
Abstract
Background
Temporomandibular disorders (TMD) is an umbrella term for pain and dysfunction involving the masticatory muscles and the temporomandibular joints (TMJs). TMD is the most common orofacial pain condition. Its prominent features include regional pain in the face and preauricular area, limitations in jaw movement, and noise from the TMJs during jaw movements. TMD affects up to 15% of adults and 7% of adolescents. Chronic pain is the overwhelming reason that patients with TMD seek treatment. TMD can associate with impaired general health, depression, and other psychological disabilities, and may affect the quality of life of the patient.
Assessment
Evaluations indicate that the recently published Diagnostic Criteria for TMD (DC/TMD) are reliable and valid. These criteria cover the most common types of TMD, which include pain-related disorders (e.g., myalgia, headache attributable to TMD, and arthralgia) as well as disorders associated with the TMJ (primarily disc displacements and degenerative disease). As peripheral mechanisms most likely play a role in the onset of TMD, a detailed muscle examination is recommended. The persistence of pain involves more central factors, such as sensitization of the supraspinal neurons and second-order neurons at the level of the spinal dorsal horn/trigeminal nucleus, imbalanced antinociceptive activity, and strong genetic predisposition, which also is included in DC/TMD.
Conclusion
The etiology is complex and still not clearly understood, but several biological and psychosocial risk factors for TMD have been identified. Several studies indicate that patients with TMD improve with a combination of noninvasive therapies, including behavior therapy, pharmacotherapy, physical therapy, and occlusal appliances. More stringently designed studies, however, are needed to assess treatment efficacy and how to tailor treatment to the individual patient.
Introduction
Temporomandibular disorders (TMD) is a collective term for pain and dysfunction of the masticatory muscles and temporomandibular joints (TMJs). Its most common features are regional pain in the face and preauricular area, limitations in jaw movements, and noises from the TMJs during jaw movements (1). The most common types of TMD include pain-related disorders (e.g., myalgia, headache attributed to TMD, and arthralgia) and disorders associated with the TMJ (primarily disc displacements and degenerative diseases) (2).
Chronic pain is the overwhelming reason for seeking TMD treatment, while TMD may also be associated with impaired general health, depression, or other psychological disabilities that affect the patient’s wellbeing and quality of life (3). TMD shares similarities with other chronic pain conditions − such as chronic tension-type headache or migraine, low back pain, and fibromyalgia − and causes much suffering for the individual (4). The economic burden on society of diagnosis and treatment of orofacial pain and TMD is high, with conservative estimates of around $100 billion a year in the US alone (5).
Definition
There are several diagnostic systems for orofacial pain/TMD (2,3,6–8).
Diagnostic criteria for the most common pain-related temporomandibular disorders.
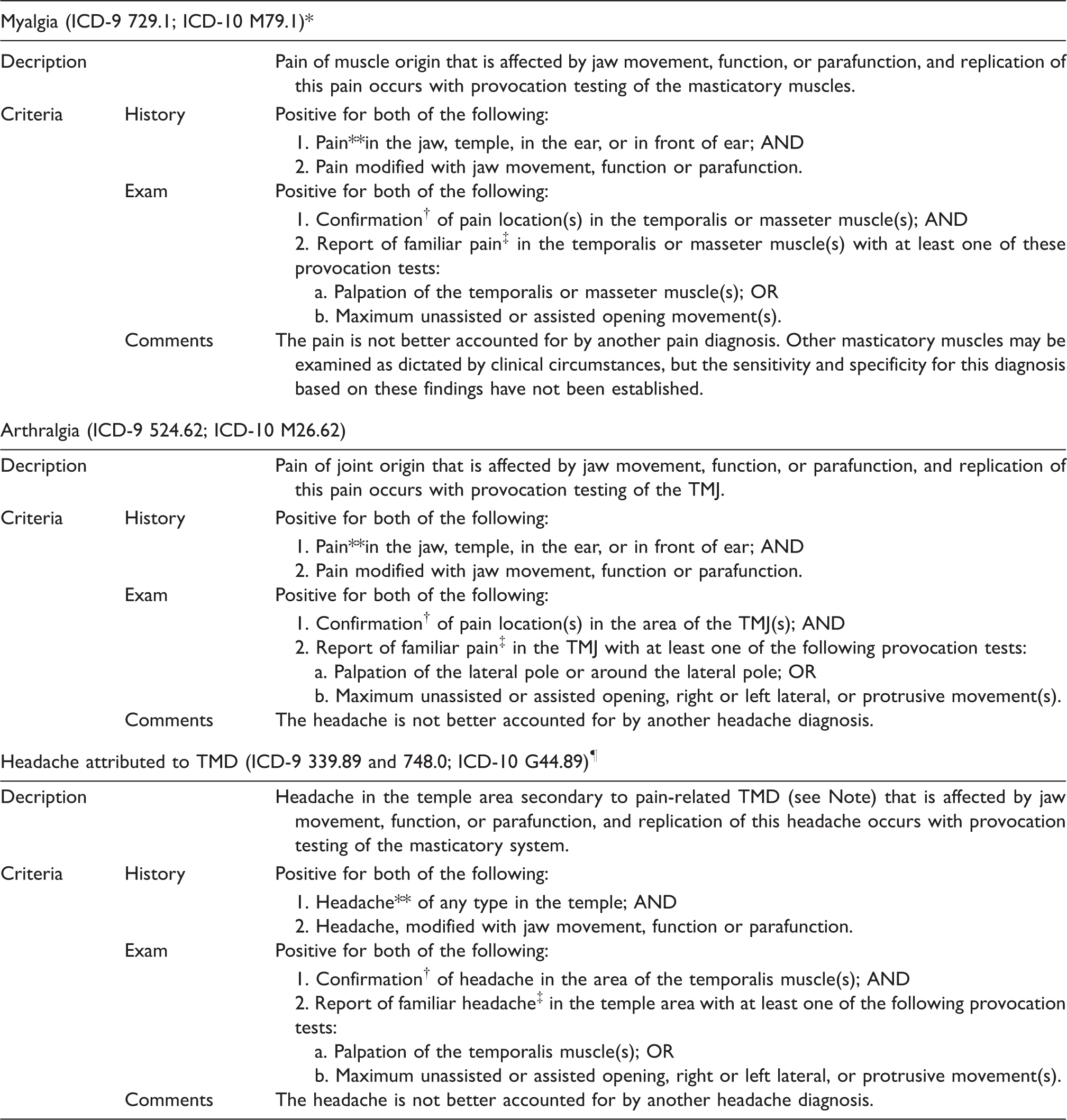
Note: A diagnosis of pain-related TMD (e.g. myalgia or TMJ arthralgia) must be present and established using valid diagnostic criteria. *ICD-9: International Classification of Diseases 9th Revision; ICD-10: International Classification of Diseases 10th Revision
The time frame for assessing pain including headache is in” the last 30 days” since the stated sensitivity and specificity of these criteria were established using this time frame. Although the specific time frame can be dependent on the context in which the pain complaint is being assessed, the validity of this diagnosis based on different time frames has not been established.
The examiner must identify with the patient all anatomical locations where they have experienced pain in the last 30 days. For a given diagnosis, the location of pain induced by specific provocation test(s) must be in an anatomical structure onsistent with that diagnosis.
“Familiar pain” or “familiar headache” is based on patient report that the pain induced by specific provocation test(s) has replicated the pain that the patient has experienced in the time frame of interest, which is usually last 30 days. “Familiar pain” is pain that is similar to or like the patient's pain complaint. “Familiar headache” is pain that is similar or like the atient’s headache complaint.
The ICD-9 and ICD-10 have not established a specific code for headache attributed to TMD as a secondary headache; ICD-9 and ICD-10 G44.89 are for “other headache syndrome” and ICD-9 784.0 is for “Headache, Facial Pain, Pain in Head”. Reproduced with permission from Schiffman et al. 2014 (2).
Validity statistics of the DC/TMD by diagnosis.

Reproduced with permission from Schiffman et al. 2014 (2).
Recommended Axis II assessment protocol for the DC/TMD.

Reproduced with permission from Schiffman et al. 2014 (2).
The strength of the DC/TMD Axis I protocol includes its reliable and valid diagnostic criteria for common pain-related disorders and intra-articular disorders (Table 2). The Axis I protocol provides standardized evaluation of subjective symptoms, contains clearly defined examination methods, and utilizes specific diagnostic criteria to interpret the clinical findings (Table 1). The Axis II protocol, a psychosocial assessment, has two options: A brief assessment and a comprehensive set of instruments for expanded assessment (Table 3). The American Academy of Orofacial Pain (AAOP) has now incorporated the DC/TMD in its Guidelines, as has the WHO in the International Classification of Diseases (ICD-11), classification of pain (6,10).
Clinical examination (Axis I) diagnostics require a patient history, including questionnaires and a structured clinical examination. A questionnaire, together with these clinical findings, provides enough information to diagnose the most common TMD conditions. Ascertaining that the pain experienced in the clinical examination is familiar to the patient has proved to be very important for excluding irrelevant pain. Likewise, the questionnaire’s timeframe “in the last 30 days” emphasizes a more clinically relevant pain that is both important to the individual and a reason why the patient is seeking care. Including these concepts in the provocation of pain – for example, through jaw movements and palpation – provides criteria to minimize false-positive findings.
Clinical assessments evaluate pain localization, jaw movement limitations (lateral, protruding, and mouth opening), movement pain, TMJ noises, and pain upon palpation of the masticatory muscles and TMJ. Written, illustrated instructions for the examination and an instructional video are available at http://www.rdc-tmdinternational.org.
Chronic pain affects cognitive, emotional, sensory, and behavioral reactions. These can, in turn, aggravate and maintain pain. Thus, it is important to assess the psychosocial situation of patients experiencing chronic pain and consider it during treatment planning and prognosis evaluation. The DC/TMD Axis II assessment of the patient's psychosocial situation and pain consequences are based on validated instruments (questionnaires) and interpretation guidelines. It includes instruments for assessing pain behavior, jaw function, and psychosocial functioning and distress (2). Table 3 shows the instruments recommended for the general practitioner (brief), and for the orofacial pain specialist (comprehensive). Studies suggest that use of these instruments in treatment planning and prognosis assessment may benefit patients (11,12).
Historical background
The first report of TMD was by a British surgeon in 1887, who published an article describing surgical management of disc displacements in the TMJ. An early and influential publication by Costen emphasized that dental malocclusions caused pain around the ear and the TMJs, but also related to other ear symptoms such as tinnitus, impaired hearing, and dizziness. In the decades following this, TMD research focused on single-factor explanations of TMD – such as the TMJ, muscle, or dental occlusion – but found little supporting evidence (9).
More recent research recognizes that TMD is not caused by a single factor but is a complex disorder with overlapping comorbidities of physical signs and symptoms, as well as changes in behaviors, emotional status, and social interactions as manifestations of general central nervous system dysregulation (18). This has led to acceptance of a multifactorial etiology and the widespread use of the biopsychosocial model of TMD pain (3). The RDC/TMD was the first classification that incorporated the biopsychosocial pain model, and it has been translated into 22 languages and has an overwhelming number of literature citations (9).
Symptomatology
The signs and symptoms associated with TMDs vary in their presentation and will often involve more than one component of the masticatory system. The three major signs and symptoms are pain, limited range of motion, and TMJ sounds. Pain is usually the main complaint, originating in the temporal area and the cheek, but also affecting the peri-auricular area. This pain is aggravated by provocation, such as chewing, yawning, or talking. The pain can be intermittent or persistent and is of moderate intensity, on average, but there are cases with severe pain intensity. Pain and tenderness upon palpation of the pericranial muscles and TMJ are the most common clinical signs and they do often coexist (14).
Other symptoms also reported include i) comorbid pain conditions such as tension-type headache (TTH), ii) neck and back pain, and iii) psychosocial distress, such as depression and anxiety (19).
Epidemiology
Reports indicate the prevalence of TMD in the population to be about 10–15% for adults and 4–7% for adolescents (20–22). Incidence reports for adults meeting a TMD-pain diagnosis were 3.9% and for self-reported TMD-pain in adolescents, 4.6% (23,24). The condition affects women more frequently than men and is most common in the child-bearing years (20–40 years), with a decrease in distribution with age (20). In adults, the sex ratio is approximately 2:1 (women:men) in population-based studies and 4:1 or more among clinical cases of TMD pain (1). There are no gender differences in children, but with increasing age during adolescence to young adulthood, the sex ratio increases to approximately 2:1 (girls:boys) (21,25).
In a longitudinal study in adults, 49% of the incident cases reported persistent pain when re-examined six months later (26). Similarly, in a longitudinal study of adolescents, 45% reported TMD pain once a week or more when re-examined 10–12 years later (27).
Risk factors
The etiology of TMD-pain is considered multifactorial, and several risk factors appear to predispose, precipitate, or prolong TMD-pain (22). These can include biological factors (e.g., sex hormones), endogenous opioid function, differences in anatomical genotypes, trauma, occlusal changes, parafunctions, and psychosocial factors (e.g., stress exposure, pain coping, stress, catastrophizing, and emotions). Maixner et al. proposed a model for how risk factors interact and contribute to the onset of TMD pain (28). An extensive National Institute of Dental and Craniofacial Research (NIDCR)-funded prospective study (the Orofacial Pain Prospective Evaluation and Risk Assessment, OPPERA) investigated several of these factors, assessing genetic and phenotypic measures of biological, psychosocial, clinical, and health-status characteristics (28). A decade later, many of these risk factors have been confirmed, but there are also new findings regarding risk factors, which we discuss in the following text (26).
Genetics
The case-control component of the OPPERA study explored genetic risk factors for TMD pain. It assessed over 350 candidate pain genes using a candidate gene panel. The study indicated an association between TMD and two genes: HTR2A and COMT (29). Smith et al. proposed the biological pathways through which genetic variations could causally interact to influence development of TMD pain (30). A systematic review supported these findings, showing evidence for an association between TMD pain and genes. However, the genes involved seem to account only for small associations with TMD pain, and they interact with other genes and environmental influences (31). The main contribution seems to be from candidate genes that encode proteins involved in the processing of painful stimuli from the serotonergic and catecholaminergic systems (31).
Hormonal factors
Since TMD pain is more frequent in females, some have suggested that female sex hormones, such as estrogen, are involved in pain modulation (32). Estrogen seems to be involved in modulating TMJ inflammation and regulating nociceptive responses in both the peripheral and central nervous systems (33). LeResche et al. reported that the periods of highest TMD-pain may be correlated with rapid periods of change in estrogen levels, whereas other studies have found a correlation between low estrogen levels and TMD pain (32). Overall, however, a systematic review found the evidence supporting the hypothesis that estrogen levels are associated with TMD to be weak (34).
Pain comorbidity
In one large population-based cross-sectional study, 83% of subjects suffering from TMD pain reported one comorbid pain condition and 59% reported at least two (35). The most commonly reported comorbid painful conditions in persons with TMD-pain are headache, neck pain, and back pain (36).
In cases with TMD pain, the majority of adults and adolescents report headache [21,37,38]. Subjects with TMD-pain were up to 8.8 times more likely to have headache compared to individuals without TMD-pain (38), and in most cases, the headache could be characterized as TTH. Likewise, headache seems to precede TMD pain in many adolescents with pain (39).
A case-control study found that adults with headache at least once a week had an increased risk of orofacial pain (OR = 3.7) (40). A cohort study for adolescents found that, for those with headache, the chance of developing TMD pain was 2.7 times higher than for adolescents without headaches (25). Another study found that adults who frequently experienced headache were more likely to present with aggravated TMD signs and symptoms than individuals with a lower headache frequency (41).
Adults and adolescents with TMD commonly report neck and back pain (39,42). Studies showed that subjects with TMD pain are 2.6–5 times more likely to have low-back pain compared to individuals without TMD pain (39,42).
Widespread pain is common among persons with TMD pain (43, 44). Most patients with Fibromyalgia Syndrome (FMS) seem to exhibit TMD pain (45). The OPPERA study also confirmed that comorbid pain conditions were an important predictor for onset of TMD pain (26). More information regarding painful and non-painful comorbidities in orofacial pain appears in Velly et al. 2014 (19).
Trauma and parafunctions
Trauma, both macro- and microtrauma, is another possible cause of TMD pain (22). Macrotrauma may occur following injuries or after prolonged mouth opening, such as during dental treatment or intubation. The OPPERA study found that trauma after prolonged mouth opening may predict onset of TMD-pain (46), but the cause-effect relationship here is still unclear. Microtrauma may occur after parafunctional habits such as bruxism (tooth clenching and or grinding), bracing the jaw, tongue thrusting, fingernail biting, or pencil/pen chewing. Bruxism has two distinct circadian manifestations: It can occur during sleep (sleep bruxism) or during wakefulness (awake bruxism) (47).
Lobbezoo et al. proposed a grading system that defines possible, probable, and definite sleep and awake bruxism (47). A large population-based cross-sectional survey found that more than 8% of respondents self-reported sleep bruxism at least weekly, while another study using objective measures (electromyography, EMG) reported a prevalence of 7% (48,49). A systematic review concluded that when self-reported bruxism determined the diagnosis of bruxism there was a positive association with TMD pain, but when stricter diagnostic criteria for bruxism were used, the association with TMD symptoms was much lower (50). The OPPERA study found that self-report of parafunction was a strong predictor of the onset of TMD (26). However, findings on the strength of the association between awake bruxism, sleep bruxism, and TMDs are inconsistent (50).
Occlusal factors
The relationship between dental occlusion and TMD has been a controversial topic in the dental community. A systematic review of population-based studies found only few and inconsistent associations between malocclusions and TMD symptoms (51). A large epidemiological cross-sectional survey of adults found similar results, with detected associations between malocclusions and clinical signs of TMD also being few and inconsistent, with no associations with functional occlusion factors (52).
Orthodontic treatment alters occlusion, which suggested considering it a risk factor for developing TMD (53,54). But a systematic review investigating TMD in relation to orthodontic treatment concluded that there was no support for the belief that orthodontic treatment may cause TMD (55). Similar results appeared in a longitudinal study investigating the relationship between orthodontic treatment and TMD, which found that orthodontic treatment neither causes nor prevents TMD (56).
Psychosocial
Individuals with TMD-related pain show higher levels of stress, anxiety, depression, somatic awareness, pain catastrophizing, and kinesiophobia compared with controls [40, 57–61]. A case-control study demonstrated that patients with TMD-pain were more likely to have higher levels of anxiety (OR = 5.1), somatization (OR = 2.7), and depression (OR = 3.5) than controls [40].
One three-year cohort study demonstrated that depression (incidence density ratio [IDR] = 3.2), perceived stress (IDR = 2.6), and mood (IDR = 3.7) increased the risk of TMD [62]. Another three-year cohort study showed that adolescents who experienced somatization (OR = 1.8,) and life dissatisfaction (OR = 4.1) had an increased risk of TMD-pain, regardless of gender and the presence of other pain complaints [25]. Studies have also demonstrated that psychological comorbidities contribute to the persistence of TMD-pain, regardless of the presence of painful comorbidities. For example, in another cohort study, depression and catastrophizing contributed to the onset and persistence of dysfunctional TMD-pain [44, 63].
In summary, several psychosocial factors can predispose a person to TMD-pain, precipitate it, or prolong it (25). The OPPERA study found several psychological variables to predict onset of TMD pain, but the most strongly associated were perceived stress, previous stressful life events, and negative affect at a three-year follow-up (64). In the individual, however, the interaction of factors may play a more significant role than one factor alone. Svensson and Kumar have proposed a stochastic model to better understand this interplay between risk factors and the development of TMD pain (65).
Pathophysiology
The exact pathophysiology of TMD is not yet clear despite multiple experimental studies, but several multifactorial models have been suggested [for comprehensive reviews please see (66–69)). There are relevant clinical overlaps between TMD and some headache conditions, especially TTH. Therefore, it is likely they have similar pathophysiological mechanisms. Peripheral and central sensitization may be important mechanisms contributing to the close association and complex relationship between TMD and TTH, as both disorders occur in similar anatomical areas and may reflect a possible impairment of descending modulatory pain pathways and the processes of referred pain. In addition, the clinical examination does not provide enough information to differentiate between TTH and TMD, as myofascial tenderness and pain are prominent symptoms of both disorders. Due to the similarities in the pathophysiology and clinical presentation of TTH and myofascial TMD, their comorbidity may arise from a lack of distinction between the disorders. These overlaps are also reflected in the current classification systems of both TMD and headache, and appear in the therapeutic strategies used to manage myofascial TMD and TTH.
The origin of pain in TMD has traditionally been attributed to increased contraction and ischemia of the masticatory muscles. However, numerous laboratory-based EMG studies have reported normal or only slightly increased muscle activity, while it seems that ischemia alone cannot induce TMD pain but can only provoke stronger TMD pain in combination with prolonged contraction and repetitive muscle work. Many human studies have consistently shown that the pericranial myofascial tissues are considerably more tender in patients with TMD than in healthy subjects, and that this tenderness positively associates with both the intensity and the frequency of TMD, just as in TTH (70–74). Moreover, infusion of hypertonic saline into the masseter muscles in healthy subjects elicits a pain that is perceived as TMD pain (75), and several studies report an increased number of active trigger points in the pericranial muscles of patients with TMD (73), supporting the presence of an important muscular component in TMD pain.
While theory originally attributed increased myofascial pain sensitivity to release of inflammatory mediators, resulting in excitement and sensitization of peripheral sensory afferents, animal and human experimental models have challenged this hypothesis, as only injections of Nerve Growth Factor (NGF) and hypertonic saline can provoke pain by themselves. Otherwise, various combinations of algesic substances, such as bradykinin, serotonin, glutamate, or calcitonin gene-related peptide (CGRP), are necessary to elicit clinically relevant pain. Concomitant psychophysical measures indicate that peripheral sensitization of myofascial sensory afferents was responsible for hypersensitivity. Nevertheless, it also seems that a clinically relevant TMD model must include several other factors. The issue of gender is also highly relevant due to the female preponderance in TMD cases. A Spanish study of 20 female patients with TMD and 20 healthy controls noted the presence of bilateral and widespread pressure-pain hypersensitivity in women with myofascial TMD, suggesting that widespread central sensitization is involved in myofascial TMD. This finding also has implications for the development of management strategies (76).
A recent German study demonstrated that sleep-associated disturbances increased muscle activity as measured by EMG, and facial pain in the morning occurred in 71% of patients with TMD compared to 13.6% in healthy controls (77). In fact, the OPPERA study found that deteriorating sleep quality predicted TMD incidence (26). Research has sought reliable diagnostic biomarkers for TMD, and interestingly, recent studies report dopamine to be markedly elevated in plasma from TMD patients (77,78), with a close correlation to pain intensity and perceived stress.
Like TTH, TMDs generally seem to occur in relation to emotional conflict and psychosocial stress, but the cause-effect relationship is not clear. As in other chronic pain disorders, psychological abnormalities in TMD can be viewed as secondary rather than primary, and depression and maladaptive coping strategies (e.g., catastrophizing and avoidance) are also secondary to the pain. In addition, depression may aggravate an existing central sensitization in both TMD and frequent headaches. Thus, there may be a bidirectional relationship between depression and TMD.
Maixner et al. have proposed a model that aims to include risk factors for the onset and persistence of TMD (28), illustrated in Figure 1.
Risk factors that contribute to the onset and persistence of TMD.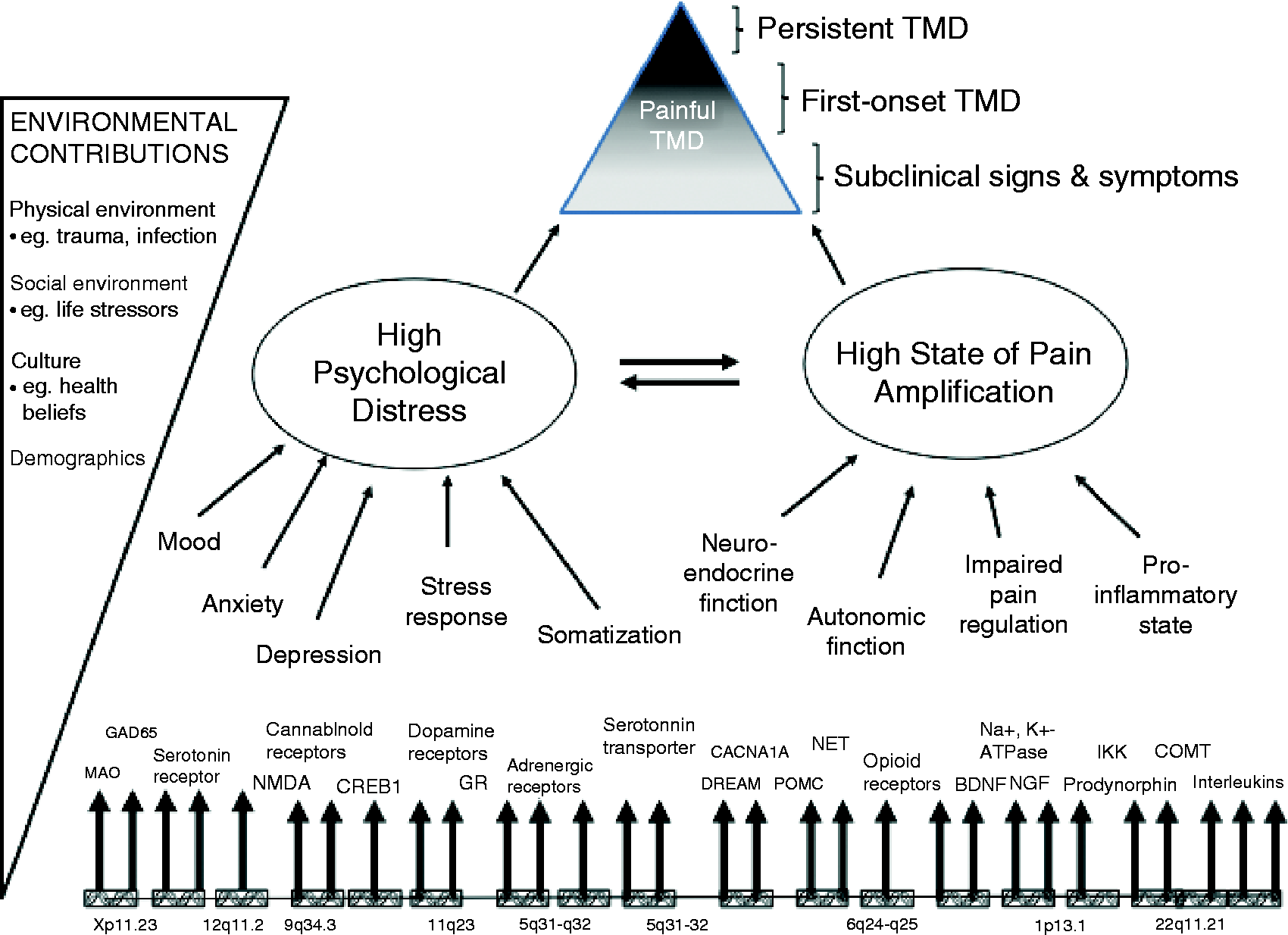
To summarize, pericranial myofascial pain sensitivity is higher in patients with TMD. Peripheral mechanisms most likely play a role in the onset of TMD, whereas more central factors such as sensitization of second-order neurons at the level of the spinal dorsal horn/trigeminal nucleus and supraspinal neurons, imbalanced antinociceptive activity, as well as genetic predisposition, drive the persistence of pain (Figure 1). Longitudinal studies will be necessary to provide final evidence for the cause-effect relationship between TMD and central sensitization.
Treatment
The treatment need for TMD in the general adult population is substantial and varies according to definition, criteria, and age. Some authors suggest that the treatment need is approximately 15% of the population (79), whereas available data indicate that only a minority of patients with TMD pain receives treatment (21). There is no single approach for treating patients with TMD. The following discusses some of the more common treatment approaches.
Reports show behavioral therapies to be effective in treating TMD (80). These therapies include counselling, education, biofeedback, cognitive behavioral therapy (CBT), habit reversal, self-treatment at home after instruction, and relaxation techniques (81,82). Systematic reviews have indicated low to moderate evidence for treatment effects, depending on which studies the review evaluated (80,82). Behavioral therapies are often an essential part of self-management programs, and the Swedish national guidelines suggest their use as a first-line therapy for TMD (83). However, further controlled trials are necessary to determine the effectiveness of these programs.
Therapeutic jaw exercises can provide coordination training, relaxation, and strengthening of the muscles. Passive stretching may improve muscle mobility and range of movement of the TMJ and, in addition, may also help patients overcome fear of moving their jaws. Jaw exercises are often part of self-care programs for patients with TMD pain (81). Evidence suggests low to moderate effects for these treatments, but more rigorously designed clinical trials are necessary (84,85).
Sensory stimulation treatment (e.g., transcutaneous electrical nerve stimulation (TENS) and acupuncture) aims to activate the afferent nervous system and thereby modulate endogenous pain control systems to promote pain relief. Acupuncture demonstrated superior pain relief in TMD and myalgia compared with no treatment, and efficacy equal to other therapies. However, compared with a placebo, results are contradictory (86). No evidence supports TENS or low-level laser in the treatment of TMD pain (82).
Occlusal appliance therapy is one of the most commonly used treatments for TMD pain, with stabilization appliances being the type most often recommended. The treatment is reversible, atraumatic, and may induce relaxation of the jaw muscles, unload the TMJ, and protect the teeth from wear due to bruxism. But the mechanisms of action have not been well studied. Studies show that wearing an occlusal appliance while asleep is likely to lead to short-term improvement, but the outcome is inconclusive compared with a placebo (non-occluding palatinal splints). Overall, there is good evidence for modest efficacy of various oral appliances in the treatment of TMD-pain (87). Patients with headache attributed to TMD reported that headache frequency and intensity decreased after treatment with stabilization appliances, but that the effect was similar to other interventions (88,89).
Studies found no evidence that occlusal adjustments (grinding on teeth) are more or less effective than a placebo in the treatment of TMD pain. All studies were restrictive in recommending the use of occlusal adjustments for treatment of TMD pain, especially since this therapy is non-reversible (90).
Systematic reviews found that non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, diazepam, hyaluronate, glucocorticoid, tricyclic antidepressants (TCAs), and antiepileptic drugs may be effective in treating TMD pain. But few primary studies were well designed with a relevant follow-up time, so results were heterogeneous and no firm conclusions can be drawn (82,91). Because of current limitations in the knowledge of pharmacologic effects on TMD pain, it is only possible to make comparisons between similar pain conditions such as backache or TTH. In several chronic pain conditions, acute drugs (e.g., analgesics and opioids) and preventive drugs (e.g., antidepressants and anti-epileptics) seem effective in relieving pain (92); thus, these drugs would probably be effective for TMD pain.
A recent study tested a stepped pharmacotherapeutic protocol and demonstrated a good response in persistent myofascial pain, even in more severe cases. Patients who did not respond to TCAs may represent a distinct subgroup for whom gabapentin, at a lower dose than previously reported, may be a good alternative (93).
Preventive drugs are always preferable for persistent TMD pain, as the benefits of acute drugs must be weighed against possible adverse and toxic effects and the risk of dependency. The potential risk of medication overuse is particularly significant for headache, as these patients have a very high incidence of comorbid primary headaches, so it is important to limit the use of all types of acute analgesics to a short period of time and to a maximum of two to three days a week.
A systematic review of surgical treatment of the TMJ concluded that arthroscopic surgery, arthrocentesis, and physical therapy all had similar effects on reduction of mandibular pain intensity and functioning (82,94). Success rates were often high, independent of treatment mode, but long-term follow-up studies are lacking. Many of the RCTs included in the systematic reviews had low quality scores and outcome measures were often coarse, which made data difficult to interpret. A majority of patients with painful disc displacements have been found to respond favorably to conservative treatment modalities. Therefore, surgical TMJ approaches are only appropriate in select patients who have been refractory to conservative treatment for at least six months and suffer from severe disability related to conditions in the TMJ (83).
Clarify the clinical and pathophysiological overlap with myofascial pain and TTH. Produce a uniform set of diagnostic criteria for TMD to be used by all professionals. Are there sensitive and specific diagnostic markers for TMD? What are effective treatment strategies to prevent chronification?
Develop and implement aligned diagnostic criteria for TMD and headache. Develop and implement aligned diagnostic instruments for Axis 1 and 2 for both TMD and headache. Tailor and test better treatment strategies for TMD and headache. Adopt a multidisciplinary approach with a team of orofacial pain specialists and a neurologist (headache specialist) for the most precise differential diagnosis possible and initiation of the best and most efficient multimodal treatment. Build closer collaborations between animal and human experimental pain models.
Conclusions
Chronic TMD is a complex musculoskeletal disorder with multifactorial etiology. Physical, behavioral and emotional factors overlap and interact in TMD. Therefore, an approach based upon a biopsychosocial illness model is recommended in the diagnosis and treatment of TMD pain.
Article highlights
Chronic TMD is a complex musculoskeletal disorder with multifactorial etiology. A biopsychosocial illness model is recommended in the diagnosis and treatment of TMD pain.
Footnotes
Author contributions
Both authors contributed to the analysis, draft, and revision of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.