
Abstract
Using a 3-year nationwide population-based database, this study aims to examine the risk of adverse pregnancy outcomes in women with migraines, including low birthweight (LBW), preterm birth, infants born small for gestational age, Caesarean section (CS) and pre-eclampsia. We identified a total of 4911 women with migraines who gave birth from 2001 to 2003, together with 24 555 matched women as a comparison cohort. Multivariate logistic regression analyses showed that after adjusting for potential confounders, the odds ratios were 1.16 [95% confidence intervals (CI) = 1.03–1.31, P = 0.014] for LBW, 1.24 (95% CI = 1.13–1.39, P < 0.001) for preterm births, 1.16 (95% CI = 1.07–1.24, P < 0.001) for CS and 1.34 (95% CI = 1.02–1.77, P = 0.027) for pre-eclampsia for women with migraines compared with unaffected mothers. We conclude that women with migraines were at increased risk of having LBW, preterm babies, pre-eclampsia and delivery by CS, compared with unaffected mothers.
Introduction
Migraine, a common chronic-intermittent neurovascular disorder, strongly predominates in adult females (1) and affects almost a quarter of all women during their childbearing years (2,3). It often improves during pregnancy, but sometimes occurs then for the first time, and may be worse during the first trimester (4–6). There has long been concern about the relationship between migraine and pregnancy. Some reviews have concluded that although a history of migraines may increase the risk of pre-eclampsia, it has no adverse effect on the outcome of pregnancy (7–9). However, this conclusion is based on relatively few studies, most with inadequate sample size.
As far as we know, to date there are only two studies of pregnancy outcomes in pregnant women with migraines. A Hungarian study reported that severe maternal migraines may increase the occurrence of pre-eclampsia and severe nausea/vomiting during pregnancy (10), but they are not associated with unfavourable delivery outcomes. Another study by Wainscott et al. was carried out at the Princess Margaret Migraine Clinic, London, between May 1973 and June 1974. Similarly, they did not find any significant difference in pregnancy outcomes when comparing 450 women with migraines and 136 women without (11). However, both studies used survey research to collect the data, a technique that can result in recall bias. In addition, the small sample size used in both studies may fail to detect differences between women with migraines and the normal population.
Therefore, this study aims to examine the risk of adverse pregnancy outcomes in pregnant women with migraines, using a 3-year nationwide population-based database, taking the characteristics of infant, mother and father into consideration. Taiwan initiated a National Health Insurance (NHI) programme in 1995. Its nationwide population-based dataset allows us to trace all medical services used by all enrollees. The database provides a unique opportunity to use unselected national data to determine whether migraines are associated with an increased risk of adverse pregnancy outcomes, including low birthweight (LBW), preterm births, babies small for gestational age (SGA), Caesarean section (CS) and pre-eclampsia.
Methods
Database
We used two nationwide population-based datasets in this study. The first was the National Health Insurance Research Dataset (NHIRD) covering the years 1996–2003. Taiwan inaugurated the NHI programme in March 1995, and Taiwan's NHI programme, a single-payer system with the government as the sole insurer, provides universal coverage, comprehensive benefits and access to any medical institution of the patient's choice. The NHIRD includes a registry and all medical claims data for over 22 million enrollees, representing over 98% of the island's population. The NHIRD is one of the largest and most comprehensive nationwide population-based datasets currently available in the world.
The second dataset was drawn from the 2001–2003 Taiwan birth certificate registry published by the Ministry of Interior in Taiwan. Birth certificates include data on birthdates for both infants and their parents, gestational week at birth, infant birthweight, gender, parity, place of birth, parents' educational levels, and maternal marital status. Registration of all births is mandatory in Taiwan, so the birth certificate data are very accurate and comprehensive. One study by Lin et al. has verified the completeness and validity of Taiwan's birth registry (12).
With assistance from the Bureau of NHI in Taiwan, the mothers' and infants' unique personal identification numbers provided links between the NHIRD and birth certificate data. All personal identifiers were encrypted by the NHI before release to the researchers. Confidentiality assurances were addressed by abiding by NHI data regulations. Because the NHIRD consists of de-identified secondary data released to the public for research purposes, this study was exempt from full review by the Internal Review Board.
Study sample
This study included 473 529 pregnant women with singleton live births in Taiwan between 1 January 2001 and 31 December 2003. Of these women, 16 042 had visited ambulatory care centres for treatment of migraines (ICD-9-CM code 346) within 2 years prior to index delivery. We selected only patients who had at least three consensus migraine diagnoses, because coding validity is often disputed for administrative databases. As psychiatric comorbidity has long been noted in association with migraine (13), patients with mental illnesses were not excluded, in order to have a more representative population of migraineurs. Ultimately, 4911 women with migraines were included in the study cohort.
The comparison cohort was selected from the remaining 457 487 mothers. We excluded those who had been diagnosed with certain chronic diseases (such as systemic lupus erythematosis, rheumatoid arthritis, gout, sarcoidosis or ankylosing spondylitis), but we did include those with hypertension (ICD-9-CM code 401.XX∼405.XX, 642.0X∼642.3X, 642.9X, 760.00), diabetes (ICD-9-CM code 648.0X, 250.XX), hyperlipidaemia (ICD-9-CM code 272.X), and coronary heart disease (CHD, ICD-9-CM code 410.XX∼414.XX, 429.2). We randomly extracted 24 555 mothers (five for every one with migraines) matched with the study group in terms of age (<20, 20–24, 25–29, 30–34 and ≥35 years), the year of delivery, hypertension, diabetes, hyperlipidaemia and CHD as our comparison cohort.
Variables of interest
In this study, outcome variables were all dichotomous, including LBW (<2500 g), preterm gestation (<37 weeks), babies SGA (birthweight below the tenth percentile for gestational age), CS delivery vs. vaginal delivery and pre-eclampsia. The independent variable of interest was whether a woman had been diagnosed with migraines or not.
Potential confounding factors were adjusted for, including characteristics of the mother (age, highest educational level and marital status), father (age and highest educational level), infant (gender and parity) and family monthly income. Parental age was defined as each parent's age, in years, at the time of the infant's birth. Parity was grouped into the following categories: 1, 2, ≥3. Maternal and paternal highest education levels were categorized into four levels: elementary school or lower, junior high school, senior high school, college or above. Family monthly income was grouped into four categories: <NT$15 000, NT15 000–NT30 000, NT30 001–NT50 000, ≥NT50 001.
Statistical analysis
The SAS statistical package (SAS System for Windows, Version 8.2) was used to perform the analyses. The χ 2 tests were carried out to examine differences in the characteristics of infant, mother and father for women with migraines and unaffected women. Conditional logistic regression analyses, which were conditioned on maternal age, the year of delivery, hypertension, diabetes, hyperlipidaemia and CHD, were then used to investigate the risk of LBW, preterm gestation, SGA, CS and pre-eclampsia for mothers with and without migraines, after adjusting for potential confounders. Adjusted odds ratios (OR) are presented with 95% confidence intervals (CI). A two-sided P-value of <0.05 was considered statistically significant for this study.
Results
Comparisons of pregnant women with and without migraines in relation to maternal, paternal and infant characteristics in Taiwan, 2001–2003 (n = 29 466)

The distribution of LBW, preterm birth, SGA, CS and pre-eclampsia for mothers with migraines and unaffected mothers, 2001–2003 (n = 29 466)
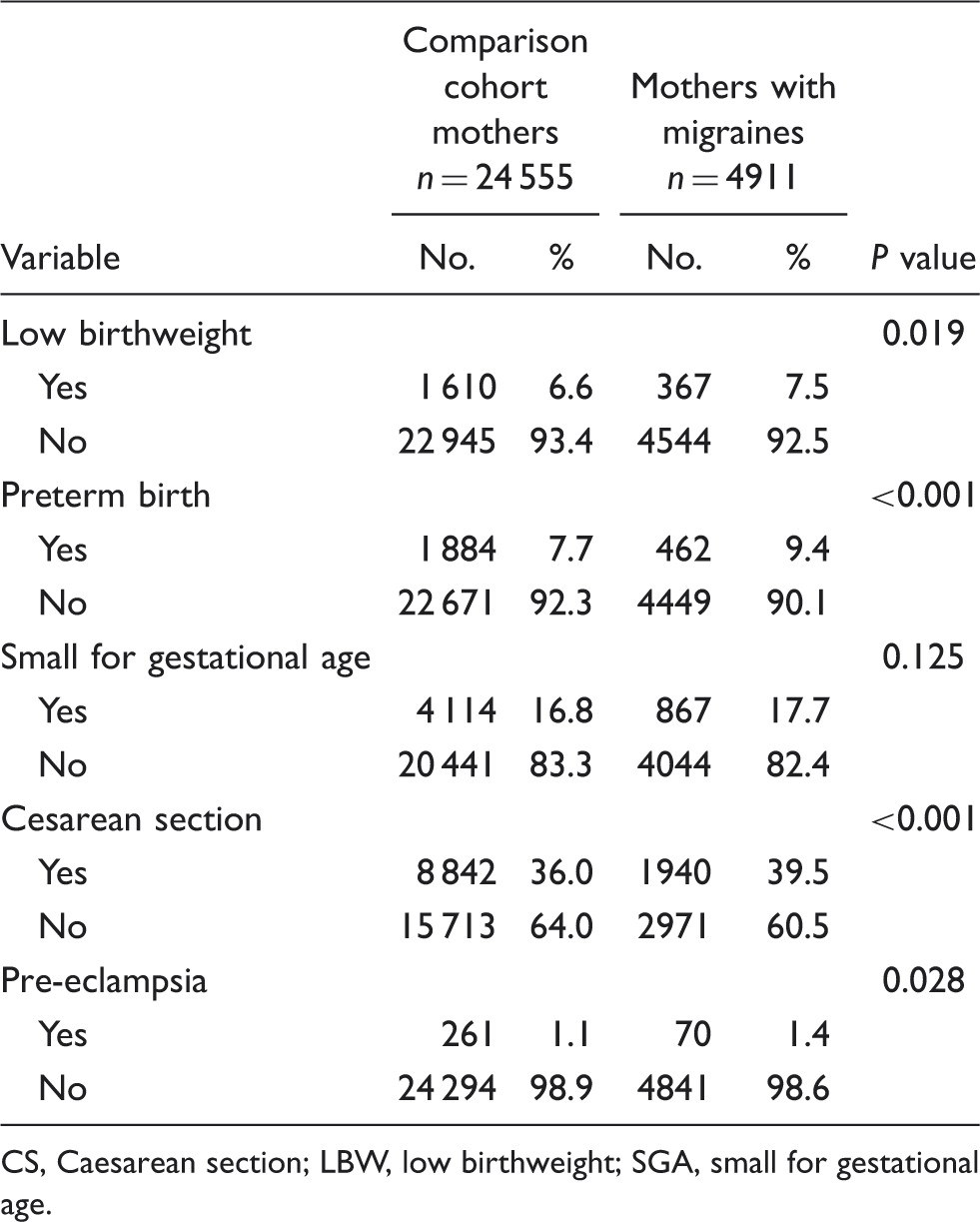
CS, Caesarean section; LBW, low birthweight; SGA, small for gestational age.
Crude and adjusted odds ratios (OR) for LBW, preterm birth, SGA, CS and pre-eclampsia among women with and without migraines during pregnancy, 2001–2003 (n = 29 466)

*Indicates P < 0.05; ***indicates P < 0.001.
Crude ORs were calculated using conditional logistic regressions that were conditioned on maternal age, the year of delivery, hypertension, diabetes, hyperlipidaemia and coronary heart disease.
Adjusted ORs were calculated by using conditional logistic regressions that were conditioned on maternal age, the year of delivery, hypertension, diabetes, hyperlipidemia and coronary heart disease and adjusted for infant's gender, parity, highest maternal education level, parental age difference, mothers' marital status and family monthly income.
CI, confidence intervals; CS, Caesarean section; LBW, low birthweight; SGA, small for gestational age.
Discussion
This nationwide population-based study clearly demonstrated that maternal migraines were independently associated with a 1.16- and 1.24-fold increased risk of having LBW and preterm babies, respectively, after adjusting for family income and maternal, paternal and infant characteristics. Women with migraines were also more likely to experience pre-eclampsia and CS, compared with unaffected women.
Our findings are consistent with 9 of 11 published studies conducted in different regions that have documented a positive association between migraines and pre-eclampsia (14). However, most previous methodologically rigorous studies were conducted among North American, Latin American and European women (15–18). This is the first study to evaluate the association between migraines and pre-eclampsia risk among East Asian women. Our findings add to the evidence supporting increased pre-eclampsia risk for women with a history of migraines and also extend the literature to include an East Asian population.
In addition, as far as we know, our study is the first to identify increased risk of LBW, preterm birth babies and CS among mothers with migraines. Although some studies have reported no increased incidence of poor pregnancy outcomes among women with migraines (10,11), these studies suffer from several limitations that could undermine the strength of their findings. For example, one recent population-based study compared outcomes for 38 151 newborns, 713 of them born to women with severe migraines during pregnancy (10). They found maternal migraines may increase the occurrence of pre-eclampsia during pregnancy, but are not associated with unfavourable delivery outcomes. Although they used the dataset of newborn infants from the Hungarian Case–Control Surveillance System of Congenital Abnormalities, the maternal information was mainly obtained from prenatal care logbooks and a structured questionnaire. Only 68% of migraines were recorded medically in the prenatal logbooks, while the rest were based on patient self-reports. Potential recall bias suggests underestimation of migraines, which clearly undermines the strength of their findings.
Similarly, in 1978, Wainscott and Volans carried out a retrospective survey at the Princess Margaret Migraine Clinic, London, UK (11). They examined pregnancy outcomes for 450 women with migraines compared with 136 controls, and found the incidence of miscarriage, toxaemia, congenital anomalies and stillbirth was not increased among the migraine sufferers compared with the national averages or the controls. However, selection bias is a possible problem with this study, because the control participation rate was much lower than the case participation rate. In addition, many studies investigating populations with migraines have been limited to small clinical samples and did not use currently accepted diagnostic criteria for migraines and pre-eclampsia; consequently there were significant methodological shortcomings.
Because the extent to which migraines affect pregnancies is not well established, this report uses a comprehensive dataset in Taiwan that provides a unique opportunity to evaluate the association between migraines and adverse pregnancy outcomes. Similar to those of previous investigations, our results further confirmed the relation between migraines and pre-eclampsia (15–18). However, unlike previous studies (10,11), our study identified increased risk of preterm delivery and LBW among women with migraines. The mechanisms by which migraines produce adverse pregnancy outcomes are complex and heterogeneous. Unfavourable foetal outcomes may relate to antiphospholipid antibodies (aPL) (19), channelopathic vasculopathy (20), and use of triptan medications (21). Further, triptans are agonists at the 5-HT1B/1D receptors that cause vasoconstriction and neuronal inhibition and they are frequently prescribed to treat acute attacks of migraine. Exposure to these drugs during pregnancy has been associated with an increased risk of preterm delivery and LBW (22).
This study has several noteworthy strengths. First, the very large sample size used provides ample statistical power to detect differences in risk of adverse birth outcomes between pregnant women with and without migraines. To the best of our knowledge, this is the most complete nationwide population-based study ever conducted to assess the risk of adverse pregnancy outcomes among women diagnosed with migraines. Furthermore, linking the NHIRD with the national birth registry leaves little room for selection and non-response bias and its robust findings can be generalized to the population as a whole. We have also incorporated increasing concern about the effects of paternal characteristics on adverse birth outcomes that may be independent of maternal effects into the study design (23). Lastly, factors such as hypertension, diabetes, hyperlipidaemia and CHD might adversely affect maternal pregnancy outcomes. Risks of cardiovascular illnesses and CHD were also associated with patients with migraine (24–26). In our study, the study and comparison cohorts were matched in terms of these conditions to better evaluate independent effects of migraine on pregnancy outcomes. Future studies need to differentiate the impact of migraine from other significant factors affecting birth outcomes.
Despite the above strengths, findings should be interpreted with caution due to the following limitations. First, because we identify mothers diagnosed with migraines by the ICD-9-CM code from the NHIRD released by the Bureau of the NHI, the sample may not accurately represent the population with migraine. Second, the validity of the migraine diagnoses could be a concern. Due to the use of a claims dataset, whether the coded migraine actually represented patients with migraine headache and whether that control did not have migraine could not be independently verified. For a variety of reasons, women may be misclassified. However, in Taiwan, the diagnosis of migraine in clinical settings is generally based upon the International Headache Society criteria (27). Further, the NHI Bureau routinely cross-checks a sample of claims from each hospital and clinic with its medical charts. It is generally believed that the NHI's cross-checks foster accurate coding. Third, with this large sample in our study, overpower might be a concern, for even small differences could be statistically significant. Indeed, some estimates in our study were small with confidence limits close to one. These results should be interpreted cautiously in terms of the meaningfulness or the clinical significance. Lastly, because the NHIRD does not include complete information regarding medications taken during pregnancy, it is not possible for us to assess the confounding role of medications in the relationship between migraines and adverse birth outcomes. However, in Taiwan, most women with migraines are reluctant to take medications during pregnancy due to concerns about adverse consequences for the developing foetus. Thus, the association between migraines and birth outcomes found in our study was largely based on women not receiving migraine treatment during pregnancy.
Although previous studies have concluded that migraines have no adverse effect on pregnancy outcomes, this study used a large, unselected national dataset to demonstrate that women with migraines were at increased risk for having LBW and preterm babies, and for delivery by CS, compared with unaffected mothers. In addition, our results, combined with reports by others, suggest that the risk of pre-eclampsia is increased in women who have a history of migraines. We suggest that clinicians should make women with migraines aware of potential risks before planning a child, coupled with more intensive monitoring and prenatal care during pregnancy. Future studies are needed to explore the association between adverse birth outcomes and migraine severity, as well as medications taken during pregnancy, to enable more specific interpretation of these findings.