
Abstract
Fungus balls are a non-invasive form of fungal infection involving the maxillary sinus in most cases. Sphenoid sinus fungus balls (SSFB) are rare and their clinical presentation is not well described. We intended to define the clinical presentation of sphenoid fungus balls, and retrospectively reviewed 24 cases of SSFB seen at our institution over a 10-year period, identified through pathological reports. Presenting symptoms were separated into three groups: headache, rhinological and asymptomatic. Headaches were subdivided into acute and chronic, unilateral and diffuse. Radiological clues leading to diagnosis were reviewed. Prognosis was determined from medical files or by phone calls. Sixty-seven per cent of patients were female. The mean age at presentation was 65 years. Sixty-two per cent presented with headache, 36% unilateral, mainly in the first trigeminal branch territory. Rhinological symptoms were seen in 21%. In 16% of patients the SSFB was asymptomatic and found during routine tests. SSFB, even if noninvasive, did lead to recurrent bacterial infections and central nervous system complications in three patients. Of 15 patients presenting with headache, 10 were significantly improved post surgery. The prognosis is good, with no recurrence of fungal infection after a main follow-up of 2.3 years. Our study underlines that SSFB present with headaches, often unilateral and in the fronto-orbital region. Proper imaging of the sphenoid sinus is useful in patients with unexplained headache. The neurologist has to be aware of radiological clues suggesting fungal sinus infection, since surgery is the main treatment, with good prognosis and frequent resolution of headaches.
Introduction
Isolated sphenoid sinusitis is rare, and in 10% of cases it is caused by fungal infection (1). Fungal sinusitis has been classified in invasive and non-invasive forms, based on the presence or absence of hyphae in adjacent mucosa. Each group is subdivided into two subcategories, fulminant and chronic for the former, and fungus ball (previously called aspergilloma or mycetoma) and allergic for the latter (2). Invasive forms can be clinically severe, with neurological complications such as meningitis, thrombosis of the adjacent cavernous sinus and intracranial extension (3). They are more frequent in immunosuppressed patients. In these cases, neurological signs mandate a thorough investigation usually leading to the diagnosis. Non-invasive forms are more frequent in immunocompetent older women. Symptoms are rhinorrhoea, nasal congestion, post-nasal drip, cough, headache or facial pain (4–6). Asymptomatic cases are described, but rare. Neurological signs are often absent, although visual disturbances have been reported. Characteristic computed tomography (CT) scan findings include opacification of the sinus with a hyperdensity in its core, osteosclerosis and osteolysis (7–9). Fungal sinusitis affects more frequently the maxillary sinus, but in 10–25% it affects the sphenoid sinus, unilaterally (2). Two series of sphenoid sinus fungus balls (SSFB) have been published. One by Klossek et al. described rhinological symptoms in 10 patients, with or without headache (10). More recently, Bowman also mentioned headache as a presenting symptom (11). Isolated sphenoid sinusitis, independently of the cause, is said to present with headache in 85% of cases, with different locations including frontal (43%), vertex (33%), occipital (25%) and temporal (16%) (12).
We describe a retrospective set of patients who were operated for sphenoid sinusitis, and in whom the diagnosis of fungal infection was proven by pathological examination. Symptoms leading to investigation are reviewed and radiological findings detailed.
Methods
Cases were identified through a review of histological specimen classified as sphenoid aspergillomas in our institution between 1998 and 2008. Twenty-seven cases were reviewed. One case was excluded because it was invasive, one because the pathology was finally negative for fungus despite typical appearance of the specimen macroscopically, and one was excluded because of insufficient available clinical data. Medical files were reviewed for clinical details. All cases had a pre-operative CT scan. Available CT scans (N = 12) were reviewed by the same radiologist (J-P.G.) to examine specific clues for fungal infection. Twelve films were not available for review, so radiological reports were used. Six patients had magnetic resonance imaging (MRI). All patients underwent endoscopic sphenoid sphenotomy, although in some patients complications justified more extensive interventions. Specimens were systematically sent to pathology for analysis. Pathology reports of mucosal biopsy to evaluate invasion were available for 15 patients. Patients were contacted by telephone for a brief questionnaire about their clinical evolution.
Results
Sixteen patients (67%) were female, and mean age at surgery was 65 years (range 36–89 years). All patients were considered to be immunocompetent. Three patients were diabetic, two had rheumatoid arthritis, one was treated with non-steroidal anti-inflammatory drugs (NSAIDs), the other with low-dose prednisone. Two were on chronic NSAIDs for ankylosing spondylitis and chronic lumbar pain. One patient was homeless and the bearer of a sickle cell anemia. Epidemiological data and prior medical history are summarized in Table 1.
Epidemiology and comorbidities of sphenoid sinus fungus ball patients

NSAID, non-steroidal anti-inflammatory drugs; RA, rheumatoid arthritis.
Symptoms leading to investigation are summarized in Table 2. They were either headache (n = 15) or rhinological complaints (n = 5). Headaches were separated into acute (days to 3 months, n = 3) and chronic (> 3 months, n = 12) groups. The localization of headache (Fig. 1) was unilateral in eight patients, with predominance of the fronto-orbital or fronto-temporal region. In four patients the headache was diffuse. In one patient there was a diffuse headache with unilateral paroxysms. Rhinological symptoms were posterior rhinorrhoea, cough, nasal discharge and expistaxis. Finally, in three patients, the diagnosis of aspergilloma was unexpected, occurring during work-up for breast cancer, pulmonary aspergillosis and spondylodiscitis. No neurological or rhinological associated symptoms were described in these patients. In one patient, the diagnosis was made during a work-up for recurrent for Escherichia coli meningitis, with five episodes in a 1-year period.
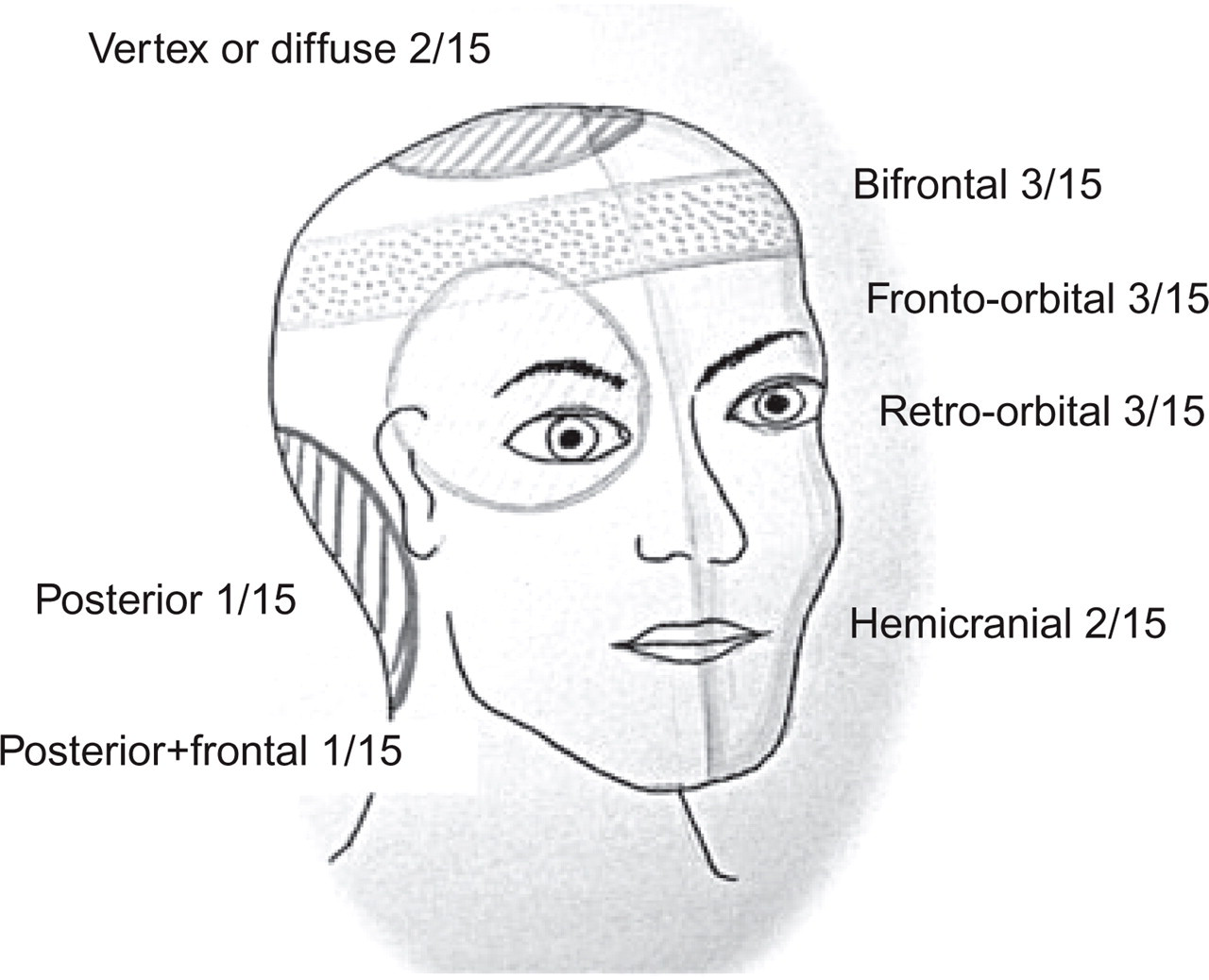
Localization of headache (15 patients).
Symptoms leading to investigation

Imaging studies
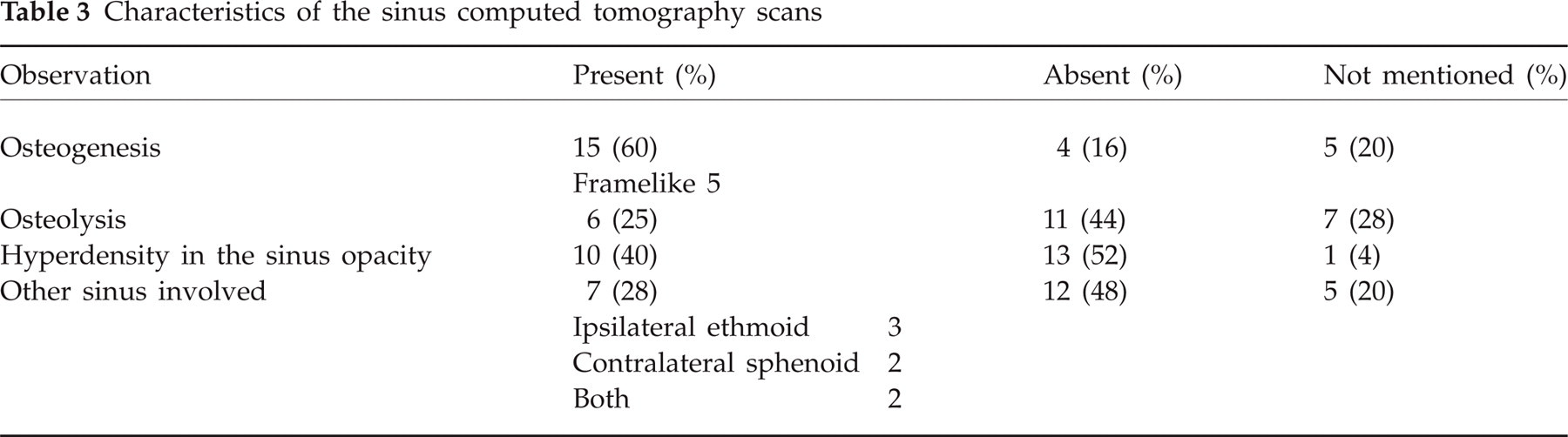
CT scans of sinuses with bone windows were performed in all patients. Available films (12/24) were reviewed by a radiologist (J-P.G.) to systematize the search for precise clues. If original films were unavailable, the radiology report was used. Partial or total opacity of the sphenoid sinus, involvement of another sinus, intrasinus hyperdensity, bone lysis or erosion, bone sclerosis or osteogenesis, frame-like appearance, were looked for; findings are summarized in Table 3. Opacity of the sphenoid sinus was described in all patients but one, lysis of adjacent bone in six, intracavity hyperdensity with a foreign body appearance in 10, and osteogenesis or sclerosis of the adjacent bone in 15. Figure 2 shows the sinus opacity with small hyperdensities and osteosclerosis of the bone wall. MRI were performed for six patients, mostly in complicated cases in search for complications. In one case the MRI (performed for a pituitary tumour work-up) suggested the diagnosis of SSFB, but the CT scan confirmed the diagnosis by showing hyperdensities.

Computed tomography scan of the sinuses. Axial view of sphenoid sinus showing opacity, small hyperdensities (white arrow) and osteosclerosis (black arrow) of the bone wall.
Characteristics of the sinus computed tomography scans
Evolution
Patients presenting with headache were contacted by telephone. Thirteen patients were successfully contacted. Mean follow-up was 2 years 3 months, range from 7 years to 2 months. Significant improvement of headache was seen in 10/15 patients, even in chronic cases (Table 4). Of the five remaining patients, two could not be interviewed, one had a stroke 6 months later with cognitive deficits precluding evaluation, one had persisting diffuse headache with medication oversuse headache, and one had persisting neuropathic pain related to a bone flap. A second functional endoscopic sinus surgery (Table 5) was done in five patients, for recurrent bacterial infections (n = 5) and suspicion of recurrence of SSFB on the control CT (n = 1), which was not confirmed. One patient had a bone flap done because of empyema. In summary, there was no recurrence of fungal infection. Despite the age of the patients, there was no mortality due to surgery or complications of the SSFB.
Detailed symptoms of headache patients and prognosis after surgery

N/A, not available; MOH, medication overuse headache; HA, headache.
Surgeries performed after the first sphenotomy

Histology
Macroscopically, the appearance of the fungus ball was usually of a clay-like, cheesy mass of a greenish or brownish colour, hence the French name ‘truffe’, which means truffle. A picture is presented (Fig. 3). Typical branched hyphae were seen on all pathological specimens. Mucosal specimens were negative in 12, insufficient in two, and equivocal with suspicion of a few hyphae in one patient. There was no pathological analysis of the mucosa in nine patients, none of them with a complicated evolution.

Photography of the fungus ball, or truffle.
Discussion
Our cohort confirms the older age [mean age and female predominance (16/24)] of SSFB patients.
Presenting symptoms can be headache or rhinological symptoms, but a significant number of patients were diagnosed during an investigation for a non-neurological or rhinological problem. Although some patients presented with diffuse pain, the pain was unilateral and in the first trigeminal territory in the majority of cases. This challenges the concept that headaches in sphenoidal disease are located in the vertex (13). Our observation reflects well the anatomical data, since sphenoid sinus is innervated by the first and second branches of the trigeminal nerve, via the nasociliary and sphenopalatine nerves, respectively. Rhinological and neurological symptoms were not described together. It has not been possible, considering the retrospective aspect of the study, to verify if presenting headaches were tension-type, migrainous or trigemino-autonomic type according to ICHD-II criteria. One patient spontaneously reported lid oedema and lacrimation ipsilaterally. Two case reports have mentioned SSFB presenting as cluster headache (14, 15).
SSFB can cause significant complications. Even when the aspergillus itself is not invasive (as proven by the negative mucosal biopsy specimens in our patients), the fungus ball can be the site of infection with a bacterium, causing bacterial sinusitis, meningitis and empyema. It is not clear whether there has to be lysis of the bone to allow entry of the bacteria in the epidural then subdural space, or if arterial or venous entry is possible.
Radiological clues were present in all patients. This is due in part to a reference bias, since CT scans result lead to diagnosis and surgery in all cases. A differential diagnosis has to be kept in mind, including bacterial sinusitis, mucocoele, malignant tumour or metastasis (16). Metal-dense hyperintensities are considered very suggestive of fungal infection, and could be caused by the presence of iron or manganese in the fungus ball. Osteogenesis was more frequent in our series than hyperdensity (60% vs. 40%). There has been questioning about the sometimes impressive osseous changes seen in non-invasive cases. The underlying pathophysiology is not known, but a local inflammatory reaction caused by the fungus ball has been proposed by Bowman. Some authors have even suggested a category of destructive/non-invasive to describe this situation (17). MRI is not helpful in the diagnosis. Bone is not well seen on MRI, and both air and fungus ball are hypointense on T2 images, which does not help to clarify the content of the sinus. Hyperdensities seen on the CT are not easily identified on MRI. MRI can be performed to rule out another cause of the headache, or to evaluate complications. Cultures were not detailed in this study because they were not performed on a routine basis. Fungal cultures are known to be frequently negative, even when pathology shows abundant hyphae (2).
The prognosis was good overall, with resolution or significant improvement of the headache in 10/15 cases. No fungal recurrence was seen.
Conclusion
SSFB present most frequently with headache, chronic or acute, and mainly in first trigeminal branch territory, often in older patients. Surgery can be curative, and is mandatory considering the risk of infection and neurological complications, especially in frail patients. Fungal infection should be suspected in any isolated abnormality of the sphenoid sinus. Radiological clues suggesting a fungus ball are intrasinus hyperdensity, and osteogenesis or lysis of the bone wall. Adequate imaging of the sinuses with bone windows is important in the work-up of headache. Neurologists have to be aware of the clinical presentation of SSFB, since a referral to an ENT surgeon can lead to curative surgery in at least two-thirds of patients.