, as the authors admit, might be considered unethical.
Duijzer et al. (2016) define two vaccine allocation problems for multiple populations: (i) Find the vaccine allocations to subpopulations that maximizes the herd effect, that is, the number of individuals who escape infection without being vaccinated themselves. (ii) Find that critical vaccination coverage, that is, that vaccine allocation entailing a reproduction number of 1 in the whole population, that needs the least amount of vaccines. The authors show that problems (i) and (ii) are actually equivalent to each other, and provide an efficient algorithm (and for special cases even analytic solutions) for them.
For a sudden epidemic outbreak in a population partitioned in regional subgroups, Duijzer et al. (2018) address the problem of determining the optimal allocation of a vaccine stockpile that is insufficient to vaccinate the entire population. The focus of the work is on a situation without interaction between the subgroups, but also the case of interaction is touched. The authors identify a convex–concave property and other characteristics of the function quantifying the herd effect, elaborate on the role of the dose‐optimal vaccination fraction, and derive a simple heuristic for the vaccine allocation problem. Similarly as Keeling and Shattock (2012), the authors observe that mathematically optimal solutions are frequently inequitable, such that one has to choose between equity and efficiency. Nevertheless, the authors fully acknowledge the importance of the equity aspect in vaccine allocation and conclude that “new ideas are needed to reconcile equity and efficiency” in this area. This paper takes up the last‐mentioned research issue and exploits some useful analytical techniques from Duijzer et al. (2018) for investigating it. However, not only the extension to inequity aversion, but also the full treatment of the case of interaction between subgroups, require new analytical results that are provided in this paper.
Westerink‐Duijzer et al. (2020) consider a variant of the multipopulation situation where a central DM is lacking, but health agencies negotiate on sharing their available doses. The concept of the “core” from cooperative game theory is used to model this case. The authors use a case study on the redistribution of influenza vaccines to illustrate their approach.
As Duijzer et al. (2016) and some other articles, Enayati and Özaltın (2020) capture the vaccine allocation problem in the form of minimizing the number of vaccine doses needed to extinguish an emerging outbreak in its early stages, that is, to ensure that the reproduction number is less than or equal to unity. Their work achieves an essential progress on the one hand by proposing an exact solution approach, based on discretization with multiparametric disaggregation, on the other hand by incorporating equity constraints expressed in terms of the Gini coefficient. There are close relations to this paper, but three main differences have to be mentioned: (i) We consider outcome equity instead of input equity, which significantly increases the computational complexity. (ii) Instead of minimizing the number of doses required to extinguish the outbreak, we minimize the size of the epidemic for a given stockpile of doses. (iii) We do not use an equity constraint, but rather combine equity and efficiency to a compact (albeit parameterized) objective function satisfying well‐defined axioms.
In the context of the COVID‐19 pandemic, the trade‐off between efficiency and equity has also been addressed in some recent preprints as Bertsimas et al. (2020) or Chen et al. (2020). While these works use more involved models of the disease dynamics (adapted to COVID‐19) than this paper and also include the practically important aspects of timing and age groups, they put less emphasis on analytical insights into optimal vaccine allocation decisions. Insofar, this paper is rather in the line of articles as Duijzer et al. (2016) or Enayati and Özaltın (2020). Again in the context of COVID‐19, Munguía‐López and Ponce‐Ortega (2021) compare different fairness‐related objectives, as the Rawlsian criterion or the Nash solution from cooperative game theory, to the utilitarian objective where the sum of all individual utilities is maximized. The model does not specify an epidemiological model for representing the infection dynamics.
Pressman et al. (2021) aim at the development of an empirically measurable vaccine equity index for COVID‐19 vaccinations. In particular, the index should be able to quantify inequities between different racial or ethnic groups. For the purposes of this paper, Pressman et al. (2021) is especially relevant by the clear distinction the authors make between input equity and outcome equity (the authors use the terms “equality” and “equity” for these two notions, respectively), their proposed measure being of outcome equity type. Rastegar et al. (2021) build on Enayati and Özaltın (2020), but they modify the objective function definition by maximizing the minimum delivery‐to‐demand ratio per group and time period, a definition of Rawlsian type that captures efficiency and equity in one single function. This paper adopts a Gini index–based IAAF with the same aim; however, it also investigates a Rawlsian version of the problem, both within the framework of outcome equity rather than input equity. A further recent investigation on fair vaccine distribution can be found in Balcik et al. (2022).
For a review on models, methods, and applications of optimization under equity considerations, see Karsu and Morton (2015). Therein, a central notion of this paper, IAAFs, is discussed in detail, based on works as Kostreva et al. (2004). A special case of IAAFs are ordered weighted averages (OWAs), which occur under different names already early in the literature. For example, they are called generalized Gini indices in Weymark (1981) or symmetric comonotonically linear functionals in Ben‐Porath et al. (1997). In this paper, a particular class of OWAs will be used as social welfare functions allowing a simultaneous consideration of efficiency and equity: the class of linear combinations of the utilitarian measure (total or average benefit) with Gini's mean absolute difference (for the latter, see, e.g., Yitzhaki & Schechtman, 2013). This class is a parameterized set with a single parameter expressing the weight given to the Gini component. We call these functions GAFs. They are not new; for example, they have been investigated in detail in Porath and Gilboa (1994). Therein, besides a direct definition, also an axiomatic characterization in the form of seven axioms has been given. Recent applications of GAFs can be found in several papers as Gutjahr and Fischer (2018), Mostajabdaveh et al. (2019), or Gutjahr (2021). Moreover, also Eisenhandler and Tzur (2019a, 2019b) choose in their investigations a special GAF as their evaluation measure for inequity‐averse optimization. Another measure of OWA type, but different from GAFs, is used in Filippi et al. (2021).
Compared to the above‐cited literature, the new contribution of this paper to optimal vaccine allocation under fairness considerations can be seen mainly in the following issues: (a) The presented model is based on outcome equity rather than on input equity. (b) An IAAF of Gini type is applied as the objective function of the optimization approach in order to have a compact representation of both efficiency and equity. (c) An APR allocation with close connections to the Rawlsian solution is defined and shown to be optimal for a large range of preference profiles also under the Gini‐oriented evaluation perspective. (d) Numerical solution techniques for the proposed model are developed. (e) The model is extended to the practically relevant case of interactions between subgroups. (f) A new case study is presented, and two case studies from the literature are reanalyzed from a viewpoint including inequity aversion.
PROBLEM FORMULATION
Epidemiological model
The backbone of the epidemiological component of the proposed model is the well‐known SIR dynamics. As Duijzer et al. (2018) (cf. also the literature cited in Brauer et al., 2019, chapter 5), we apply it in a multipopulation context: It is assumed that the overall population decomposes into m subpopulations (patches), each of which is further subdivided into the three compartments “susceptible,” “infected,” and “removed.” The size of patch j is











As Duijzer et al. (2018), we suppose a situation where at a time τ in the early stage of an epidemic, a limited stockpile V of doses of a vaccine is available. For simplicity, we assume



The basic output variables on which our health outcome evaluation rests are the variables









From a utilitarian point of view, that is, when disregarding equity aspects, the resulting optimization problem is the following:
Before turning to the conceptual extension of (2), let us address the question how












A frequently studied special case in the literature is that of no interaction between subpopulations. In this special case,






In the case of no interaction between the subpopulations, the quantity


An alternative representation of





Including equity
It has been recognized in the vaccine allocation literature that applying the utilitarian objective function “sum of the benefits of all individuals,” as expressed formally in the optimization model (2), can lead to highly inequitable and perhaps socially unacceptable vaccine distributions (cf. Duijzer et al., 2018; Enayati & Özaltın, 2020; Keeling & Shattock, 2012). This paper follows Enayati and Özaltın (2020) and other works in the choice to express inequity by a Gini‐related measure, but it deploys this concept in a quite different way. First of all, we rather strive for equity in health outcomes







Second, instead of splitting the efficiency and the equity issue over objective function and constraints, respectively, we use a single compact IAAF as the overall aggregated assessment of a solution

Gini aggregation functions
To take equity into account, we replace in (2) the objective function by a weighted sum of the utilitarian objective and a 1‐norm deviation of the outcomes across subpopulations:















While the choice of the inequity aversion parameter λ is up to the subjective preferences of the DM, it can be made understandable to the DM what a specific value of λ means by giving simple numerical examples. A way to elicit a rough estimate of λ from the DM is the following: Consider the case of two persons to whom the DM wants to provide benefits of some kind. Let y
1 and y
2 be the benefits allotted to persons 1 and 2, respectively, under distribution plan A, and let







For example, we may ask the DM how large the benefit x would have to be so that she/he is indifferent between the two distributions (60, 40) and



In addition to the use of a GAF as the objective function, which gives Problem (6), it will also be interesting to investigate the use of the simplest IAAF, the measure aggregating the individual benefits


An APR allocation
The well‐known pro rata (PR) allocation in vaccine allocation consists in allotting the available vaccine in proportion to the population sizes An APR allocation is a vector











An APR allocation lets the second term in the objective function of (6) vanish and provides in this way an allocation that is perfect from the equity point of view. In the next section, it will be shown that at least in the more specific scenario without interaction, under mild conditions, an APR allocation exists and is unique. The relations between the APR allocation, the Rawlsian solution, and the GAF solution need a deeper investigation, which will be one of the topics of the following sections. An obvious other topic is of course the question how the three types of solutions can be determined.
ANALYTICAL RESULTS
This section derives analytical results on vaccine allocation under different solution concepts, still on the assumption of no interaction between the subpopulations. For easier orientation, Figure 1 gives an overview.
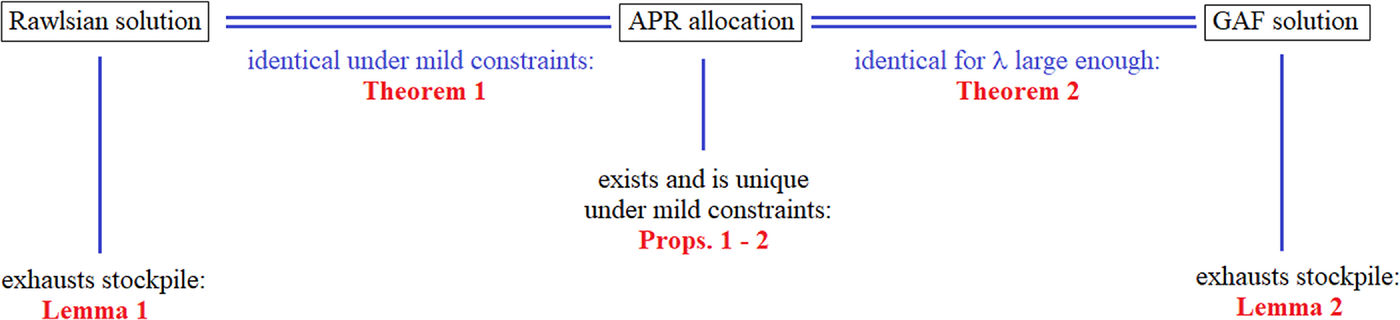
Schematic overview of the analytical results (case without interaction).
Existence and uniqueness of the APR allocation
For abbreviation, set The following conditions are necessary conditions for the existence of an APR solution:






The proofs of all mathematical results can be found in Supporting Information EC.2.
Note that in the special case where all





The conditions above, together with If (10) and


In the following, we shall impose condition (10)(b) in its inessentially strengthened form
Rawlsian solution and APR allocation
In the context of vaccine allocation optimization disregarding equity, Duijzer et al. (2018) showed that it is optimal to always use the complete vaccine stockpile, in other words, that the first constraint in (2) is satisfied with equality in an optimal solution. It turns out that on the not very restrictive condition (11), also in the Rawlsian context, an optimal solution exhausts the available stockpile: Suppose that the stockpile size V satisfies (11). Then, in an optimal solution of the Ralwsian problem (8), the constraint

With the help of this lemma, we can show that on mild conditions, Rawlsian solution and APR allocation are equivalent: Suppose that the stockpile size V satisfies (10)(a) and (11). Then, the Rawlsian optimization problem (8) possesses a unique optimal solution, namely, the APR allocation.
The GAF solution
We turn now to the use of a GAF as the objective function, as described by problem formulation (6). Let us start by the observation that also the GAF solution, as the Rawlsian solution, completely exhausts the available stockpile: Suppose that the stockpile size V satisfies (11). Then, in an optimal solution of the GAF problem (6), the constraint

Next, we discuss the relation of the GAF solution to the APR allocation. By definition, the APR allocation reduces the second term of the objective of (6) to the minimal possible value of zero. Thus, the APR allocation corresponds in a certain sense to the limiting case



Intuitively, one would expect that as λ is reduced from ∞ to a large finite value and further on through a sequence of decreasing numbers, such that gradually more and more weight is shifted from equity to efficiency, the optimal solution vector f should, gradually again, move from the APR allocation to solution vectors taking the efficiency aspect more and more into account. This intuition turns out to be wrong, as we will show. Actually, mixing an increasing concern for efficiency into the objective function of (6) by reducing λ will at first not impair the (exact) optimality of the APR allocation at all. Only for a typically already rather low value of λ, the solution will jump to a vector that pays attention to the efficiency criterion (and change then gradually in the case of a further reduction of λ). Let
















Local and global optimality of the APR allocation
Motivated by the last examples, it is tempting to ask under which conditions the APR allocation already solves the GAF problem to optimality. The next lemma confirms that a threshold value for λ decides on this issue. This is valid both for the question of local and for that of global optimality (with different threshold values). In the sequel, If for some







While the results in this section generally refer to the case without interaction, a look at the proof of Lemma 3 shows that the lemma holds in the case of interaction as well.
The next result shows that by choosing λ sufficiently large, the APR allocation can always be made globally (and hence also locally) optimal. Although this property may be expected, as for large λ, the second term of the objective function of (6) dominates the first term, proving the result rigorously for the general case is surprisingly intricate.2
To each instance of the vaccine allocation problem (6), there is a



Theorem 2, together with Lemma 3, suggests the following definition: Let The local APR optimality threshold is the smallest λ for which APR is locally optimal:
The global APR optimality threshold is the smallest λ for which APR is globally optimal:



Thus, by Lemma 3, the APR allocation is locally optimal w.r.t. the GAF measure for



Definition 2 extends in a formally identical way to the case where interaction is present, with the only difference that in this case, it can happen that the set for which





For numerical purposes, a slight extension of Definition 2(b) is necessary: With















For the computation of Let V satisfy (11), and let









NUMERICAL SOLUTION
In this section, we indicate numerical solution methods for (a) the problem (6) of finding the optimal vaccine allocation w.r.t. a GAF, (b) the problem of determining the local and the global APR optimality thresholds,


It has to be mentioned that larger instances of problem (a) cannot be expected to be solvable to optimality because of its nonlinear and even nonconvex nature: Note that already the simpler problem of optimizing vaccine allocation without including a nondifferentiable equity term in the objective function has been recognized as computationally too challenging for exact optimization approaches (see Duijzer et al., 2018; Westerink‐Duijzer et al., 2020).3 Therefore, a two‐track approach has been followed here: First, an enumerative algorithm was developed. This algorithm is based on a suitable grid‐type discretization and enables the solution of smaller problem instances (up to ≈5 patches) to a desired degree of accuracy, providing rigorous lower and upper bounds for the solution value of the maximization problem. In order to identify the bounds, we need to know to what extent the function values in the continuous domain can deviate from those in the grid points. For this purpose, we determine a Lipschitz constant of the objective function and use it to calibrate the mesh size of the grid. The details are described in Supporting Information EC.5.
Second, a PSO metaheuristic (Poli et al., 2007) for the numerical solution of larger instances was implemented and assessed by comparison to the results of the enumerative algorithm on small instances. The PSO algorithm builds on an appropriate encoding of the solution space, together with a repair mechanism for infeasible solutions. The description of the algorithm as well as results on its quality evaluation are provided in Supporting Information EC.6.
From an applied point of view, one would wish to be able to specify upper bounds










Contrary to problem (a), the first of the problems listed under (b), namely, the determination of the local optimality threshold


Finally, we addressed the harder problem of the estimation of the global optimality threshold, where we relied again on the discretization approach as well as on the PSO metaheuristic. This led to Algorithm 1 and Algorithm 2, respectively, which are presented in Supporting Information EC.7. Algorithm 1 determines a lower and an upper bound on Teytelman and Larson (2013) investigate a vaccine allocation model for the 2009 H1N1 influenza epidemic in the United States. In Table EC.11 in the Supporting Information, the numbers
















Also for 12 randomly generated test instances investigated in Supporting Information EC.6, a majority of 75% produced PSO‐based lower bounds (and even upper bounds) below 0.10, as seen there.
An investigation of the influence of varying stockpile size V on the optimal allocation, analyzed at an example taken from Keeling and Shattock (2012), can be found in Supporting Information EC.8.
INTERACTION
In this section, the concepts and procedures of the previous sections will be extended to the case where there is interaction (positive infection rates) between the subpopulations. Two types of application may be of specific interest: a first one where subpopulations are defined by geographical regions or political districts and a second one where subpopulations are formed by age groups. (Also combinations may be envisaged, see Enayati & Özaltın, 2020.) It will be seen that the results for these two types show marked differences, even after the application of the same concepts. The section will focus on a generalization of the APR allocation and of the solution optimizing the GAF. The relations between APR allocation and the Rawlsian solution in this more general context is a topic of future research.
Computation of the APR allocation in the presence of interactions
An APR allocation has been defined by Definition 1 already in a context including the possibility of interactions. We are now interested in a way how to compute the APR allocation also in the presence of interactions. For this purpose, we build on Equation (3). Slight reformulation and use of the assumption The following properties hold: The function The function






















Lemma 5 can be used as follows for efficiently solving (18): First, observe that constraint










If the intersection of the










The proposition below derives monotonicity properties concerning the influence of transmission rates and of initial fractions of susceptibles on the APR allocation. Regarding its second part, recall that as a consequence of the assumption of no removed individuals at the beginning, a smaller number of susceptibles at time 0 entails a larger number of infectious persons already at time 0.
With Suppose that j and















It can be conjectured that the GAF solutions converge to the APR allocation If the APR allocation exists, then as










Computation of the GAF solution in the presence of interactions
If there is interaction, the solution of the optimization problem (6) becomes especially challenging because already the determination of the objective function value






OTHER GENERALIZATIONS
Vaccine efficacy
Up to now, it was assumed that vaccination is 100% effective and leaves complete immunity. In particular, this assumption entails also that a vaccinated person cannot transmit the disease to any other individual. For many infectious diseases, this is an oversimplification. Therefore, we relax the assumption along the lines of Hill and Longini Jr (2003) (see also Duijzer et al., 2016, online appendix D) by assuming that a vaccination achieves its goal only in a certain fraction







As Duijzer et al. (2016) remark, the introduction of efficacy factors simply rescales the parameters









Patch‐specific weights
One might be interested in being able to assign different weights to the numbers of infected cases in the single subpopulations. Let



Instead of the outcome variables







An APR allocation can be defined for the described weighted case analogously as for the original unweighted case: Generalizing Definition 1, we call a vector




To compute the APR allocation for the weighted model, we set now








Finally, the optimal ζ is the determined as the solution of the following counterpart of (18):

Susceptible‐exposed‐infectious‐removed (SEIR) and SI n R models
Our approach can also be extended from SIR models to SEIR models, or, more generally, to SI
n
R models. SEIR models address latency by including an “exposed” state E, while SI
n
R models assume n different infectious stages with different transmission parameters. As remarked in Ma and Earn (2006), SEIR is a special case of SI
n
R, so it suffices to consider SI
n
R. Final size formulas for SI
n
R in the form of systems of equations are available for particular situations; see, for example, Theorem 9.2 in Ma and Earn (2006), which gives conditions ensuring that the final size formula for a multipatch SI
n
R model is of the same form as that for a multipatch SIR model. In such situations, our approach can be applied unchanged. In the general case, an (approximate) APR allocation can be determined as follows: As an initial solution, compute (along the lines of Section 6.1) the APR allocation of the corresponding SIR model based on the final size formula, and fine‐tune this solution then by minimizing the inequity term of (6) on the constraint of stockpile exhaustion, using PSO, where

CASE STUDIES
Case Austria
In this subsection, we use publicly available data4 from the first wave of the COVID‐19 pandemic in Spring 2020 in the nine provinces (“federal states”) of Austria. We take this wave as an instance of a severe and highly contagious epidemic and estimate all parameters needed for our model from the real‐world data, though we do not include all features of COVID‐19 in our case description. In particular, we assume an early availability of a vaccine, which was actually not yet available for COVID‐19 in 2020, and we assume that vaccination needs not to be repeated, but leaves long‐term immunity at least for a certain fraction of vaccinated individuals, an assumption that is now well known to be wrong for COVID‐19, but holds for some other infectious diseases. Thus, the goal of this case study is not to provide a fully adequate model for the very complex COVID‐19 pandemic, but to analyze a hypothetical situation based on parameter values as they could be valid for some future epidemic.
First of all, from the time series of daily incidences, daily estimates of the reproduction numbers for March 15 to April 3, 2020, in each of the nine provinces have been estimated (see Table 1). Their average values over the 20 days lie between between





Test cases Austria 1 and 2: The nine provinces (“federal states”) of Austria with their population sizes, estimated reproduction numbers, and case fatality rates (CFRs; in %) in the first wave of COVID‐19 (2020).


To obtain estimates of the transmission rates 


Map of the provinces (“federal states”) of Austria.
The reproduction number derived from the observed incidence data during March 15 to April 3, 2020, cannot be interpreted as the basic reproduction number 




A vaccine efficacy of 





Test cases Austria 1 and 2, results. Upper tables: utilitarian allocation (left) and adjusted pro rata (APR) allocation (right). Lower table: objective function values.








We can derive the following observations from Table 2:
Test case Austria 1: APR almost reaches the efficiency (measured by the utilitarian objective, the fraction of infection‐free individuals) of the utilitarian solution For moderate inequity aversion of








Test case Austria 2: At this test instance, where contact rates have been increased by 50%, the difference of the fraction of infection‐free individuals between The quality of It is striking that








The left graph of Figure 4 shows the dependence of 




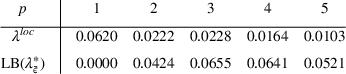
Test case Austria 1. Left graph: unweighted case, plot of the optimal Gini aggregation function (GAF) objective function value







For test case Austria 1, one obtains the following solutions, where 
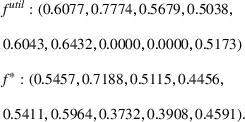






The right graph of Figure 4 plots the loss function 


The numerical results above allow it to estimate the price of fairness (Bertsimas et al., 2011), represented here by the difference between 




The downside of the utilitarian allocation, on the other hand, is that fatalities would be distributed very unjustly over the provinces: Tyrol, for example, would have to bear 


Considering the actual practice in many countries during the COVID‐19 pandemic, it rather seems that political DMs shied away from a utilitarian policy minimizing the total number of infections or of deaths, a policy that would necessitate the mentioned harsh inequalities in vaccine allocation, and opted instead for a broad distribution of vaccine, usually guided by the ordinary PR rule. For example, the European Union committed itself to “ensure that each country receives doses based on a PR population distribution key” (Bolcato et al., 2021). As our results for Austria 1 show, however, the PR policy may entail a much larger death toll than the utilitarian policy. Compared to PR, the GAF solution (which is in the case 
Case Teytelman and Larson 2013
A further application case, obtained by extending the case from Teytelman and Larson (2013) (which we already addressed in Example 2) to the situation of interactions between patches, is described in Supporting Information EC.11. The results are similar to those for Austria 1 and 2.
Case Wallinga 2010
In order to investigate also the situation where the population is not stratified into spatial clusters but rather into age groups, let us reanalyze an application case presented in Wallinga et al. (2010) and taken up again in Duijzer et al. (2016). Six different age groups are distinguished, and age group sizes 



As with the test case referring to Austria, we investigate two different versions: a version Wallinga 1 where the original transmission rates 







In view of the large 







Test case Wallinga 1, unweighted case. Blue upward triangles: supported efficient solutions for the biobjective problem with objective functions μ and Δ. Red downward triangles: same solutions with the second coordinate representing the Gini index
Starting from the rightmost point on the frontier, which corresponds to the utilitarian solution, one can see that already a small drop in efficiency by less than 0.5% suffices to achieve a reduction of the Gini index by almost 20%. Near the leftmost point of the frontier, which corresponds to the APR allocation, the marginal gain in equity bought by a reduction of efficiency is weaker. This effect is consistent with related observations in other publications (cf. Chen et al., 2020).



It turns out that an APR allocation does not exist anymore for Wallinga 1, weighted as described above. This is not quite surprising: The huge mortality differences between age group 1 and age group 6 cannot be equalized anymore by a suitable vaccination strategy relying on a limited stockpile of vaccine. One may ask whether the goal of providing each age group with the same excess mortality rate from the epidemic is meaningful at all. We cannot expect that the health‐related disadvantage of the elderly can be completely overcome by medical interventions. This consideration questions the application of established fairness measures to age groups, while such measures may be completely appropriate and justifiable when applied to regional subpopulations.
Whereas 






Utilitarian comparison of PR to APR
Although the purpose of APR is not to yield a good utilitarian evaluation but to maximize outcome fairness, some results in the case studies in Sections 8.1–8.3 suggest that the APR allocation provided by the weighted model might possibly be superior at least to the ordinary PR allocation also w.r.t. the utilitarian assessment by 

Comparison results for special cases with only 



















Table 3 summarizes the results. We see that only in 3 out of the 56 combinations, PR was superior to APR. These are combinations with small V and a small variation of the weights 
Results for 500 random test instances per entry, each instance with 




Similarly, the average sizes of the difference 










The general tendency to a superiority of APR observed in Table 3 is weakest in the case 












DISCUSSION AND POLICY IMPLICATIONS
The main message for practice derived from our numerical investigations above is that for epidemics of the considered type, already a comparably small weight given to the equity term in an aggregated evaluation of the vaccine allocation to geographical clusters typically tends to make an APR policy optimal. The necessary adjustment of PR is prompted not by efficiency considerations, but by a replacement of input equity with outcome equity: The goal is equal chances of escaping infection rather than equal chances of getting vaccinated. The proposed APR allocation can be computed by a fast numerical approach. It turns out that under regional stratification with comparably low contact rates between the regions, both the investigated artificially generated instances and the real world–based case studies usually reveal the APR solution as already best possible also in the GAF evaluation, except for DMs with an uncommonly low commitment to the equity goal.
While these results suggest that a healthcare DM faced with geographical subgroups can expect to be on the safe side by a suitably APR policy, this does not hold anymore for age‐based subgroup partitioning of the overall population. In the latter case, an APR allocation needs not to be optimal or may even not exist at all. By estimating the indices proposed in this paper, namely, local and global APR optimality thresholds, the DM can recognize such situations and, if necessary, apply the proposed heuristic procedure to get a tailored solution to the specific allocation problem.
As shown in Section 7, the presented model also allows it to take account of different weights of an infection case in different subpopulations, for example reflecting different rates of severe illness or of mortality. Empirically, marked regional differences in mortality rates can often be observed. Possible reasons might be differing speed of access to hospitals in urban and rural areas, or differing ways of dealing with diseases in different socioeconomic groups. If numbers of fatalities instead of numbers of infections are chosen as the outcome variables, the question of which price of fairness the society should accept becomes especially controversial. This question is first and foremost an ethical one and has to be discussed on the level of values. However, it has also a pragmatic aspect: In our case study Austria 1, it could be seen that the utilitarian solution (minimizing the number of fatalities) would completely deprive two provinces of vaccine. No matter how this is evaluated from an ethical point of view, it seems rather clear that it is not politically implementable in view of the resistance it would provoke. On the other hand, the ordinary PR solution is frequently rather inefficient, as indicated by the results in Section 8.4. The APR allocation may be a good compromise solution between utilitarian and PR allocation in such situations.
Some limitations of this work have to be mentioned. First, the extension from the classical SIR model to SEIR or SI n R would deserve an experimental investigation. Second, the assumption of vaccine supply at one time rather than by a series of deliveries should be relaxed by suitable model extensions. A natural way to deal with the latter case is to apply our approach repeatedly at different times, using at each time the observed state as the new initial condition (after relaxing the assumption that initially, no individuals are in the state “removed”). Of course, this does not guarantee optimality, and the obtained algorithm should be evaluated by comparison to other dynamic allocation algorithms. Similar remarks are in place for the related case where (as with COVID‐19) repeated vaccinations are necessary to achieve a sufficient degree of immunity.
A practical limitation of the presented approach concerns the possible difficulty to explain the solution aiming at outcome equity to the population. Admittedly, outcome equity is not quite as easy to defend by political DMs as input equity, since the prediction of outcome equity measures is model based and needs the involvement of epidemiological experts. Nevertheless, the difficulty regarding political communication would still be distinctly aggravated by a model‐based approach disregarding equity.
CONCLUSIONS
We extended models for optimal vaccine allocation to subpopulations by using social welfare functions that integrate the utilitarian criterion (“sum of all benefits”) with a fairness criterion (“equality of benefits”), based on the probabilities of being spared from infection. Three concepts were investigated: (a) an outcome‐based adjustment of the popular PR policy of vaccine allocation, (b) the Rawlsian solution (“best outcome for the worst‐off”), and (c) the allocation optimizing a linear combination of the utilitarian objective and Gini's mean absolute difference, called GAF. On the theoretical level, we showed that (a) and (b) are basically equivalent. Moreover, also (a) and (c) tend to produce the same solutions, provided that the degree of inequity aversion, the weight parameter used in the linear combination defining the GAF, is not too low. We defined threshold values for this parameter, above which the APR allocation simultaneously optimizes the GAF, and proposed procedures for computing good estimates for these thresholds. Moreover, exact as well as heuristic solution algorithms for computing the optimal vaccine allocation also in the cases where it is different from APR have been provided. Furthermore, a generalization to subpopulation‐specific weights of infections was investigated, which allows it to analyze questions about fractions of hospitalization or of fatalities.
Numerical results differed for the cases of spatial and of age‐based stratification. In the first case, the optimality threshold is typically low, which recommends the APR allocation as a both fair and efficient policy. In the second case, the APR allocation only optimizes the combined objective function if the DM's inequity aversion is comparably high, so that losses in terms of fairness have to be taken into account in order to achieve an optimal total health benefit. However, the question how “fairness between age groups” should really be measured may remain subject to discussion.
Footnotes
1
For convenience, we shall include in the definition of the GAF the boundary case
2
There may possibly be connections of this result to the theory of optimization with sparsity‐inducing norms, as it has been studied for parameter fitting applications (see, e.g., Bach et al., 2011). The aim is there to get sparse models by letting only a limited subset of the model parameters deviate from zero. This is managed by extending the objective function with a penalty term containing the 1‐norm of the parameter vector. Our problem formulation is not the same as that in sparse optimization, as we do not apply the 1‐norm to the coefficients ![]() guarantees that this can be achieved by giving the penalty term a sufficiently large weight λ. Considering the parallels with sparse optimization, we conjecture that a replacement of the 1‐norm in the penalty term of the GAF definition by some other
guarantees that this can be achieved by giving the penalty term a sufficiently large weight λ. Considering the parallels with sparse optimization, we conjecture that a replacement of the 1‐norm in the penalty term of the GAF definition by some other
3
Because of the convex–concave nature of the objective function of (2), already the special case ![]() ) have shown NP‐hardness.
) have shown NP‐hardness.
4
5
The reader should be aware that this refers to infection rates as the outcome variables; for the consideration of severe courses of the disease, see the results for the weighted model below.