
Abstract
Photophobia is an important criterion for the diagnosis of migraine. However, several Asian epidemiological surveys about migraine have shown lesser prevalence of photophobia than that of Western studies. This discrepancy is probably caused by underestimation of photophobia due to inappropriate questioning of patients by physicians. To investigate this issue, we developed a questionnaire about photophobia and evaluated its usefulness in 103 patients with migraine. In phase 1 of the study, we found good repeatability of the questionnaire with a 0.826 k coefficient. In phase 2, the prevalence of photophobia from interviews and that from the questionnaire were compared. The prevalence of interview-documented photophobia was 51.5% and of questionnaire-documented photophobia 82.5% (P < 0.001). In phase 3, we attempted to make a short-form questionnaire with the same detection power of the questionnaire study. Two short-form questionnaires were identified as a useful method for detecting photophobia. The prevalence of photophobia could be underreported via interview, especially in Asian migraineurs. Using this questionnaire to test for photophobia, the diagnostic rate of photophobia and migraine could be improved.
Introduction
Photophobia, an intolerance of the eyes to light, is usually associated with eye disease, migraine and various other diseases (1). As photophobia is a subjective symptom, diverse manifestations are reported, including light-induced glittering or glare, hypersensitivity to light and light-induced painful sensation (2). Photophobia has been reported in up to 90% in migraineurs during attacks (3–5), and some migraine attacks could be induced by photic or visual stimuli such as sunlight, flickering of light or a simple striped pattern (6–8). According to the International Classification of Headache Disorders, 2nd edn (ICHD-II), diagnosis of migraine requires at least one of following associated symptoms: (i) nausea or vomiting or (ii) photophobia and phonophobia (9). ID-Migraine, a simple and useful method for primary physicians to diagnose migraine, also includes a question about photophobia: ‘Does light bother you (a lot more than when you don't have headaches)?’ (10, 11).
Headache specialists as well as primary physicians should ask patients about photophobia as it is an important factor in the diagnosis of migraine. However, the sensitivity of simple questions in detecting photophobia in migraineurs seems debatable (12). Several migraine epidemiological studies performed in Asian countries have shown that the prevalence of self-reporting photophobia was lower (35–60%) than that from previous Western studies (74–88%) (13–18). Although those studies did not attempt to explain the cause of the difference, it may be related to any cultural or language differences.
To develop a more sensitive and useful questionnaire for the detection of photophobia in migraineurs, we listed eight possible questions that are commonly used during patient interviews to diagnose unpleasant light-related symptoms during a headache. We investigated the sensitivity of the eight questions in detecting photophobia and compared it with the sensitivity of the simple question in ID-Migraine. The most sensitive question among the eight questions was additionally investigated.
Methods
This study was conducted at the Headache Clinic of Korea University Medical Centre from March 2006 to May 2007. During this period, we included patients who were newly diagnosed with migraine or probable migraine according to ICHD-II (9). Exclusion criteria was as follows: (i) patients who declined to participate; (ii) patients who were illiterate; (iii) patients who had known ophthalmological diseases including cataract, glaucoma and other inflammatory eye disease; (iv) patients already diagnosed with migraine due to the possibility that these patients might be biased through education; and (v) patients with chronic migraine. A total 103 patients participated. Interviews were conducted by a single headache specialist (K.O.) at an out-patient headache clinic. For detecting photophobia during the interview, we asked the same question as included on ID-Migraine survey: ‘Does light bother you (a lot more than when you don't have headaches)?’. After this question, the participants were asked to complete the photophobia questionnaire.
Questionnaire
The questionnaire included eight questions about photophobia during a migraine attack (Q1–7) and headache-free period (Q8). The ictal questions (Q1–7) were about simple glittering sensations (Q1 and Q2), avoiding behaviours (Q3 and Q4), and painful photophobic symptoms (Q5 and Q6). The last ictal question (Q7) questioned whether the photic stimuli could induce a headache or not (Table 1). If a patient answered ‘yes’ to at least one of the questions from Q1 to Q7, we concluded that the patient had photophobia during migraine attacks.
Questionnaire for photophobia—Korean and English versions
Phase 1
For establishing the reliability of the questionnaire, test–retest reliability was evaluated using κ coefficient. We repeated the questionnaire 2 weeks following the completion of the initial questionnaire in 19 patients who had enrolled at the beginning of the study.
Phase 2
We compared prevalence of photophobia reported in the interview in response to the simple question from ID-Migraine with the prevalence of photophobia in the questionnaire for all 103 patients. The prevalence difference between the simple interview and the questionnaire was analysed using the McNemar method.
Phase 3
We intended to make the short-form questionnaire with same sensitivity power for the detection of photophobia in the clinical diagnosis of migraines. The sensitivity of each single question of the questionnaire was compared with that of the whole questionnaire. We made eight sub-questionnaires comprising three questions, one each from the three categories: simple glittering sensations (Q1 and Q2), avoiding behaviours (Q3 and Q4) and painful photophobic symptoms (Q5 and Q6). The eight sub-questionnaires were as follows: Q135 (Q1+Q3+Q5), Q136 (Q1+Q3+Q6), Q145 (Q1+Q4+Q5), Q146 (Q1+Q4+Q6), Q235 (Q2+Q3+Q5), Q236 (Q2+Q3+Q6), Q245 (Q2+Q4+Q5) and Q246 (Q2+Q4+Q6). The prevalence of photophobia from these subgroups of questions was compared with that of the whole questionnaire. The prevalence difference was tested using the McNemar method.
Results
The mean age of the participants was 38 ± 15.8 years (range 14–72). Seventy-eight patients (75.7%) were women. Eighty-four patients were diagnosed with migraine without aura (including eight patients with probable migraine without aura) and 19 were diagnosed with migraine with aura (including three patients with probable migraine with aura). Demographic features of patients are listed in Table 2.
Clinical features of the participants

Phase 1
Test–retest reliability of the questionnaire was 0.826 (κ coefficient). The reliability of each question ranged from 0.678 to 1.000 (κ coefficient) (Table 3).
The positive rate to interview and each item of the questionnaire

∗The interview-documented photophobia means positive answer to the question, ‘Does light bother you (a lot more than when you don't have headaches)?’.
†Questionnaire-documented photophobia means answering positively at least one question from Q1 to Q7.
Phase 2
The prevalence of interview-documented photophobia was 51.5% (53/103) and of questionnaire-documented photophobia 82.5% (85/103) (P < 0.001) (Table 3). All patients with interview-documented photophobia answered ‘yes’ to more than one of the seven questions (Q1 to Q7) in our questionnaire. When the prevalence rates of photophobia for each question were compared with interview as a whole, two questions about glittering sensation (Q1 and Q2), one question about avoiding behaviour (Q3) and two questions about painful photophobia (Q5 and Q6) showed similar prevalence rates. Thirty-two (31%) patients also had photophobia during headache-free periods (Q8).
Phase 3
Comparing the result of the eight subgroups with that of whole questionnaire, two subgroups (Q1+Q3+Q5 and Q2+Q3+Q5) were identified as showing the same statistical power of detection of photophobia as the whole questionnaire (Pearson's correlation coefficient ranges from 0.883 to 0.835). All patients with interview-documented photophobia also answered ‘yes’ in these two subgroups. Detailed statistical analysis is illustrated in Table 4.
Comparison of the sensitivity between the whole questionnaire and short-form questionnaire
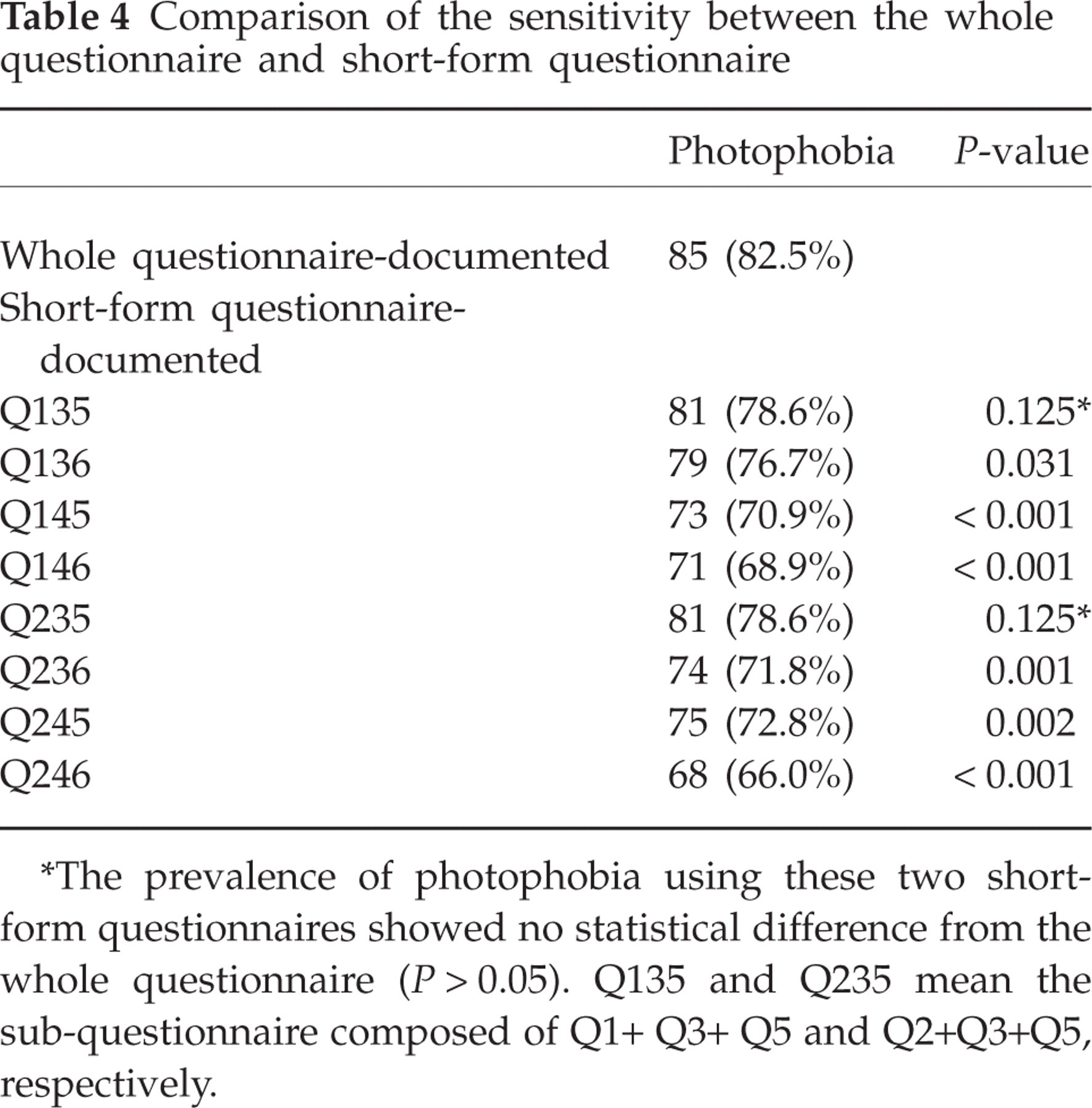
∗The prevalence of photophobia using these two short-form questionnaires showed no statistical difference from the whole questionnaire (P > 0.05). Q135 and Q235 mean the sub-questionnaire composed of Q1+ Q3+ Q5 and Q2+Q3+Q5, respectively.
Discussion
From this study, our questionnaire for photophobia seems to be a sensitive and reliable tool for detection of photophobia among patients with migraine. The present study shows that use of this questionnaire can improve the detection rate of photophobia when compared with interviews using the single question from the ID-Migraine. Some subgroups composed of three questions are also sensitive at rates compatible with the whole questionnaire.
Photophobia, as an intrinsic property of migraine, is essential its diagnosis, but it has been unclear how to assess the presence of photophobia (19). During interviews, individual physicians are more or less effective at detecting photophobia because they each use different questions. According to previous large-scale epidemiological studies, many different questions have been used to identify ictal photophobia. However, a standard question about photophobic symptoms for migraine diagnosis did not exist until ID-Migraine was proposed. However, the ID-Migraine has only a single question regarding photophobia (10, 11). Since this question is about vague and subjective feelings, there is a possibility that patients who are hypersensitive to light in different ways answer negatively to this question. Consequently, this bias could result in underestimation of photophobia and decreased sensitivity of migraine diagnosis.
Phase 1 of our study showed that our questionnaire has good repeatability (κ 0.826). This report is the first to show the repeatability of a questionnaire for photophobia. This questionnaire includes eight questions that can be easily understood and answered.
Phase 2 has shown that the sensitivity of the questionnaire for detecting photophobia (82.5%) is higher than that of interview (51.3%). The questionnaire is superior at detecting photophobia when compared with a simple interview (P < 0.001). Positive response rates for each of the two questions about glittering sensation (Q1 and Q2) and painful photophobia (Q5 and Q6), in addition to a question about avoiding behaviours (Q3), were similar to those of an interview using the question of the ID-Migraine. These findings reflect the fact that photophobia could manifest differently in different migraineurs and could be easily missed by a single item during an interview. This issue was also noted by a study of Evans et al., which showed underreported photophobia and phonophobia during simple interview and suggested a need for a more detailed, close-ended question about these associated symptoms of migraine (19). When we considered the results, our questionnaire determined photophobia more sensitively. In this study, of 11 probable migraineurs, eight were reclassified as definitive migraineurs when using our questionnaire. Although we could not perform statistical analysis because the number of patients diagnosed as probable migraineurs was small, it seems that we could diagnose migraine more easily using this questionnaire.
It has been suggested that glittering sensations including glare, dazzle, flicker and pattern glare might also be attributed to hypersensitivity to visual stimuli in migraineurs (20–22). Moreover, it has been shown that migraineurs avoid light by wearing sunglasses, turning off the lights or drawing a curtain (8, 20, 21) and are more vulnerable to visual stimuli not only during attacks but also during interictal stages (20, 23, 24). Our study has demonstrated that a simple glittering sensation (Q1 and Q2) is the most common photophobic symptom in migraineurs and about one-third of patients have interictal photophobia (Q8, 31%). About the question regarding the avoidance of behaviour during a headache, our patients preferentially answered that they turn off the lights or draw a curtain (Q3). On the other hand, our patients are unlikely to wear sunglasses during migraine attacks in an attempt to reduce photophobic symptoms (Q4). This low prevalence might be due to traditional Korean thought. Korean people tend to think that wearing sunglasses in public or in front of other people is rude behaviour. To evaluate the value of this question, a further survey is needed among people in Western countries. Previously, some authors have suggested that true photophobia may be a pain induced by bright light (25). However, the reported prevalence of photic stimuli-induced migraine was relatively low in previous studies (30–57%) (1, 6), and, moreover, its prevalence was extremely low in the present study (Q7, 13%). Therefore, we thought that it is not appropriate to assess photophobia in migraineurs using this definition only.
In phase 3, two subgroups composed of three questions (Q135 and Q235) seem to be statistically comparable to the whole questionnaire for detecting photophobia. These short-form questionnaires consist of one question about glittering sensations, one question about avoiding behaviours and one question about painful photophobia. These findings also suggest that if we ask a patient at least three questions about photophobia during an interview, we could detect photophobia with the same detection power as the whole questionnaire. The short-form questionnaire can be easily used in out-patient clinics without great effort.
Since the ID-Migraine was introduced, its validation test has been performed (11, 26–28). The reported studies have shown that nausea, photophobia (ranging from 49 to 75% in those studies) and disability symptoms could be used to detect migraine. An ID-Migraine study was also performed in Korea, in which the prevalence of photophobia was low (49%) (26). Moreover, numerous epidemiological studies performed in Asia have reported the prevalence of photophobia (35–60%) to be lower than that of Western studies (74–88%) (13–18). However, there is a study that showed the frequency of photophobia to be up to 100% in Asian-Americans with migraine (29). Some researchers have questioned this result, but could not suggest possible causes (14). In the present study, the prevalence of questionnaire-documented photophobia in Korean migraineurs (82.5%) seems to be compatible with results investigating photophobia in Western people. From our results, we hypothesize that the difference of reported photophobia prevalence between Asian and Western people might be caused by cultural differences in self-reported behaviours during interview with physicians.
The present study has several limitations. It was conducted by one headache specialist at one university medical centre in Korea. The number of patients was small, and the same questionnaire was not performed in patients with other types of headache or a control group. Although we considered someone as suffering from photophobia if they answered at least one question positively, we still do not know which photic hypersensitivity is specific to migraineurs. Furthermore, the questionnaire was not tested on Western or other Asian people. Further investigation is needed on Western or other Asian people comparing the results from that interview with a questionnaire like ours. However, in spite of these limitations, this study has shown how physicians ask about light sensitivity in clinical practice. Since uncovered associating symptoms could lead to incorrect diagnosis, as mentioned before (19), the International Headache Society should consider including a discussion about asking specific additional questions concerning light sensitivity in the diagnosis of migraine.
In conclusion, the prevalence of photophobia could be underreported during the simple physician interview. Our questionnaire, consisting of eight questions about various photophobic symptoms, seems to be a useful method for detecting photophobia in patients with migraine, at least in Korean. The questionnaire could improve the diagnosis of migraine and lead clinicians to give proper management to migraine sufferers. The short-form questionnaires, including three questions about photophobia, can be used as a convenient tool for detecting photophobia in migraineurs instead of a whole questionnaire.
Footnotes
Competing interests
None to declare.
Acknowledgements
This study was supported by grants from Korea University College of Medicine (K0714791).