
Abstract
The aim was to describe the consulting behaviour and clinical outcomes of children presenting with headache in primary care. This was a historical cohort study using data from the UK General Practitioner Research Database. Cases were children aged 5-17 years who presented to primary care with primary headache (migraine, tension-type headache, cluster headache) or undifferentiated headache (no further descriptor). Controls were age, sex and practice matched. Their records were examined for consultations, referrals, relevant treatments and specific diseases in the subsequent year. Children with headache (n = 48 575) were identified and matched to controls. At presentation, 9321 (19.2%) of headaches were labelled primary, 549 (1.1%) secondary and 38 705 (79.7%) received no formal diagnosis. Of the latter group, 2084 (5.4%) received a primary headache diagnosis in the subsequent year. Following a diagnosis of migraine, 258 (3.5%) had received a triptan and 1598 (21%) were using propranolol or pizotifen. Total consultations were higher in cases than in controls in the year before the headache: cases ages 5-8 years, mean (S.D.) 5.0 (4.0) consultations; controls 4.0 (3.5) consultations. In 1 year controls had 43 430 consultations, of which 256 (0.6%) were for headache, of whom 64 (25%) were referred to secondary care. Headache was a risk factor for benign and malignant tumours, cerebrovascular disease, primary disorders of raised intracranial pressure and depression. This risk was reduced if a diagnosis of a primary headache disorder could be made. Although there is an increased likelihood of a serious pathology with headache presentations, the risk is small particularly if a diagnosis of a primary headache is made. General practitioners are likely to be underdiagnosing migraine. This study can inform management guidelines for new presentations of headache in primary care, particularly when a secondary pathology is suspected.
Introduction
Headache is the most frequent neurological symptom and commonest manifestation of pain in childhood (1). Studies have reported annual prevalence rates in children of 3–11% for migraine (2–4) and 10–24% for tension-type headache (2, 5). The impact of headache on the quality of life of sufferers is significant both at school and at home (6). Headache has a high risk of persisting into adulthood (7) with associated physical and psychiatric morbidity (8).
The needs of adult headache sufferers are often unmet (9, 10), and this situation may be worse in the paediatric population, where sufferers are less likely to articulate their problem or seek help. However, little is understood about current practice in managing headache in children, although the importance of interventions in school and primary care settings is recognized (11, 12).
The natural history of headache in children is largely unknown. Headache can be the presenting feature of important pathology—of which a brain tumour is probably the major concern for parents, patients and practitioners (13). This concern can result in imaging studies of doubtful appropriateness, driven by non-clinical factors, including medico-legal concerns (14). Headache is also associated with other medical conditions, of which anxiety and depression are the most common (15, 16).
The objective of this study was to describe the consulting behaviour and outcomes of headache presentations of children in primary care. Our specific aims were:
To identify the proportion of primary care consultations that were for headache, the consultation rates for headache and for other problems, and the number of patients referred to secondary care.
To describe the number of headache consultations receiving a specific headache diagnosis, both at presentation and in the subsequent year.
To assess the number of patients receiving specific migraine therapy in the year following a diagnosis of migraine.
To identify important diagnoses, including brain tumours and depression, in the year after a new presentation of headache.
Ethical approval was given by the Scientific and Ethical Advisory Group of the General Practice Research Database (GPRD).
Methods
This was a historical cohort study using data from the GPRD. Doctors contributing to the GPRD record full details of patient characteristics, including all consultations and diagnoses. Data are subject to thorough validation and stringent quality checks, and have been used in many epidemiological studies (http://www.gprd.com).
Cases
These were children aged 5–17 years with a code for headache in their records, having had no other headache code in the previous year. A list of headache codes was compiled by the authors (available from them) and agreed with the GPRD. We included cases from the inception of the database in January 1987 to June 2005 who had at least 1 year of full data in their records after the index headache consultation. These cases were identified by GPRD staff and the full anonymized electronic records were extracted. The index headache code was categorized into a primary headache (migraine, tension-type headache or cluster headache) or a secondary headache—if they had a further descriptor. All other codes were classified as undifferentiated headache, i.e. headache as a presenting symptom with no further descriptor.
Controls
Each patient was matched to one control. Matching was by year of birth (to protect anonymity, dates of birth are stored only by the birth year in the GPRD), sex and practice. Controls had no record of headache during the year before the index date of their case, although they could have had a headache before or after this year. Controls also had to have at least 1 year of full data after the index date.
Data collection
Diagnoses and therapy
Libraries of codes relating to the outcomes of interest (available from authors) were created. These were for conditions recognized as potential underlying causes of headache: benign and malignant tumours, cerebrovascular disease, raised intracranial pressure (hydrocephalus or benign intracranial hypertension) and depression. The records of cases and controls were examined for the year after the index consultation of the case to identify these conditions. Undifferentiated headache records were also examined for any subsequent diagnosis of a primary headache. Cases receiving a diagnosis of migraine were examined for specific migraine treatment in the subsequent year. We identified drugs that were most likely to be used exclusively for the management of migraine. For the acute attack nasal sumatriptan is the only licensed triptan in the age groups studied; and propranolol and pizotifen are frequently used as preventative medication.
Consultation rates
All consultations in the year before and after the index consultation were counted, and categorized into headache and other consultations. Since by definition no case or control had a headache recorded in the year before the index consultation, a different year—running from 2 years before index to 1 year before index in controls—was used to estimate the percentage of total consultations in primary care related to headache.
Analysis
Differences in the consultation rates between cases and controls were assessed for significance using t-tests. Differences in subsequent diagnoses were estimated using Cox proportional hazards models. Analyses were performed using Stata version 8, 2001 (Stata Corp., College Station, TX, USA).
Results
There were 48 575 patients with a primary or undifferentiated headache satisfying our inclusion criteria. We were able to match all cases to a control.
Table 1 shows the diagnoses made at presentation, broken down into three age groups; 9321 (19.2%) had a primary headache code at their index consultation. Migraine accounted for 7468 (80.1%) of these primary headaches, the remainder being accounted for by tension headache [1565 (16.8%)] and cluster headache [288 (3.1%)]. Five hundred and forty-nine (1.1%) patients were diagnosed with secondary headache and 38 705 (79.7%) had headache that was classified as ‘undifferentiated’. The proportion with undifferentiated headache fell with age from 91.0% in the 5–8 years age group to 76.9% in the 13–17 years age group. In the year following the index consultation, 2084 (5.4%) children with undifferentiated headache were attributed a diagnosis of primary headache, 78% of which were migraine. For all age groups, consultation rates in cases and controls in the year before the index date were significantly higher in cases when compared with controls (Table 2). In the year starting 2 years before the index dates, controls had 43 430 consultations, of which 256 (0.6%) were for headache, 1.6 new headache consultations per 100 patients per year. Of these children, 64 (25%) were referred to secondary care for management of their headache.
General practitioners' diagnoses of headache

Mean consultation rate in the year before the index date
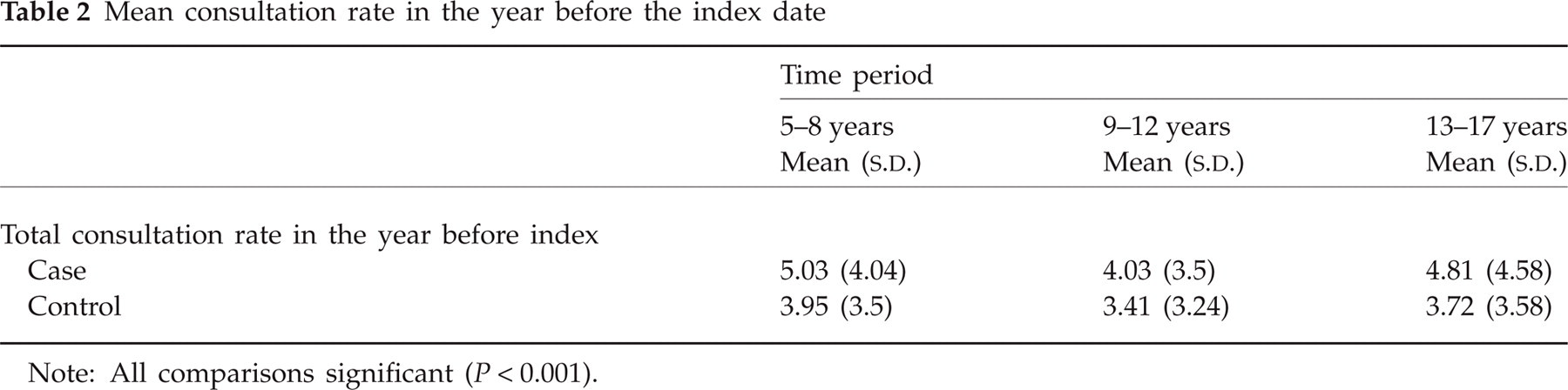
Note: All comparisons significant (P < 0.001).
Table 3 shows selected diagnoses in the year following the headache presentation compared with controls. In particular, the risk of a primary tumour in children with a headache presentation was 0.03% compared with a risk in controls of 0.004%. With a diagnosis of a primary headache, secondary pathology was identified in only 0.02%, none of whom had a primary brain tumour. The risk of subsequent depression with a headache presentation was 1.5%, over double the control rate. Most of the secondary diagnoses followed a label of undifferentiated headache. There was a marked female predominance. In patients with undifferentiated headache, 10 of the 13 malignant tumours were identified within 90 days of the index presentation.
Important diagnoses in cases and controls in year following presentation

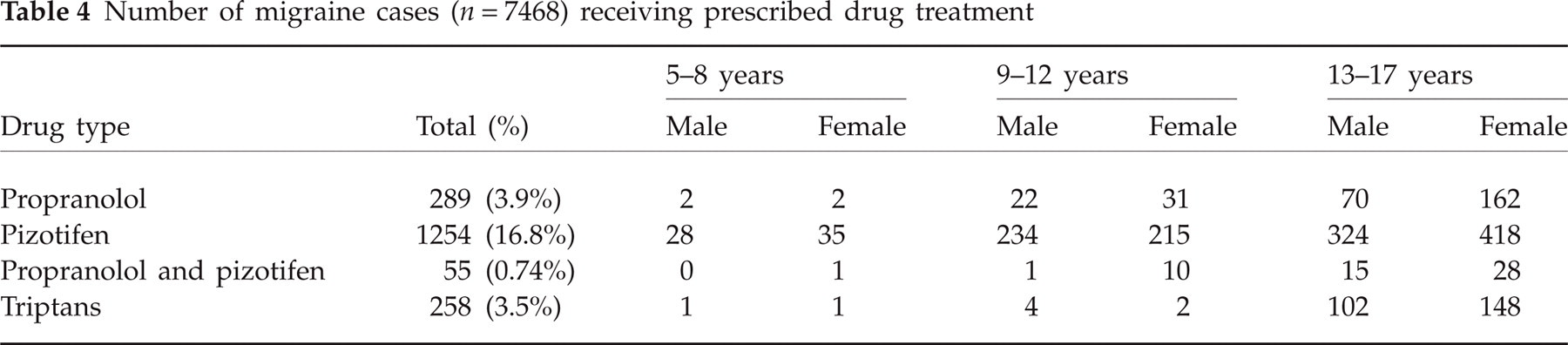
Table 4 presents the number of subjects diagnosed with migraine at presentation who were prescribed specific migraine treatment in the subsequent year; 3.5% had received a triptan and 21% of subjects were using propranolol or pizotifen.
Number of migraine cases (n = 7468) receiving prescribed drug treatment
Discussion
Main findings
For children aged 5–17 years, approximately 0.6% of general practitioner (GP) consultations are for headache; a quarter of these children are subsequently referred to secondary care. Patients presenting with a headache have a significantly higher rate of non-headache consultation than controls in the previous year. Headache was a risk factor—albeit a small one—for cerebral tumours, cerebrovascular disease, raised intracranial pressure and depression. These conditions were less common after the diagnosis of a primary headache. At presentation, 19% of headaches were diagnosed as primary and 1% as a secondary headache, but 80% did not receive a formal diagnosis. Of the latter group, 5.4% were diagnosed with one of the primary headaches in the next year. Use of specific therapies for migraine is rare; less than a quarter of the cohort diagnosed with migraine were prescribed an antimigraine agent.
Study strengths and weaknesses
An important strength of this study is that the data were collected prospectively in primary care—the setting where most patients presenting with headache are seen. The study was also large. This allowed us to identify small increases in the diagnoses of interest, when compared with control patients. However, using pre-existing data has a number of limitations. We were able to use only the headache label as recorded by the GP and not formal diagnostic criteria. Even so, GPs appeared to use the diagnoses of primary headache and undifferentiated headache for different groups: underlying diagnoses were much less likely in the former group. Finally, although we had no means of verifying the secondary diagnoses, we have no reason to believe there would be systematic differences in recording of these diagnoses between our cases and controls.
Setting our findings within the context of other literature
We identified that 1.6 new headache consultations occurred for every 100 patients per year, of whom 25% were referred to secondary care. This compares with a rate of 4.4 per 100 adult patients each year, of whom 4% are referred (17). Our consultation rate is slightly lower than data reported from two other studies of headache in children, which reported that 2–11% of children consult each year for headache. This apparent discrepancy almost certainly reflects our decision to study new cases of children presenting with headache, as opposed to all cases of children presenting with headache (18, 19).
The high numbers of headache presentations where a specific diagnosis is not made are similar to adults, where 65% of primary care headache presentations do not receive a diagnosis at presentation or in the subsequent year (20). Retrospective studies of adults suggest that 84% of headache presentations in primary care are migraine (21). As 10.6% of the UK school population are reported to have migraine (4) and cluster headache is extremely rare in the age group studied, the simplest explanation for our results is that GPs are under-diagnosing migraine. It is of importance that once diagnosed, only a quarter of children received specific therapy for migraine.
Our finding of increased total consultation rates for headache sufferers is confirmed by other studies (22) and may reflect higher levels of somatization. For example, there is an increased frequency of other pain disorders in children with headache including neck, abdominal and back pain (23–25). The increased risk of depression is well recognized. Children with headache have higher levels of anxiety and depression and demonstrate different behavioural characteristics when compared with children not having headache (23, 26). However, the interplay between headache, contextual factors and coping ability remains poorly understood and the direction of causality between headache and the comorbidities that are described remains contested (27). The risk of subsequent tumour amongst children presenting with headache of 0.03% compares with data derived from adults, where risks of 0.08% for patients < 50 years old and 0.28% for those > 50 years have been identified (28).
Conclusion
Although there are a number of limitations to our study, it is the most comprehensive undertaken to date, being based on data derived from a very large population base. Our data inform management guidelines for new presentations of headache, and reassure practitioners that the risk of a brain tumour presenting with headache is very low, particularly if a primary diagnosis of headache is made.
GPs experience difficulty in diagnosing adult headaches, and our study suggests that GPs also find difficulty in diagnosing headache in children. As simple, inexpensive and evidence-based approaches to the treatment of primary headaches in this age group are available (29), it is important to identify, diagnose and treat this common condition once more serious causes have been excluded. Qualitative research is needed to explore why GPs find difficulty in diagnosing headaches, particularly in the younger age group, and to develop strategies to facilitate its diagnosis and management. GPs should be encouraged to make a positive diagnosis in their headache patients as the first essential step to successful management.
Competing interests
None to declare.
Acknowledgements
D.K. and W.H. receive research practice funding from the Department of Health (St Thomas, Exeter, and Barnfield Hill, Exeter), and W.H. holds a NIHR postdoctoral award. Access to the GPRD was supported by an MRC licence.