
Abstract
The course of migraine without aura (MO) is greatly influenced by the events of female reproductive life. Much less is known about migraine with aura (MA). The aim of this study was to evaluate the relationship between MA and the milestones of reproductive life. A retrospective case control study was carried out on 100 women affected by migraine with typical aura (cases) and 200 age-matched women with MO (controls). Pre-menstrual syndrome was found to be much more common among the patients with MA (odds ratio (OR) 6.0; confidence interval (CI) 3.1–11.6). Menstrually triggered migraine was more frequently encountered among MO than among MA patients (MA 15.0%; MO 53.5%; OR 0.1; CI 0.1–0.3). In both forms of migraine, pregnancy had a favourable effect; however, a lower percentage of MA (43.6%) than MO patients (76.8%; OR 0.2; CI 0.1–0.5) showed improvement or remission. The use of oral contraceptives worsened migraine in MA more frequently than in MO patients (MA 56.4%; MO 25.3%; OR 3.8; CI 1.6–9.3). The course of MA seems to be influenced by female reproductive life events, but in a different way with respect to MO.
Introduction
Migraine is typically a ‘women’s disease'. It is far more frequent in women than in men (with a female-to-male ratio of 2.5–3:1) (1–3), and this gender imbalance appears to be evident at puberty (4, 5). After the menarche, the events of reproductive life deeply influence the course of the disease. Menses, pregnancy, the post partum period, oral contraceptive (OC) intake, menopause, and hormone replacement therapy all modulate, negatively or positively, the course of migraine (6–16). Indeed, it is has been known for a long time that migraine can begin at menarche (17), worsen cyclically during menses (18), improve or recede during pregnancies (19) and disappear after the menopause (15). Such a pattern, however, really applies only to the most common type of migraine: migraine without aura (MO). The relationship between critical female hormonal changes and the course of migraine with aura (MA) has been the focus of much less study. Previous reports, however, indicate that MA may be differently modulated by reproductive life events from MO. Indeed, MA is less likely to be affected by menstruation (8, 20–22) and more likely than MO to worsen during pregnancies (9, 10).
The aim of the present study was to clarify the relationship between the course of migraine and hormonal milestones in MA patients, in comparison with MO patients taken as a control group.
Subjects and methods
A case control study was carried out on female out-patients, aged 18–55 years, referred to the Pavia Headache Centre. The cases were 100 consecutive patients (mean age 33.5 ± 11.4 years) affected by migraine with typical aura. Besides age, the only inclusion criterion was the absence, also historically, of attacks of MO. For every case, we selected two age-matched (± 2 years) controls, affected by MO and with no history of MA attacks. Both the cases and the controls had lived for at least 6 months in the vicinity of the headache centre. The diagnosis of migraine with typical aura and MO was made according to the International Headache Society (IHS) criteria (23).
Data collection
Having obtained the consent of all the participants, a detailed questionnaire was administered by physicians who were unaware of the study hypotheses to both cases and controls. The following data were recorded: personal details, physiological history, gynaecological history, events of reproductive life, OC intake and the changes induced by these events on the course of migraine. As regards gynaecological history in particular, menstrual cycles were defined as ‘irregular’ if their length had been either more than 32 days or less than 24 days for more than half of the subject's reproductive life. The presence of pre-menstrual syndrome (PMS) was investigated using a checklist of the more common pre-menstrual complaints (Calendar of Premenstrual Experience, COPE, Italian version) (24). Women presenting with menstrual symptomatology in at least 80% of their menstrual cycles were considered to be affected by PMS. The relationship between migraine and the menstrual cycle was categorized into four groups: (i) attacks only during the menstrual period, i.e. ‘pure menstrual migraine’. Women who only had migraine attacks starting on day 1 ± 2 of the menstrual cycle were considered as affected by menstrual migraine, in accordance with McGregor's definition (25); (ii) attacks mostly during menstrual period, i.e. ‘menstrually triggered migraine’ (26); (iii) attacks occurring at random during the menstrual cycle; (iv) attacks never occurring during the menstrual period. Since some women had had only one pregnancy and others more than one, we decided to compare the effects on the migraine course of only the first pregnancy in all the women. In the case of the multiparae, the effects of pregnancy on their headache could have differed between pregnancies (10). The data concerning the course of migraine during OC use referred to the last cycle of ‘pill’ intake prior to our observation. We did not analyse the type of OC used, as many women were not able to recall the commercial name of the drug taken. Both for pregnancy and OC intake, changes were defined as a reduction or an increase of at least 50% in the attack frequency.
Statistical analysis was performed using the McNemar χ2 test to compare the significance of differences between cases and controls for the factors considered.
Results
Personal details
As regards occupation and education, no significant differences emerged between the two forms of migraine, while investigation of marital status revealed that patients with MA were less often married than those with MO (odds ratio (OR) 0.5; confidence interval (CI) 0.3–0.9) (Table 1).
Personal details
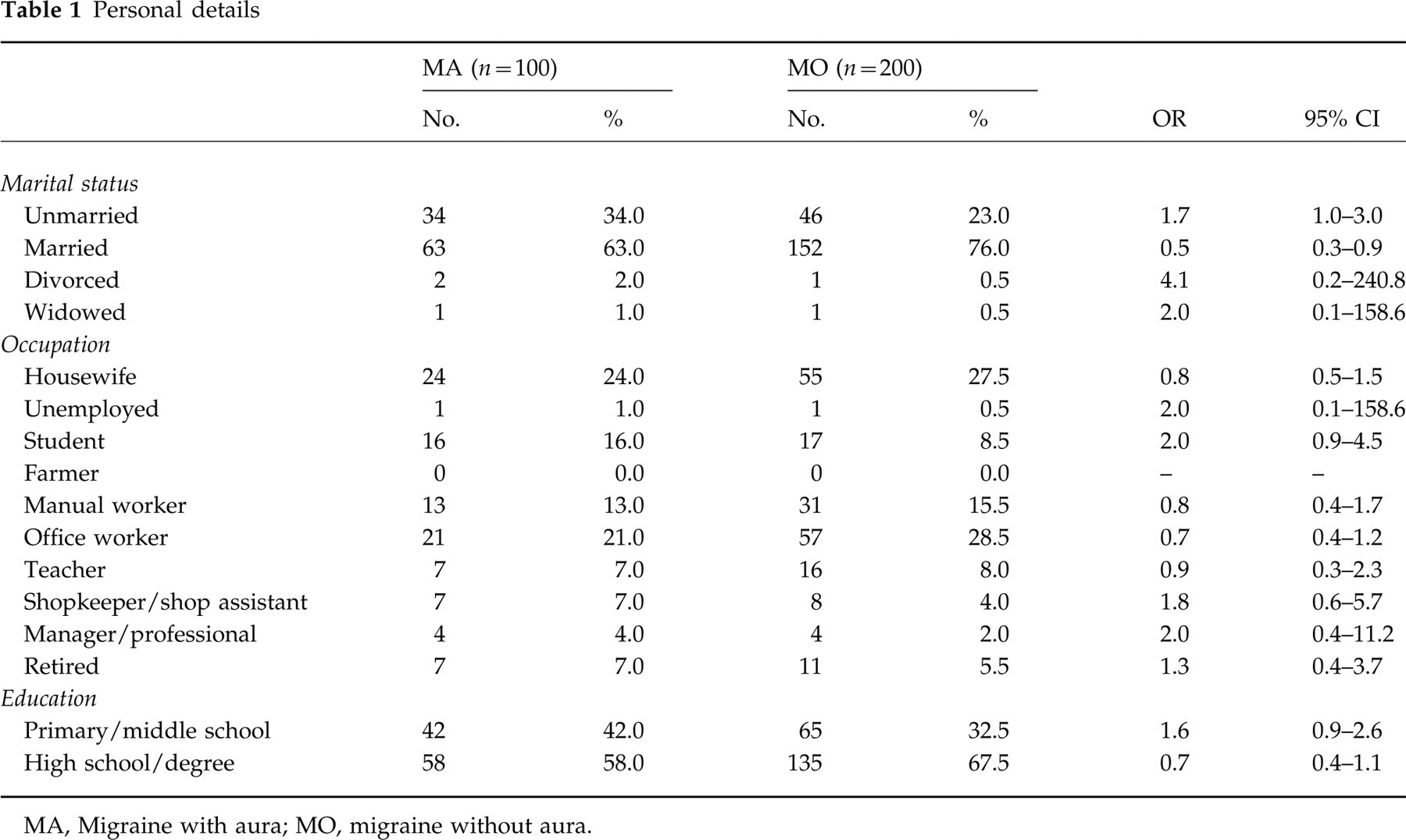
MA, Migraine with aura; MO, migraine without aura.
Gynaecological history
The patients affected by MA suffered from dysmenorrhoea less frequently than those with MO (OR 0.2; CI 0.1–0.5) and tended to have more regular cycles (OR 0.5; CI 0.3–1.0). In contrast, PMS was much more common among the patients with MA (OR 6.0; CI 3.1–11.6) (Table 2).
Gynaecological history
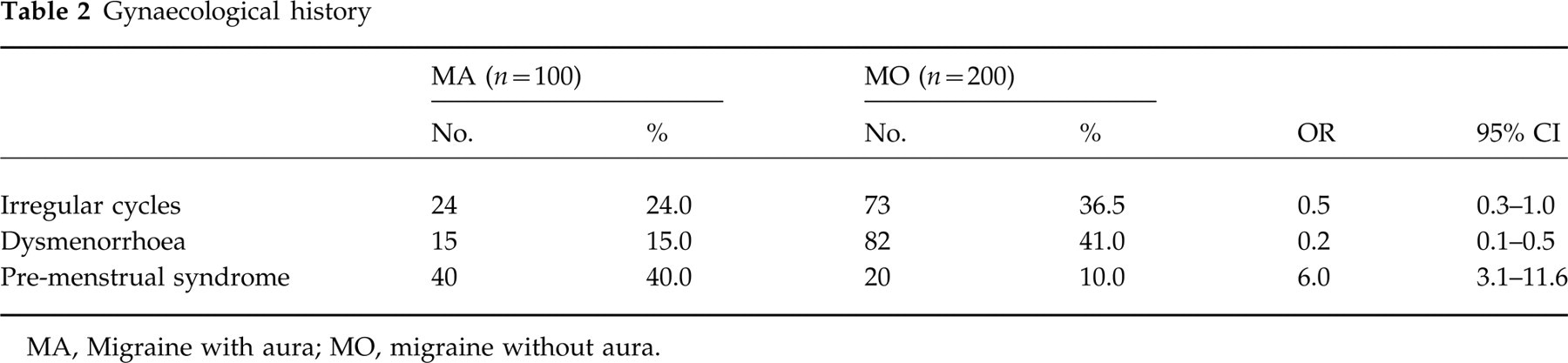
MA, Migraine with aura; MO, migraine without aura.
Relationship between migraine onset and reproductive life events
In several cases the onset of migraine coincided with the major events of reproductive life, but no significant differences emerged in this regard between MA and MO, with the exception of onset during OC intake (OR 10.6; CI 1.1–509.1) (Table 3).
Relationship between migraine onset and reproductive life events

OC, Oral contraceptive; MA, migraine with aura; MO, migraine without aura.
Number of women who had had pregnancies.
Number of women who had taken OCs.
Number of women in menopause.
Relationship between migraine attacks and menses
No difference in the occurrence of pure menstrual migraine emerged between the two forms (MA = 4.0%, MO = 3.5%; OR 1.1; CI 0.2–4.6), while menstrually triggered migraine was more frequently encountered among MO than among MA subjects (MA = 15.0%; MO = 53.5%; OR 0.1; CI 0.1–0.3). Moreover, in a high percentage of MA patients migraine never occurred during the menstrual period (MA = 27.0%, MO = 2.5%; OR 14.4; CI 5.2–49.3) (Table 4).
Relationship between migraine attacks and menses

MA, Migraine with aura; MO, migraine without aura.
Course during first pregnancy
As shown in Table 5, pregnancy had a different effect on each of the two types of migraine: MO, in fact, improved more often than MA in pregnancy (MA = 43.6%, MO = 76.8%; OR 0.2; CI 0.1–0.5), while MA patients more commonly showed no change in their migraine course during pregnancy (MA = 48.7%, MO = 22.2%; OR 3.3; CI 1.4–7.9).
Course of migraine during first pregnancy in patients already suffering from migraine at the time of their first pregnancy

MA, Migraine with aura; MO, migraine without aura.
Course during OC intake
Use of OCs worsened the headache more frequently in MA than in MO subjects (MA = 56.4%, MO = 25.3%; OR 3.8; CI 1.6–9.3). In both forms a small number of patients, in contrast, reported an improvement in their headache (Table 6).
Course of migraine during oral contraceptive use

MA, Migraine with aura; MO, migraine without aura.
Course after menopause
The study did not include enough menopausal women to allow an analysis of the migraine course after the cessation of menses.
Discussion
Some clinical and epidemiological studies have suggested that MA and MO are two distinct nosological entities (20, 22, 27). Among other distinctive elements, it appears possible to differentiate between the two disorders on the basis of their course in relation to the events of female reproductive life. There are reports (21) which have focused on this topic; however, this study is, to our knowledge, the first case control study devoted to this subject.
Our study has several limitations. First of all, it was conducted on out-patients of headache centres, i.e. on a highly selected population. It is well known, in fact, that migraineurs attending tertiary care centres have, on average, a more severe form of the disease in comparison with migraineurs from the general population; furthermore, they may differ in many other aspects, such as education, social background, etc. Indeed, it is only with great caution that these results should be generalized to the totality of migraine patients. Second, we chose to carry out a retrospective study in order to analyse the relationship between migraine and all the events of reproductive life (menarche, menses, pregnancy, OC intake, menopause); we certainly could not, without conducting a longitudinal study of several decades' duration, have applied a prospective design to our study of all these subjects. While one merit of this approach is that it allows us to obtain a global view of the relationship between migraine and female hormone changes, a fault is its lacks of precision. The course of migraine during the menstrual cycle or during OC intake would have been better studied by means of a prospective diary-based study. Moreover, our study is subject to recall bias, even though this is reduced, in our opinion, by the fact that the control group was not made up of healthy individuals, but of patients affected by another form of migraine, which means that a recall imbalance between cases and controls is, in general, unlikely. A recall bias cannot be ruled out, however, in the case of certain specific events, such as migraine onset during pregnancy. A first-ever MA attack that occurs during pregnancy, for example, will doubtless frighten a woman much more than the occurrence of a ‘simple’ headache, and therefore be more clearly remembered.
Let us now examine in detail the relationship between migraine and the various aspects of reproductive life. As regards gynaecological history, the higher prevalence of dysmenorrhoea among MO patients could hypothetically be explained by a high release of prostaglandins in the menstrual phase of the cycle in these subjects. It has been suggested that during menses women with menstrual migraine have abnormally raised plasma prostaglandin levels (28). Indeed, the role of these substances in provoking dysmenorrhoea is well established (29). As regards the high occurrence of PMS in the MA group, there are no data in the literature that can corroborate our finding. Previous studies have mostly investigated the relationship between menstrual migraine and PMS (30, 31). Facchinetti et al. found a PMS prevalence of 64% in 22 women affected by menstrual migraine and of 33% in 12 women with MO, concluding that a strong comorbidity exists only between menstrual migraine and PMS (31). The aetiology of PMS is controversial, but some data favouring a psychogenic origin have been produced (32, 33). It is known that MA (much more than MO) is comorbid with several psychiatric disorders, i.e. major depression (34), panic attacks (35), and suicide attempts (34). It could therefore be hypothesized that psychogenic disorders—and this is what PMS probably is—may occur more frequently in MA, in which the psychiatric comorbidity is more prominent.
When examining onset coinciding with the menarche, no difference emerged between the two migraine forms, and our data are supported by the findings of Cupini et al. (21) and Russell et al. (22). Onset of migraine during pregnancy is not an unusual event, ranging—if we do not consider the outlying percentage (80%) found by Callaghan (36)—from 1.3% (7) to 18% (19) of cases. In addition, several anecdotal reports (37–40) describe cases of MA onset during pregnancy, especially in the third trimester. Maggioni et al. (10) recently reported that MA showed a higher tendency for onset during pregnancy than MO (MA = 2/14 cases, 14%; MO = 9/90 cases, 10%). In accordance with this study and other reports (20, 21), we too found a trend towards a higher incidence of MA (10.7%) with respect to MO (3.8%). The same trend emerged in the post partum period (MA 8.9%; MO 3.1%). As regards the use of OC, we found, at variance with Cupini et al. (21), a significant difference between the two forms of migraine, with a higher incidence of the disorder emerging in MA (11.4% vs. 1.2%), even though, in view of the small sample size, caution should be exercised when interpreting these data (CI 1.1–509.1).
Unlike other investigators (21, 22), who have found a higher prevalence of menstrual migraine among MO sufferers, we did not observe any difference between MA and MO as regards the prevalence of ‘pure’ menstrual migraine. This could be due to a selection bias, since patients with menstrual MO (who suffer from only one attack per month) are infrequently referred to headache centres, whereas patients affected by MA are more likely to be referred to a subspecialty centre, also for diagnostic reasons. Moreover, the low percentage of ‘pure’ menstrual migraine detected in both types of migraine may be due to the fact that we used very restrictive inclusion criteria. In fact, we considered only women who had suffered from menstrual migraine throughout their reproductive lives. Menstrually triggered migraine, i.e. migraine with attacks mainly occurring around the menses, was much more common in MO than in MA subjects, in accordance with previous reports (20, 21). The percentage of menstrually triggered migraine that we found in MO (53.5%) is roughly superimposable on that reported by other authors (7, 17, 21, 41). An unexpected finding of our study was the high percentage (27%) of MA patients in whom attacks never occurred during menses. The mean frequency of attacks in MA patients was about three per year (data not shown), but some patients had one attack per year or less. Therefore, this ‘paradoxical’ effect could simply be due to the low frequency of attacks in most MA patients who, by chance, had perhaps never experienced an attack during the menstrual period or, if they had, did not remember it. An alternative hypothesis involves a true protective effect of menstrual cycle-related changes in sex hormones and/or neurotransmitters in some patients with MA, even though the pathophysiological basis of such an effect is unclear. It is noteworthy that MacGregor et al. in their prospective study of patients affected by MO or MA (6) identified four groups of women: (i) with menstrual migraine (7.2%); (ii) with menstrually related migraine (34.5%); (iii) with attacks occurring throughout the menstrual cycle, but with no increase at the time of menstruation (32.7%); (iv) with attacks not occurring at the time of menstruation (25.5%).
In both the forms of migraine, pregnancy had a favourable effect and the percentage of patients who experienced a worsening during pregnancy was negligible in both the MO and MA groups. Migraine, however, seemed to improve or recede in a lower number of MA (44%) than MO subjects (77%; OR 0.2, CI 0.1–0.5). The findings of our study conflict with those of other investigators (10, 21, 22) who did not find significant differences between MA and MO in this respect. One of these studies (10), however, enrolled too few MA patients (n = 12) to allow any firm conclusion on this aspect to be drawn. On the other hand, Russell et al. carried out a survey on the general population (22), on subjects therefore in whom disease severity was probably not as great as that in patients referred to a headache centre. It is possible that this question can only be answered through a prospective study following a sufficient number of migraineurs throughout the whole course of pregnancy.
In accordance with other studies (7, 14), OC intake led to a worsening of headache in about a quarter of the patients affected by MO. The proportion of MA patients whose migraine worsened during the use of OC was significantly higher (56%; OR 3.8; CI 1.6–9.3), similar to that recently found by Cupini et al. (21). Since the package inserts of OCs, as well as the verbal instructions often given to patients, mention the possibility of the headache worsening, it cannot be excluded that this ‘warning effect’ may have negatively influenced the women, inducing them, in some cases at least, to attribute a spontaneous worsening of their migraine to OC intake.
On the basis of our results, both MA and MO seem to be modulated by the events of female reproductive life, but in different ways. To a great extent, the pathophysiological mechanisms underlying these different patterns are still to be discovered. Future studies should look at the fluctuations and the absolute values of sex hormones and other substances, including prostaglandins and opioids, in the two forms of migraine throughout the menstrual cycle and during hormonal treatments, in order to determine the mechanisms conditioning the different courses of MA and MO during fertile life in women.
Footnotes
Acknowledgement
This study was partly supported by a grant from the Ministry of Public Health ICS 030.9-RC96.70.