
Abstract
An altered neurovascular coupling has been proposed in migraine. We aimed to investigate neurovascular coupling during a mental task interictally in patients with migraine without aura (MO) by near-infrared spectroscopy (NIRS). Twelve migraineurs and 12 healthy controls were included. Using NIRS, we recorded the magnitude and latency of cortical changes in oxyhaemoglobin (HbO2) and deoxyhaemoglobin (Hb) during the colour-word matching Stroop test via 16 channels covering the forehead. We found no differences in the magnitude of responses between migraineurs and healthy subjects in the incongruent Stroop task subtracted by the neutral Stroop task on either side of the frontal cortex for HbO2 (left, P = 0.984; right, P = 0.406) or Hb (left, P = 0.689; right, P = 0.406) values. No differences in error rate (P = 0.611) or reaction time (P = 0.936) were found between healthy subjects and MO patients for incongruent tasks. The present study suggests that vascular reactivity and oxygen supply during a mental task in patients with MO are intact interictally.
Introduction
Migraine is proposed to be an uncoupling disorder where the neuronal activity-induced metabolic demand, such as oxygen or glucose, is unmet by vascular supply (1–3). Cortical spreading depression (CSD), a pathophysiological correlate of migraine aura and probable cause of migraine headache following aura, has recently been put forward to lead also to migraine attacks without overt aura (4). Studies supporting the above notion essentially originated from findings in mutations leading to familial hemiplegic migraine (FHM) phenotypes (5) that affect glutamatergic synapses in the cerebral cortex, which can lower the threshold for CSD in animals (6) and might change neuronal excitability. Studies in migraine without aura (MO) have investigated cortical excitability interictally and so far revealed conflicting results ranging from hyperexcitability (7,8), hypoexcitability (9), normoexcitability (10,11) to dysfunctionality (12,13). In principle, increased extracellular glutamate, as described in FHM mutations, and changes in cortical excitability will affect the neurovascular coupling. This coupling could be tested via a specific neuronal task in combination with measurement of vascular reactivity.
Transcranial Doppler (TCD) studies have recorded velocity in the middle cerebral artery and reported increased (14–16) or normal (17–19) interictal vascular reactivity during metabolic CO2 challenges in MO patients. However, if neurovascular coupling is impaired in MO the changes might be subtle, and therefore TCD might not be sensitive enough to reveal indirectly changes occurring at the cortical microvasculature.
Near-infrared spectroscopy (NIRS) is well established as a non-invasive method of detecting changes in parenchymal haemoglobin concentration and oxygenation (20). NIRS provides an opportunity for continuous recording of cortical oxygenation during experimental tasks with an excellent temporal resolution. The main advantage of NIRS is the ability to detect directly microvascular changes occurring at the frontal cerebral cortex in relation to a specific neuronal task. The Stroop test is known to be an efficient and consistent activator of the prefrontal cortex (21), and vascular alterations driven by neuronal activity are probably achieved by a mental or executive function of the forebrain. Furthermore, the Stroop test is well suited for computerized applications. Previous studies have shown that NIRS reliably detects vascular changes at the frontal cortex during Stroop tests (22–24). General linear model (GLM) is the most widely used method for analysing functional magnetic resonance imaging (fMRI) data, and studies have shown a close relationship between the signals measured by NIRS and fMRI (25,26). Over the past 5 years extensive experimental studies, using visual stimulation, finger tapping and memory tasks, have validated and shown that GLM can be applied to NIRS data analysis (27–31). The device and the protocol used in the present study were previously employed in a study to perform feasibility analysis using GLM for making statistical inferences from NIRS data (32). The results were encouraging, which led us to use GLM for analysing the data obtained in this study.
We therefore employed a NIRS device (1) particularly designed for the human forehead to detect vasoreactivity through oxyhaemoglobin (HbO2) and deoxyhaemoglobin (Hb) alterations accompanied to a Stroop task interictally in MO patients compared with healthy controls. We hypothesized that migraineurs would show impaired interictal neurovascular coupling during a mental task.
Design and methods
Mean values of clinical features for migraine without aura (MO) patients in the study

The post processing of NIRS data was performed by investigators (K.C., A.A. and H.B.) who were blinded in respect of patient or control status.
The study was approved by the Ethics Committee of the Danish County of Copenhagen (H-KA-20070004). All subjects gave informed consent to participate in the study, which was undertaken in accordance with the Helsinki Declaration of 1964, as revised in Edinburgh in 2000.
Experimental paradigm
A colour-word matching Stroop test adapted from Zysset et al. (34) was performed as a single trial. All subjects did a short 2-min test run before the main test. Experiments were performed with the subjects sitting in a comfortable chair and right hand on a standard computer mouse in a silent, lightly-dimmed room. Stimuli were presented via an LCD screen 0.5 m away from the subject's head.
Subjects were presented with two words, one written over the other. The top one was written in ink-colour whereas the one below was in white (over a black background). Subjects were asked to judge whether the word written below correctly denoted the colour of the upper word or not. If so, subjects were to press the left mouse button with their right index finger and if not to press the right mouse button with their right middle finger. Subjects were informed to perform the task as quickly and correctly as possible. The experiment consisted of neutral, congruent and incongruent trials. In the neutral task the upper word consisted of four Xs (XXXX) in ink-colour. In the congruent task ink-colour of the upper word and the word itself were the same, whereas in the incongruent task they were different. To prevent subjects from focusing on the lower word and blurring out the top word, the top word was presented 100 ms before the lower word. In this way, visual attention is shifted automatically to the top word (34).
The stimuli were presented in a semi-blocked manner. Each block consisted of six trials. The inter-stimulus interval within the blocks was 3 s and blocks were placed 15 s apart in time. The stimulus type within a block was homogeneous (but the arrangement of correct and false stimuli might change), i.e. a block consisted, for example, of only congruent trials that may be correct or false. There were 10 blocks of each stimulus type. The stimuli stayed on the screen until the subject responded or disappeared at the end of 2 s if the subject did not respond.
NIRS acquisition
Experiments were performed using a continuous wave near-infrared spectroscopy device (NIROXCOPE 301) built in the Biophotonics Laboratory of Bogazici University (Istanbul, Turkey) (1,35,36). The NIROXCOPE 301 transmits near-infrared light from light-emitting diodes (LEDs) at two wavelengths (730 and 850 nm) that are known to be able to penetrate through the scalp and probe the cerebral cortex (37,38). The device detects the light attenuation at these wavelengths and, using the attenuation characteristics of HbO2 and Hb, calculates the relative concentrations of these chromophores using modified Beer–Lambert Law, which empirically relates the optical attenuation to the chromophore concentrations and absorption characteristics in a highly scattering medium (39). Modified Beer–Lambert Law states that the attenuation of the light is proportional to the concentration of the absorbing molecule (c), extinction coefficient (ε), distance between the light source and detector (d), differential path length factor (B) and the factor due to scatter (G).

Using this equation and assuming a constant scattering during the measurements, the concentration change (Δc) may be calculated by:

In the above equation, the change in light attenuation (ΔA) is measured, d is determined by the position of the source-detector pairs and ε is taken from previous experimental studies. B depends upon the actual path the photons travel before reaching the detector. It is not possible to measure the path length by continuous wave NIRS devices. Hence, the concentration change is found up to a scaling factor, B. The values are normalized against baseline for each individual.
Employing four LEDs and 10 detectors, the device can sample 16 different volumes in the brain simultaneously (Figure 1). Distance between each source and detector is 2.5 cm, to obtain a probing depth of approximately 2 cm from the scalp surface (38). The light source and detectors give a total of 16 channels in an area of 20 × 7 cm of the forehead, where the centre bottom light detector is placed on the Fz position of the international 10–20 EEG system (40). LEDs and detectors were placed in a rubber band that was specially designed to fit the forehead. Sampling frequency of the device was 1.7 Hz.
Representative data obtained from one subject. (a) Averaged oxyhaemoglobin (HbO2) data from left lateral detectors (1–4). (b) Averaged deoxyhaemoglobin (Hb) data from left lateral detectors. (c) Averaged HbO2 data from right lateral detectors (13–16). (d) Averaged Hb data from right lateral detectors. Shaded areas denote the trial blocks, from dark (neutral) to light (incongruent).
We employed the GLM to be able to derive the haemodynamic parameters of interest (32). Stimulus onset vectors for each type of stimulus (neutral, congruent and incongruent) were formed and convolved with the canonical haemodynamic response function. For modelling the latency of the haemodynamic response, temporal derivative of the canonical haemodynamic response function was also added as a regressor (41). The NIRS data were digitally low-pass filtered with a cut-off frequency of 0.33 Hz. To be able to cope with various low-frequency trends, discrete cosine transform functions (42) were added to the design matrix with a minimum period of 120 s. Incorrect and omitted trials were modelled separately and they, together with the trend terms, form the nuisance part of the design matrix.
The GLM was run separately for each subject and each detector was analysed individually. Hence for each subject and for each detector of a subject we derived the parameter estimates of canonical haemodynamic response function and its temporal derivative. The latencies were estimated from the estimated coefficients of the main response and derivative terms. Using Taylor series expansion, Friston et al. (41) have shown that it is possible to get a good estimate of the latency from the ratio of the coefficient of the derivative term to the main response. The latency estimate is adjusted so that it will shrink towards zero when there is little evidence for a stimulus response according to the method described by Liao et al. (43). Contrast vectors were used to find the differences in haemodynamic responses among different trial types and the corresponding statistical significances of these estimates were calculated. The leftmost detectors (1–4) were denoted as the left lateral detectors and the rightmost detectors (13–16) were denoted as right lateral detectors. Then for each subject among these detectors those that exhibited statistically significant responses for the given contrast were determined. For these detectors contrasted magnitude and latency estimates were calculated. These values were averaged separately for each subject for the left and right lateral detectors. Hence, at the end, for each subject and for each contrast two (one for left lateral cortex and one for right lateral cortex) magnitude estimates and two corresponding latency estimates were determined. Figure 2 shows representative averaged data from the lateral detectors for HbO2 and Hb obtained from one subject.
Illustration of near-infrared spectroscopy (NIRS) light sources and detectors in 16-channel arrangement covering the forehead in a 20 × 7 cm area.
Statistics
All values are presented as mean ± 1 standard deviation (
The primary end-points were the differences in HbO2 and Hb magnitude between migraineurs and healthy subjects in the incongruent task subtracted by the neutral task (interference effect) and the incongruent task subtracted by the congruent task.
The secondary end-points were the differences in HbO2 and Hb latency between migraineurs and healthy subjects in the incongruent task subtracted by the neutral task and the incongruent task subtracted by the congruent task.
Exploratory end-points were: (i) differences in error rate and reaction time between migraineurs and healthy subjects in the neutral, congruent and incongruent tasks; (ii) differences in error rates and reaction time within groups between neutral vs. incongruent and congruent vs. incongruent tasks.
For comparison of migraineurs vs. healthy, non-parametric Mann–Whitney U-test for two independent samples was performed. For comparison of error rates and reaction time within groups, Wilcoxon signed ranks test for two related samples was performed.
All analysis was performed with SPSS for Windows 16.0 (SPSS Inc., Chicago, IL, USA). Five per cent (P < 0.05) was accepted as the level of statistical significance.
Results
All 25 subjects completed the Stroop test without any apparent problems.
NIRS results
We found no differences in the magnitude responses between migraineurs and healthy subjects in the incongruent Stroop task subtracted by the neutral Stroop task on either side of the frontal cortex for HbO2 (left, P = 0.984; right, P = 0.406) or Hb (left, P = 0.689; right, P = 0.406) values. No differences in the magnitude responses between migraineurs and healthy subjects were found on either side of the frontal cortex in the incongruent Stroop task subtracted by the congruent Stroop task for HbO2 (left, P = 0.936; right, P = 0.810) or Hb (left, P = 0.936; right, P = 0.689 (Table 2 and Figure 3).
Magnitude (+1 Differences in magnitude estimates (± 1 IS, incongruent Stroop task; NS, neutral Stroop task; CS, congruent Stroop task; MO, migraine without aura.

Differences in HbO2 and Hb latency estimates in seconds (± 1
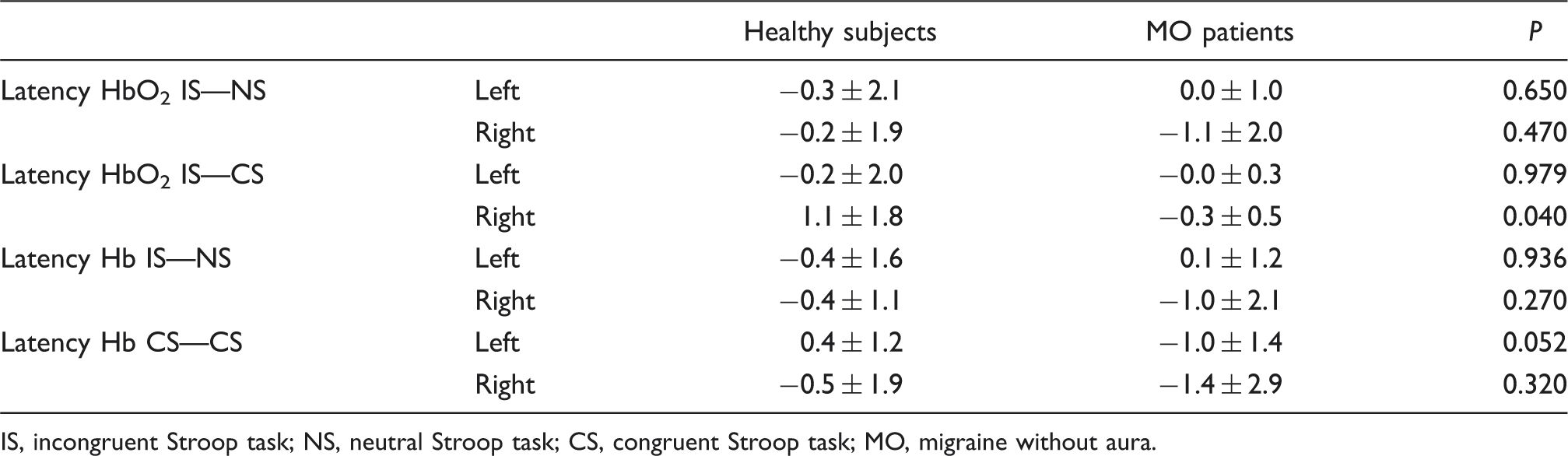
IS, incongruent Stroop task; NS, neutral Stroop task; CS, congruent Stroop task; MO, migraine without aura.
Behavioural results
No differences were found in error rate between healthy subjects and MO patients in neutral (P = 0.437), congruent (P = 0.137) or incongruent tasks (P = 0.611) (Table 4 and Figures 4 and 5). No differences were found in reaction time between healthy subjects and MO patients in neutral (P = 0.650), congruent (P = 0.979) or incongruent tasks (P = 0.936). We found larger error rates in healthy subjects (P = 0.013) and MO patients (P = 0.042) in incongruent task compared with the neutral task, but not in incongruent task compared with the congruent task (healthy, P = 0.050; MO, P = 0.622). We found larger reaction times in healthy subjects (P = 0.001) and MO patients (P = 0.021) in incongruent task compared with the neutral task, as well as in incongruent task compared with the congruent task (healthy, P = 0.001; MO, P = 0.002).
Error rates (+1 Reaction times (+1 Error rates (± 1 Error rates neutral vs. incongruent tasks. Error rates congruent vs. incongruent tasks. Reaction times neutral vs. incongruent tasks. Reaction times congruent vs. incongruent tasks. The Mann–Whitney U-test was used to test differences between groups and Wilcoxon signed ranks test to test differences within groups.


Discussion
Major findings
No signs of neurovascular impairment associated with working memory task were detected in MO patients interictally. Activation of HbO2 and Hb were similar in both migraineurs and healthy controls. The only abnormal finding was in one secondary end-point, which showed an increase in latency response on the right side of the frontal cortex in healthy subjects compared with migraineurs in the congruent task subtracted by the neutral Stroop task for HbO2, which is probably a type 1 error. We detected no sign of cognitive impairment as the error rates and reaction times among MO patients were similar to healthy subjects. Furthermore, the Stroop test showed significant increases in error rates and reaction time in the incongruent vs. neutral task as a sign of Stroop interference in both groups.
Is neurovascular coupling altered in MO patients?
An increase in glutamate at the synaptic cleft might lead to increased neuronal excitability (44). FHM2 mutation uncovers a potential pathway by which neurovascular metabolic coupling could be affected in migraine patients. The glutamate release from presynaptic neurons is indirectly coupled to Na-K ATPase activity, glycolytic pathway and glucose uptake in to perisynaptic astrocytes (45). Any metabolic dysfunction in that pathway could lead to neurovascular uncoupling, where the activity-driven neuronal demand for O2 or glucose is unmet. If the migraine syndrome as a chronic episodic disease has effects beyond sensory processing areas (4), subclinical involvement of other cerebral cortical areas would be expected. Therefore normal interictal vascular reactivity during working memory in the present study would not support the notion that migraine is a widespread neurovascular coupling disorder.
Studies investigating cortical excitability interictally in MO patients are conflicting (7–11). The deficiency in habituation found interictally in MO patients (13) could reveal cortical dysfunction, but it might not reflect impairment of ion-channel function at neuronal synapses or neurovascular coupling. This is supported by a recent study by Bolla et al. (46) investigating the electrophysiological profile of genotyped patients with FHM type 1 and 2, which surprisingly showed that FHM patients had an increased habituation in sensory and nociceptive evoked activities compared with healthy subjects.
The Stroop task has been widely employed to investigate frontal function and working memory in functional studies (22,32,47–49). The present study is in contrast to that of Annovazzi et al. (50), who found slower reaction times interictally with a Stroop test in six MO and seven migraine with aura (MA) patients compared with controls. Furthermore, Schmitz et al. investigated 16 MO and eight MA patients interictally and found impairment in executive function compared with controls, which was correlated with decreased frontal grey matter density (51). However, both studies employed mixed MO and MA populations. Using mixed populations might give a different result, as MO and MA might not share the same pathophysiology, since spreading cortical hypoperfusion, which probably reflects CSD, is only reliably apparent in MA patients (52,53).
If neurovascular coupling is disturbed to a great extent in MO patients, it should manifest with cognitive deficits. However, the evidence of interictal cognitive deficits in MO patients is controversial (54), as some studies show cognitive impairment interictally (55–57) and others no cognitive impairment compared with controls (58–61). A large study of 347 twins with MO investigated cognitive scores on fluency, digit span, delayed word recall, and symbol digit substitution test and found no differences in cognitive scores compared with twins without MO (61). If there is indeed cognitive deficit in MO patients, it might also be attributed to other confounding factors, such as white matter lesions (62), rather than a fundamental impairment of neurovascular coupling.
Three other studies using NIRS have investigated metabolic and mechanical perturbations interictally in MO patients (1,63). Akin et al. (1) and Liboni et al. (2) both found diminished vasoreactivity interictally in MO patients during breath-holding tasks, while Shinoura and Yamada (63) found pressure-related vasoreactivity, during a head-down tilt, to be suppressed in the right hemisphere of MO patients. By contrast, Vernieri et al. (64) demonstrated that during hypercapnia, induced by CO2 inhalation, vasoreactivity was increased on the migraine pain side interictally in MA patients as measured by NIRS, which also emphasizes the probable pathophysiological differences between MO and MA conditions. These metabolic and mechanical perturbations might be demanding and rely on good compliance from the subjects to obtain accurate results. Furthermore, it is important to differentiate a mental task from a breath-holding or head-tilting test. The latter two also influence arterial carbon dioxide concentration and intracranial pressure, thereby the signal generated could be larger than merely neuronal activity-driven vascular changes. The previous studies do not imply any activation of neurons and therefore they do not investigate real neurovascular coupling.
Methodological considerations
NIRS recordings of a Stroop test showed activation at the lateral prefrontal cortex bilaterally in control subjects and patients with cerebral microangiopathy (CMA), which revealed a reduced haemodynamic response in CMA patients in tight correlation with behavioural slowing during the Stroop task (23). NIRS measured during a Stroop test over the left forehead showed significant correlation between total Hb and cerebral blood flow measured by positron emission tomography (24). A study found a similar pattern of activation for both congruent and incongruent Stroop tasks in NIRS channels located left superior-frontally (22). Ciftci et al. (32), with a Stroop paradigm and same NIRS system as in the present study, found left lateral prefrontal cortex activation for HbO2 during interference condition that was much less pronounced for Hb. A recent study by Luu and Chau has demonstrated the feasibility of recording extracerebral haemodynamics along with cortical haemodynamics during a decision-making task (65). Thus, it seems evident that the NIRS technique detects parenchymal vascular alterations of the frontal cortex during the Stroop test.
Finally, we should also consider that intact neurovascular coupling in response to Stroop test detected by NIRS in MO interictally could be due to: [i] the existing vascular differences being too vague to be detected by NIRS; [ii] the Stroop test is a mental task displaying frontal lobe function, which might not be involved in migraine pathophysiology compared with temporal and occipital lobes.
Conclusion
We conclude that neurovascular coupling is intact in MO patients between attacks a measured with NIRS during a mental task. On the other hand, the ictal phase comprising prodrome, aura or headache could be accompanied by neurovascular coupling alteration, which should be tested in future studies.
Footnotes
Acknowledgements
The study was supported by the Bogaziçi University Research Fund through projects 04X102D and 04S101 and by Turkish State Planning Organization through projects 03K120250 and 03K120240. The study was also supported by the Lundbeck Foundation via the Lundbeck Foundation Centre for Neurovascular Signalling.