
Abstract
Reversible cerebral vasoconstriction syndrome (RCVS) is characterized by sudden-onset recurrent ‘thunderclap’ headaches with reversible multifocal narrowing of the cerebral arteries, often associated with focal neurological deficits from ischaemic or haemorrhagic stroke. It has been associated with exposure to vasoconstrictive drugs, pregnancy, migraine, and a variety of other conditions. Whereas the pathophysiology of RCVS remains unclear, changes in the levels of female hormones are considered important because RCVS predominantly affects women and is frequently associated with pregnancy. We report a patient with angiographically confirmed RCVS whose MRI showed reversible brain oedema, suggesting an overlap between RCVS and the reversible posterior leucoencephalopathy syndrome. The only identified risk factor was oral contraceptive pills started 1 month prior to onset, supporting a role for female reproductive hormones in precipitating this overlap syndrome.
Over the last five decades, the phenomenon of cerebral ‘vasospasm’ occurring in the absence of aneurysmal subarachnoid haemorrhage has been documented in various clinical settings, including pregnancy and puerperium, migraine, vasoconstrictive drug use, and others (1–6). The nosology used to describe such cases has varied depending on the presumed mechanism or associated risk factor, e.g. Call–Fleming syndrome, benign angiopathy of the central nervous system, postpartum angiopathy, thunderclap headache with reversible vasospasm, and drug-induced angiopathy. Recent reviews have noted that despite the varied associations, the clinical, laboratory, imaging and pathological features of these patients are similar (7). A unifying term ‘reversible cerebral vasoconstriction syndrome’ (RCVS) has been adopted to facilitate prompt diagnosis and management and distinguish this syndrome from mimics such as primary cerebral vasculitis (7–10).
The RCVS predominantly affects women. Typical features include sudden-onset recurrent headaches with reversible angiographic ‘beading’ of multiple medium-sized cerebral arteries. Some patients develop seizures or focal neurological deficits from ischaemic or haemorrhagic strokes. Recent case reports have described transient brain oedema in patients with RCVS, suggesting an overlap with the ‘reversible posterior leucoencephalopathy syndrome’ (RPLS) (11,12). The pathophysiology of these conditions is not clear. A role for female reproductive hormones is suggested by the frequent occurrence in women and the association with conditions like migraine and childbirth. We report a woman with common migraine headaches who developed RCVS with RPLS 1 month after starting oral contraceptive pills (OCPs).
Case report
A 42-year-old woman developed a sudden, intense headache reaching peak intensity within 1 min, associated with nausea. Her past medical history included menstrual migraines, pregnancy-associated hypertension, nephrolithiasis and chronic neck pain for which she received chiropractic manipulation. There was no family history of migraine. Her only medications were monophasic combination OCPs, started 1 month previously.
Upon admission, her blood pressure was 160/90 mmHg. The neurological examination was unremarkable. Head computed tomography (CT) showed no parenchymal abnormality. With a recent history of chiropractic neck manipulation and concomitant neck pain, dissection was suspected. However, on CT angiography, no dissection was detected. Instead, mild irregularity was noted in the right middle cerebral artery (MCA). There was also an incidental finding of C6/7 osteophytes with impression on thecal sac, which probalby explained her neck pain. In view of the recent exposure to OCPs, brain magnetic resonance imaging (MRI) and MR venogram were performed to rule out central venous sinus thrombosis, and results were normal. Cerebrospinal fluid (CSF) examination showed opening pressure 19 cmHg, mildly elevated proteins (0.52 g/l, normal < 0.45 g/l), and no red blood cells or white blood cells. Her headache partially improved after treatment with paracetamol and non-steroidal anti-inflammatory drugs and she was discharged.
Ten days later, while receiving chiropractic neck manipulation, she developed a
seizure with left face and arm twitching lasting 1 min followed by loss
of consciousness. On regaining consciousness, she complained of a severe (8/10)
headache. Her systolic blood pressure fluctuated between 120 and 140 mmHg,
occasionally up to 180 mmHg. Fundoscopic examination showed multiple dot
haemorrhages, but neurological examination showed no focal deficits. In view of the
new neurological manifestation, a repeat head CT was done, which showed diffuse
occipital and parietal white matter hypodensities. To delineate the nature of the
newly developed white matter lesion, a brain MRI was performed, which showed diffuse
bi-hemispheric T1-hypointense, T2/fluid-attenuated inversion recovery-hyperintense,
non-enhancing lesions consistent with brain oedema predominantly affecting the
parietal and occipital white matter (Fig. 1A). MR venogram was again
normal. The mild right MCA irregularity noted in the initial CT angiography raised
the suspicion of a vascular component. Hence, transcranial Doppler ultrasound (TCD)
was performed, and showed elevated blood flow velocities (up to 260 cm/s) in the
right MCA, and normal flow velocities in the other intracranial arteries. A
fluorescein retinal angiogram performed 1 week after admission was unremarkable.
Complete blood count, renal, liver and thyroid function tests, erythrocyte
sedimentation rate, C-reactive protein, antinuclear antibody, anticardiolipin
antibody, lupus anticoagulant and Venereal Disease Research Laboratory tests were
normal. Electrolytes were normal except for hypokalaemia (3.0 mmol/l). Urinalysis
and urine catecholamine levels were normal. A pregnancy test was negative. Brain imaging findings. (A) Initial magnetic resonance imaging (MRI),
axial fluid-attenuated inversion recovery (FLAIR) images show bilateral
subcortical white matter hyperintense lesions consistent with brain
oedema. (B) Follow-up MRI, axial FLAIR images show resolution of the
white matter lesions. (C) Follow-up MRI, diffusion-weighted images (DWI)
show infarctions in the right caudate, corona radiata and insular
regions. (D) Initial magnetic resonance angiography shows irregular
middle cerebral arteries (arrows). (E) Initial digital subtraction
angiography (DSA) shows narrowing and dilation (beading) of the
intracranial arteries (arrows). (F) Follow-up DSA at 19 weeks shows
complete resolution.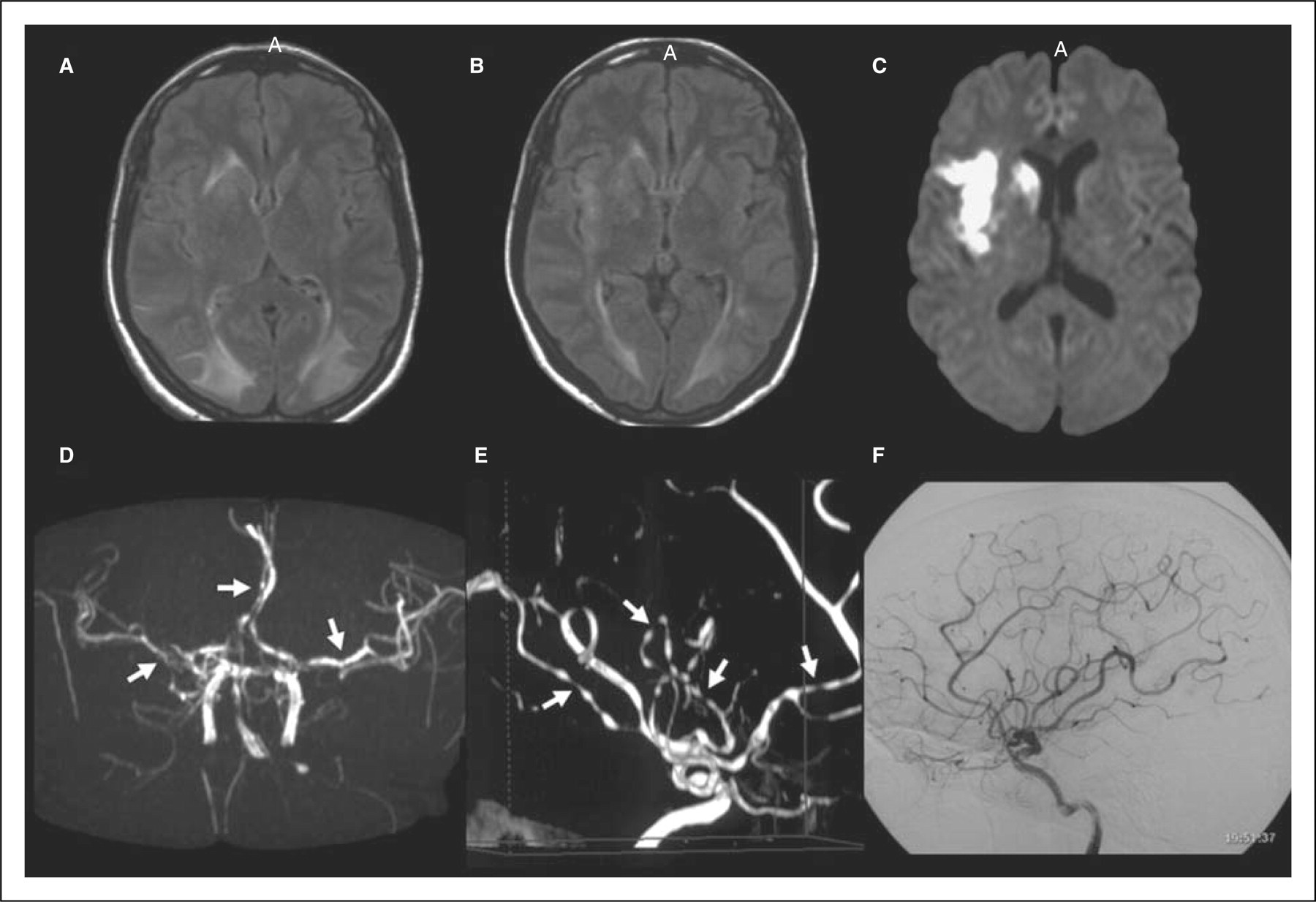
The MRI findings raised suspicion for acute disseminated encephalomyelitis (ADEM), therefore intravenous immune globulin (IVIg) and pulse methylprednisolone were initiated. Two days after starting treatment she developed sudden left hemiparesis. Brain MRI now showed partial resolution of the previously documented oedematous lesions (Fig. 1B), and new acute infarctions in right caudate nucleus, corona radiata and insular cortex (Fig. 1C). Magnetic resonance angiogram (MRA) showed irregularities in the bilateral MCAs and right anterior cerebral artery (ACA) (Fig. 1D). Repeat TCDs showed increased blood flow velocities in the bilateral MCAs and ACAs. Pulsatility index was normal. Digital subtraction angiogram (DSA) showed multifocal ‘beading’ of the right and left MCAs and their branches (Fig. 1E). A diagnosis of RCVS was considered, IVIg was stopped, and she was moved from methylprednisolone to a tapering dose of oral prednisolone. The left hemiparesis resolved completely in 3 days. Her headache gradually improved and she was discharged. When seen in follow-up after 5 weeks, her headache and TCD abnormalities had resolved completely and the neurological examination was normal. At 12 weeks, brain MRI showed complete resolution of the subcortical oedematous lesions and evolution of the known infarcts but no new lesions. MRA showed significant improvement in the arterial irregularities. MR spectroscopy showed normal N-acetyl aspartate, creatinine and choline levels in previously abnormal bilateral occipital regions. Repeated DSA performed 19 weeks after symptom onset showed complete resolution of the multifocal vasoconstriction (Fig. 1F).
Discussion
This patient's clinical features, laboratory and CSF results and serial brain imaging findings are entirely consistent with a diagnosis of RCVS with RPLS (9,11,12). As is typical with this ‘overlap’ syndrome, she developed recurrent thunderclap headaches, focal neurological deficits, reversible brain oedema and multifocal intracranial arterial vasoconstriction that was prolonged but reversible. Other causes of thunderclap headaches (13) such as carotid or vertebral artery dissection, cerebral venous sinus thrombosis and pituitary apoplexy were excluded by appropriate brain imaging studies.
The reversible imaging findings, normal CSF results and negative work-up for systemic vasculitis excluded the possibility of cerebral vasculitis, which is an important mimic of RCVS. Patients with RCVS are often treated with steroids until the work-up to exclude vasculitis is completed, because the latter condition warrants prompt immunosuppressive therapy to prevent progression. In our patient, the initial diagnostic consideration of ADEM resulted in the initiation of intravenous steroids. The patient worsened shortly thereafter, suggesting that steroids may not prevent progression of RCVS. The worsening may have been related to IVIg therapy, which has been associated with RCVS (14,15). Fortunately, these therapies were stopped soon after the diagnosis of RCVS was confirmed by DSA and her symptoms improved. Although the most appropriate treatment for RCVS is not yet established, anecdotal reports suggest that calcium channel blocker (e.g. nimodipine) may be useful in reversing the vasospasm and relieving headache (16).
The pathophysiology of both RCVS and RPLS are believed to be related to abnormalities in cerebral vascular tone (12). Supporting this hypothesis is the fact that the onset of RCVS has been temporally associated with exposure to vasoconstrictive drugs and medications. However, the only recent medication exposure identified in our patient were OCPs. Although it is possible that our patient's syndrome was spontaneous and unrelated to OCP exposure, it is important to note that changing levels of female reproductive hormones have been previously implicated in the pathophysiology of RCVS as well as RPLS due to the predominant affliction of women and the temporal association with childbirth (9). Experimental studies have shown that the cerebral arteries express specific receptors and metabolic enzymes for gonadal hormones, and that cerebral vascular tone as well as blood–brain barrier permeability is heavily influenced by the effects of oestrogen and progesterone on endothelial nitric oxide, prostanoid and other molecular pathways (17). Furthermore, there is extensive evidence supporting a role for oestrogens in migraine headaches (18). The common association of migraine with RCVS further supports the role of female hormones in the pathogenesis in RCVS. Prospective studies are warranted to clarify the role of hormones and medications in RCVS and RPLS.