
Abstract
Objectives
Topiramate (Topamax®) is licensed to be used, either in monotherapy or as adjunctive treatment, for generalized tonic-clonic seizures or partial seizures with or without secondary generalization and for prevention of migraine. The safety of topiramate in human pregnancy is largely unknown. Here we report on our experience of pregnancies exposed to topiramate.
Methods
This study is part of a prospective, observational registration and follow-up study. Suitable cases are women with epilepsy who become pregnant while taking topiramate either singly or along with other antiepileptic drugs (AEDs), and who are referred before outcome of the pregnancy is known. The main outcome measure is the major congenital malformation (MCM) rate. Secondary outcomes include risk of specific MCM, minor malformation rate, birthweight, and gestational age at delivery.
Results
Full outcome data are available on 203 pregnancies. Of these, 178 resulted in live birth; 16 had an MCM (9.0%; 95% CI 5.6–14.1%). Three MCMs were observed in 70 monotherapy exposures (4.8%; 95% CI 1.7–13.3%) and 13 in cases exposed to topiramate as part of a polytherapy regimen (11.2%; 95% CI 6.7–18.2%). Four of the MCMs were oral clefts (2.2%; 95% CI 0.9–5.6%). Four cases of hypospadias were reported (5.1%; 95% CI 0.2–10.1%) among 78 known live male births, of which two were classified as major malformations.
Conclusions
The number of outcomes of human pregnancies exposed to topiramate is low, but the MCM rate for topiramate polytherapy raises some concerns. Overall, the rate of oral clefts observed was 11 times the background rate. Although the present data provide new information, they should be interpreted with caution due to the sample size and wide confidence intervals.
Commentary
The conclusion that a pregnant woman should remain on an AED is usually reached easily. A more common concern is the risk of teratogenicity conferred by the AED. There are no prospective controlled trials of AEDs in pregnant women for obvious ethical and logistical reasons; therefore, case series of pregnant women are the basis for assessment. The teratogenic risk of AEDs is seemingly low. Because large numbers of pregnant women with epilepsy on AEDs must be examined in order to find enough cases of major congenital malformations (MCMs) to calculate the teratogenic risk with any degree of certainty, large pregnancy registries have been the answer to this problem. The results, methodology, and limitations of these registries were reviewed in a recent consensus statement (1). Modern registries have been well designed to minimize bias, particularly with regard to selection, by enrolling women before the outcome of their pregnancy is known, then obtaining follow-up data to determine the outcome of the pregnancy.
Hunt et al. report the MCM rate for topiramate from the United Kingdom (UK) pregnancy registry. The MCM rate for topiramate was 4.8% for 70 monotherapy exposures and 11.2% for 108 polytherapy exposures. It is notable that 2.2% of topiramate treated patients had oral clefts; however, the confidence intervals are large so that the exact frequency is difficult to determine. The confidence intervals even include 1.0, raising the possibility that any increase risk calculated could be due merely to the small number of patients registered to date. Similarly, four cases of hypospadias were reported, representing 5.1% of males, but this result has similar statistical limitations. Careful analysis of statistical considerations has led some to conclude that these limitations are avoided when results are not reported until 500 exposures have been collected in the registry (1). Thus, we will have to wait to determine if there is truly an increased rate of oral clefts or hypospadias in topiramate treated patients.
The overall rate of MCM reported here for topiramate treated patients is lower than that reported by Ornoy et al. in the only other similar large case series examining topiramate teratogenicity (2). Ornoy et al. identified four cases of MCM out of 41 live births from 52 pregnancies during topiramate treatment. This rate of 9.8% was not statistically different from the rate of 3.4% for 206 controls, obtained from women who had contacted their local teratogenicity information service. Interestingly, the investigators identified statistically significant lower birth weight and greater rate of spontaneous abortion in the topiramate treated group. The small number of patients on topiramate and the lack of strict controls, unfortunately, mean that the study of Ornoy et al. suffers even more from statistical limitations than other studies.
Statistical limitations aside, the overall rate of MCM attributed to topiramate is similar to the rate reported for most other AEDs that have been investigated in pregnancy registries. The essential results are listed in the Table 1 and previously have been reviewed in detail (1). The risk reported for lamotrigine (1.4–3.2%) is very low overall but may be increased for oral clefts, although a different approach suggests no increased risk (3). The risk of levetiracetam is 2.7% from the same UK registry that reports here the risk of 4.8% for topiramate; however, much larger numbers of patients will have to be investigated to determine if the risk of topiramate is really greater than levetiracetam. The risk for carbamazepine (2.2–4.0%) is comparable to topiramate and other second-generation drugs investigated so far. There is a trend toward higher risk for conventional AEDs because of the higher numerical risk associated with phenytoin (5.9%) and phenobarbital (6.5%) than with topiramate.
Risk of Major Congenital Malformation in Women with Epilepsy (in percent; Adapted from Meador et al. (1))
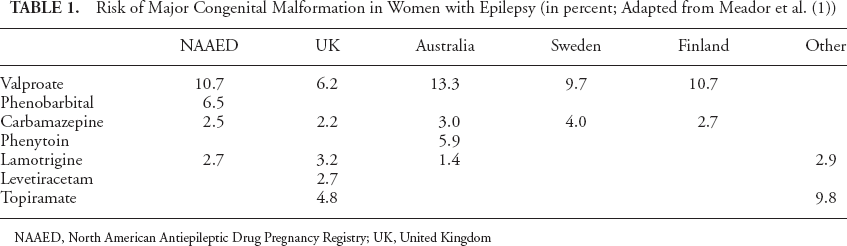
NAAED, North American Antiepileptic Drug Pregnancy Registry; UK, United Kingdom
It is very clear that the teratogenic risk for valproate (6.2–10.7%) is higher than for topiramate and all other AEDs reported so far (4). The risk of valproate was as high as 38.5% for doses greater than 1,100 mg per day in the Australian registry. Furthermore, valproate is associated with neural tube defects, which generally are more debilitating than cleft lip and palate associated with other AEDs. Valproate stands out as the one AED that should be avoided during pregnancy, when alternatives are available.
Is the rate of MCM significantly higher in women with epilepsy than in the general population? Birth defects occur in 1.6 to 2.3 percent of all live births (5,6). With the exception of valproate, the MCM rate for women with epilepsy taking AEDs is about twice the background rate, as a generality. This finding may cause women to be concerned. However, the absolute risk is still less than 4% for most AEDs. Therefore, women can be reassured that the vast majority of pregnancies turn out normal for women with epilepsy. However, it is certainly prudent to take measures aimed at minimizing the risk of birth defects, especially by recommending the use of prenatal folic acid and proper obstetric care.
What is the clinical significance of the findings reported by Hunt et al. and the pregnancy registry results reviewed here? On one hand, both clinicians and patients can be reassured that the results of systematic research confirm the clinical impression that most AEDs, other than valproate, have a low risk of anatomic teratogenicity. On the other hand, this fact does not address the risk of more subtle or delayed cognitive effects of intrauterine exposure to AEDs. Overall, recommendations typically are to continue AED treatment for pregnant women with epilepsy, avoid valproate, and hope that second-generation AEDs have relatively lower teratogenicity.