
Abstract
We applied the International Headache Society (IHS) classification coding parameters to a study population of 652 cluster headache (CH) patients, in order to determine how many patients did not fulfil the diagnostic criteria for group 3.1 and to find out any diagnostic elements that could be changed in the upcoming revision of the classification to make it more relevant to current clinical practice. Ninety-nine patients were found to have cluster-like disorder (3.3), including 74 (74.7%) who did not fulfil the diagnostic criteria for CH, because either pain was not associated with any of the accompanying autonomic phenomena listed in the classification or it was not located orbitally, supraorbitally and/or temporally. A review of our total sample showed that 72.0% of patients reported frontal and occipital pain location; in 61.8%, 33.4% and 39.1% of cases, attacks were also accompanied by restlessness/agitation, nausea and photophobia, respectively. In a coding system that took into account the diagnostic elements that we considered in our study, group 3.1 of the existing IHS classification would actually include 51 of the 99 patients currently coded as 3.3.
Introduction
The 1988 International Headache Society (IHS) classification (1) has the great merit of having recognized cluster headache (CH) as a separate entity, correctly differentiating it from other migrainous disorders grouped under the heading ‘Vascular headache of migraine type’ of the previous 1962 Ad Hoc Committee classification (2). Though allowing for the distinctive clinical features of CH that make it easily recognizable vs. other forms of primary headache, the IHS classification has necessarily restricted the choice of diagnostic elements to those that have received scientific recognition in published reports. As a consequence, a large number of CH patients may be classified by current investigators as belonging to the 3.3 group of the IHS classification ‘Cluster headache-like disorder not fulfilling above criteria’ instead of being more aptly coded to the CH diagnostic group 3.1.
Therefore, the purpose of our study was to: (a) investigate a large sample of patients to determine how many of them did not fulfil the IHS classification diagnostic criteria for 3.1; and (b) to find out any diagnostic elements that could be added to or changed in the upcoming revision of the classification to make it more relevant to current clinical practice.
Methods
Our study population consisted of all 652 CH patients (470 men and 182 women) seen for the first time at the University of Parma Headache Centre between December 1975 and December 1999. Prior to data analysis, we reviewed our patients' clinical records – which have not changed since 1975 and have ever since reported all clinical parameters required for diagnosis down to the four-digit level of the IHS classification – and revised all pre-1988 CH diagnoses accordingly (1). (See Table 1 – letter heading E was omitted in the table, because we considered only primary CH cases.) Within the selected patient sample, we identified those patients who fell within the 3.3 group ‘Cluster headache-like disorder not fulfilling above criteria’ of the existing IHS classification (3.3 patients). Under heading B of the IHS classification, pain location is defined as orbital, supraorbital and/or temporal. The term ‘supraorbital’ may seem too vague, but from the anatomo-topographic standpoint it clearly and accurately defines the area between the orbital region (whose uppermost part corresponds to the eyelid) and the anterior margin of the frontal region, representing a line that stretches from the zygomatic process of the frontal bone on one side to the corresponding process on the other side, passing through the root of nose and the orbital ridge over the eyebrow (3).
Cluster headache – diagnostic criteria (IHS 1988) ∗
Letter heading E was omitted because in this study we reviewed data only for primary CH patients.
Under letter heading B of the diagnostic criteria for CH (group 3.1), the IHS classification lists pain severity, laterality and location, and duration of attacks. Nosographically, a diagnosis of cluster-like disorder can be made even when more than one of the four above criteria are not fulfilled. However, in the case of our 3.3 patients, who had to be classified as such because they did not fulfil the criteria listed under B, only one of the four criteria was not matched. It is reasonable to assume that the headache forms in which pain did not match two or more of the features listed under the second letter heading of group 3.1 had not been considered as CH forms even at the time of the patients' first visit. For the 99 3.3. patients in our sample, we considered such general data as mean age at the first observation, mean age at headache onset and the temporal pattern of the attacks to determine which three- or four-digit level of categorization they would have belonged to if they had fulfilled all the criteria listed in the IHS classification. We also calculated the extent to which the 3.3 patients did not fulfil the different criteria.
For the accompanying autonomic phenomena and pain location, we analysed in detail those more frequently reported by the 3.3 patients and the remaining 553 CH patients, and also others than those listed in the IHS classification. Finally, based on our analysis and on previous literature reports, we considered possible modifications of the existing IHS classification and reviewed the adherence of our 3.3 patients to the diagnostic criteria thus modified.
Results
In our sample, the patients classifiable as 3.3 were 99/652 (15.2%), including 59/470 males (12.6%) and 40/182 females (22.0%). The remaining 553 patients (84.8%) were coded to the 3.1 group. Mean age of the 3.3 patients at the first visit was 39.1, standard deviation (
All 3.3 patients fulfilled the criteria listed under letter heading A, because at the time of their fist visit all of them reported more than five attacks. Most of these patients, however, did not match the diagnostic criteria for CH as described at 3.1 of the IHS classification because their headache was not accompanied by any of the autonomic phenomena listed in the classification in 45.5% of patients (45/99), or because pain was not orbital, supraorbital and/or temporal in 29.3% of patients (29/99, see Table 2). Pain was bilateral in 5.1% of patients (5/99). The attacks lasted either less than 15 min or more than 180 min in 15.2% of patients (15/99) and recurred either less than once every other day or more than eight times a day in 5.1% (5/99). In particular, attacks lasted less than 15 min in four patients out of 15: 3–5 min in one female, approximately 5–7 min in two other females and about 10 min in one male. In the remaining 11 patients the attacks lasted more than 3 h, including seven patients reporting a duration between 180 min and 10 h.
Unfulfilled criteria for patients coded to group 3.3 of the IHS classification ‘Cluster headache-like disorder not fulfilling above criteria’ in a sample of 652 cluster headache patients

Letter heading E was omitted because in this study we reviewed data only for primary CH patients.
Among the 45/99 3.3 patients who did not report any of the accompanying autonomic phenomena listed in the IHS classification, eight (17.8%), five males and three females, did not report any symptoms associated with pain, while the remaining 37 (82.2%), 24/29 males (82.8%) and 13/16 females (82.3%), reported at least one accompanying symptom other than those listed in the IHS classification (non-IHS), the average being 2.1 symptoms for each patient (range: 1–6). Analysis of the non-IHS accompanying symptoms in the 37 3.3 patients and in the 553 CH patients (411 males and 142 females) showed that restlessness/agitation, nausea and photophobia were more common in both groups (see Table 3). If all these three symptoms were listed in the IHS classification under letter heading C, 31 out of our 99 3.3 patients (31.3%) would actually be coded to the CH group. A total of 27 patients (27.3%) would also be included in this group if restlessness/agitation and nausea were added to the listed symptoms. Finally, even if only restlessness/agitation was added, as much as 20.2% of the 3.3 patients (20/99) would be classified as actual CH sufferers.
‘Non-IHS’ associated symptoms in 37 patients with ‘Cluster headache-like disorder not fulfilling above criteria’ (3.3) in 553 cluster headache patients (3.1)

A similar procedure was applied to the study of pain location. In the 29 3.3 patients who did not report pain in the orbital, supraorbital and/or temporal regions and in the 553 CH patients, ‘non-IHS’ pain location was more frequently in the frontal, occipital and parietal regions (see Table 4). At the end of our review, we calculated the percentage of the 99 3.3 patients who would fulfil CH diagnostic criteria and be classified as CH patients if frontal and/or occipital pain location were also listed under B: 15.2% (15 cases out of 99) for patients reporting frontal pain location, 8.1% (eight out of 99) for patients reporting occipital pain location, and 20.2% (20/99) for patients reporting pain in both the frontal and the occipital region.
‘Non-IHS’ pain location in 29 patients with ‘Cluster headache-like disorder not fulfilling above criteria’ (3.3) in 553 cluster headache patients (3.1)

Discussion
Some forms of primary headache are not easily described nosographically because they share a few symptoms with other clinical entities. Any classification that is aimed at an ‘overall’ description must necessarily include broad, loosely defined ‘categories’ that comprise all that is ‘non-classifiable’. Yet, in our opinion, some of the criteria required for CH diagnosis under the IHS classification are too restrictive. As a result, a large number of patients who are certainly CH sufferers are misclassified as patients with cluster-like disorder. This point of discussion is not only a semantic one. Indeed, it is bound to affect any consistent selection of CH study populations. Having applied the IHS classification criteria to a large sample of 652 CH patients in order to gather scientific evidence to support our hypothesis, we found 99 patients who could be coded to the group ‘Cluster headache-like disorders not fulfilling above criteria’. Since the very first CH descriptions (4–6), pain location has always been reported as more common in the oculo-orbital region, which was also described as the region most frequently involved in 70% of cases by Manzoni et al. in 1983 (7). However, other authors also reported frequent involvement of the frontal region: Ekbom (5) in 72.4% of his case series, Lance (6) in 46.7%, and Kudrow (8) in 68.3% (425 CH patients). These reports are in agreement with our own observations of 57.7% of cluster-like patients (group 3.3) and 54.8% of CH patients (group 3.1) reporting frontal pain.
Based on these findings, frontal pain location can be considered as typical of CH patients in general and not only of that group of patients who do not match ‘classic’ pain location characteristics. Similarly, in our sample, occipital region involvement was reported by 30.8% of 3.3 patients and by 26.0% of CH patients. Other reports also appear to support our evidence. In 1980 Kudrow (8) reported a CH patient with pain in the ocular and occipital regions. More recently, Solomon et al. (9) have pointed out the frequent involvement of the nuchal region in a large proportion of their CH patients. Mathew (10) reported that in 18% of his case series pain might also be located outside of the trigeminal nerve region, as he demonstrated again in 1993 (11) in a group of patients with atypical pain location. In our case series, pain was located occipitally in about one-third of 3.3 patients (8/29); in most of them, the occipital region was not the only one involved, as the headache also extended to the frontal, cervical, carotid and parietal regions. When we included the frontal and occipital regions among the pain location criteria, we found that 20.2% of our 3.3 patients (20/99) could actually be coded to group 3.1.
CH patients without the typical accompaniment of autonomic phenomena have been repeatedly described after 1988. Of course, we cannot exclude the presence of subclinical abnormalities in those CH patients who did not report any accompanying symptoms. In 1990 Ekbom (12) reported five patients out of 163 who could not be classified as CH patients because of the lack of any accompanying autonomic phenomena. In their study of patients referred to the Headache Centres of Parma and Pavia, Nappi et al. (13) have found a high rate of photophobia (55.8%) and nausea (40.6%). In 1988 Vingen et al. (14) concluded that photo- and phonophobia are important accompanying symptoms of CH attacks and their conclusions have recently been confirmed by an in-depth analysis of CH clinical features in a large sample of patients referred to the Parma Headache Centre (15). Our own data analysis showed that nausea and photophobia were reported, respectively, by 37.8% and 29.7% of 3.3 patients and by 36.9% and 44.1% of CH patients. We then extended our analysis to include the well-known phenomenon of restlessness/agitation, aptly described by Blau (16) in 1993, which forces patients to move incessantly. In our sample, that symptom was reported by 54.1% of 3.3 patients and by 69.3% of CH patients, respectively. When we added restlessness/agitation, nausea and photophobia to the list of CH accompanying symptoms, 31.3% of our 3.3 patients (31/99) could be coded instead to 3.1.
Bilateral pain location was extremely rare (five patients, 0.8% of our sample). Although a few cases have been reported in the literature (17, 18), we do not believe that it can be considered such a distinctive feature of this form of headache as to be listed in the IHS classification.
A comparatively large proportion of patients did not match the IHS criteria for duration of attacks (15 patients out of 99, 15.2%), while frequency of attacks was not matched by 5.1% of patients (5/99). We believe that, for the time being, such cases can only be coded to 3.3. As the frequency and duration of attacks may vary from one attack to the next in the same patient, only a prospective study specifically aimed at evaluating variations in the temporal pattern of CH attacks will make it possible in the future to include some of these patients in the 3.1 group.
In conclusion, we believe that the evidence we gathered from a large sample of patients and the review of previous reports in the literature suggest the need for a change in the IHS classification, which under B should read ‘Severe unilateral orbital, supraorbital and/or temporal and/or frontal and/or occipital pain lasting 15–180 min untreated’, and under C should list also restlessness/agitation, nausea and photophobia among the accompanying autonomic phenomena. With those modifications, 51 of our 99 patients (51.5%) who had to be coded to group 3.3 ‘Cluster headache-like disorder not fulfilling above criteria’ of the current IHS classification (see Table 5) could actually be classified as CH patients.
Application of 1998 IHS diagnostic criteria (3.1) vs. modified diagnostic criteria in 652 cluster headache (CH) patients
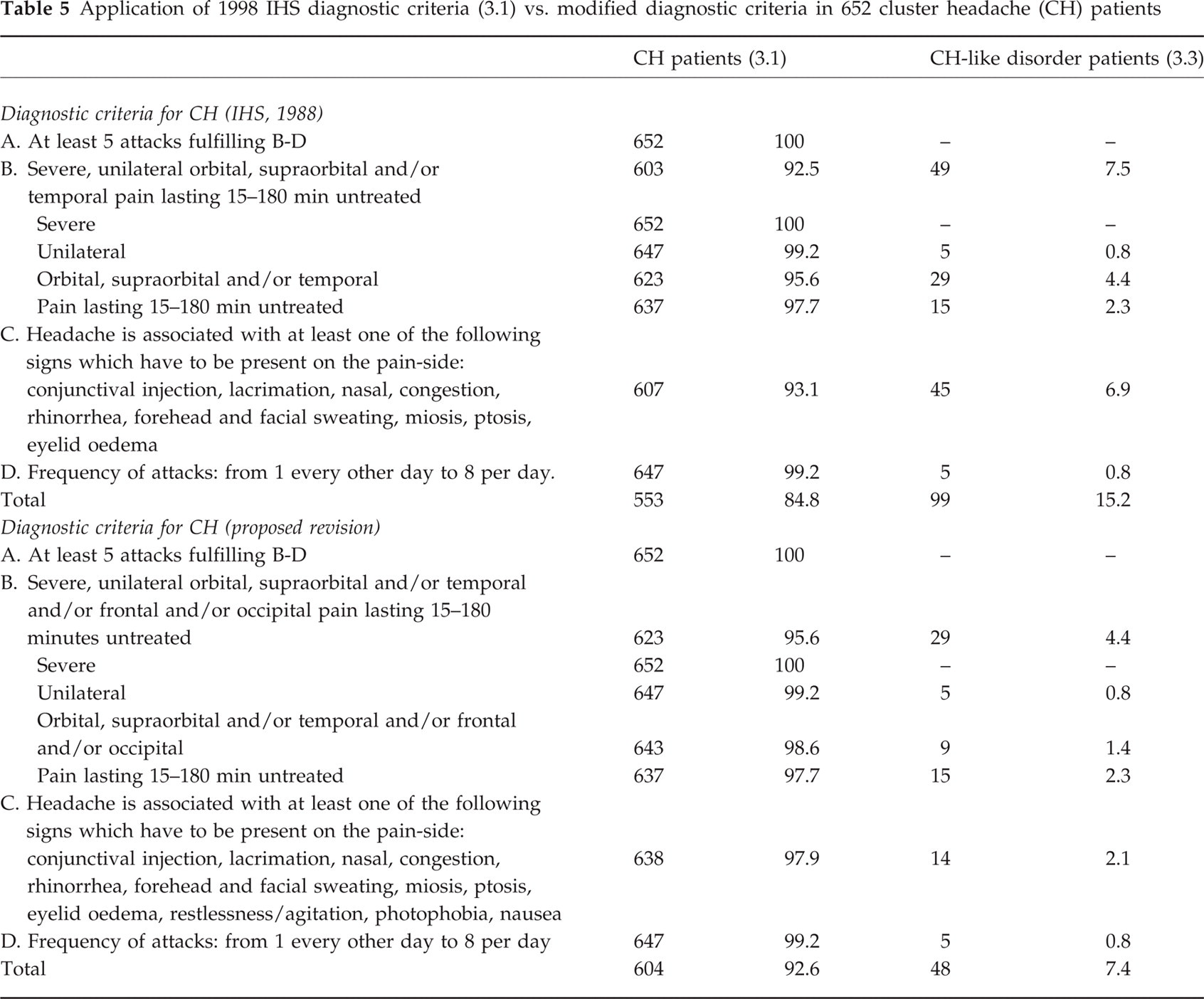
On the other hand, we do not believe that the addition of nausea and vomiting to the IHS list of accompanying symptoms would lead to inclusion of migraine without aura (MO) in the same group as CH patients, for the temporal pattern of duration and frequency of attacks in MO patients is totally different from that of CH.
Footnotes
Acknowledgements
This work was supported by Italy's Ministry for University Education and Scientific and Technological Research (MURST). Under the terms of the 1998 agreement for the allocation of funds to scientific research projects of national importance, MURST contributed to the funding of our study as part of the ‘Cluster headache pathophysiology’ research project.