
Abstract

Migraine is a common and chronic disorder. It is usually considered benign, but a number of studies have suggested it is an independent risk factor for ischaemic stroke, especially among women < 35 years old (1–3). An increased risk of ischaemic stroke in women with migraine with aura who use oestrogen-containing contraceptives is well established (4). This risk directly correlates with the oestrogen dose. The mechanisms underlying this risk are uncertain, but probably stem from the many prothrombotic effects of oestrogen.
Case report
A 21-year-old White female presented with a history of menstrual migraine attacks without and with visual aura in the form of both positive (usually fortification spectrum) and negative features. The aura was followed by a strictly unilateral headache of pulsatile character affecting either left or right hemicranium interchangeably. The headache lasted 6–9 h and was usually accompanied by photophobia, phonophobia, nausea and generalized malaise. She sometimes had used over-the-counter analgesics, usually ibuprofen. She was a non-smoker, had no other risk factors for stroke, and was not regularly using hormonal contraception of any kind. She had normal body weight and blood pressure. There was no family history of migraine or juvenile stroke.
Presentation. She was admitted to hospital with right, pulsating headache and vomiting associated with left homonymous hemianopia, metamorphopsias and left arm and leg paraesthesias. No fever was reported. She had used the Yuzpe regimen of postcoital contraception, which consisted of two tablets of levonorgestrel 250 μg plus ethinyl oestradiol 50 μg 19 h before presentation and a second dose of two tablets 7 h before presentation (e.g. a total of four tablets and 200 μg of ethynil oestradiol in a 12-h period of time).
Clinical assessment. Abnormal findings on examination were a left homonymous hemianopsia, slight dysarthria and decreased light touch and pin prick sensation of left hemibody. The rest of neurological and general clinical assessment was unremarkable.
Further diagnostic procedures. Laboratory determinations were normal, including hypercoagulation studies: protein C, protein S, antithrombin III, homocysteine, Leiden factor V mutation, prothrombin gene, lupus anticoagulant and anticardiolipin antibodies. Immunological studies, including anti-neutrophil cytoplasmic antibodies, antinuclear antibodies and rheumatoid factor, were normal. Erythrocyte sedimentation rate was 5 mm/h. Serum lactate level was normal. Electrocardiogram, Duplex ultrasound examination of the carotid and vertebral circulation, transthoracic and transoesophageal echocardiography were normal. Magnetic resonance imaging (MRI) showed a fresh cerebral infarction in the thalamus and right occipital cortex (Figs 1 and 2). MR angiography showed no abnormalities of the intracranial network and classical anatomy with a symmetrical and complete Willis circuitry without venous thrombosis or vasculitis features.
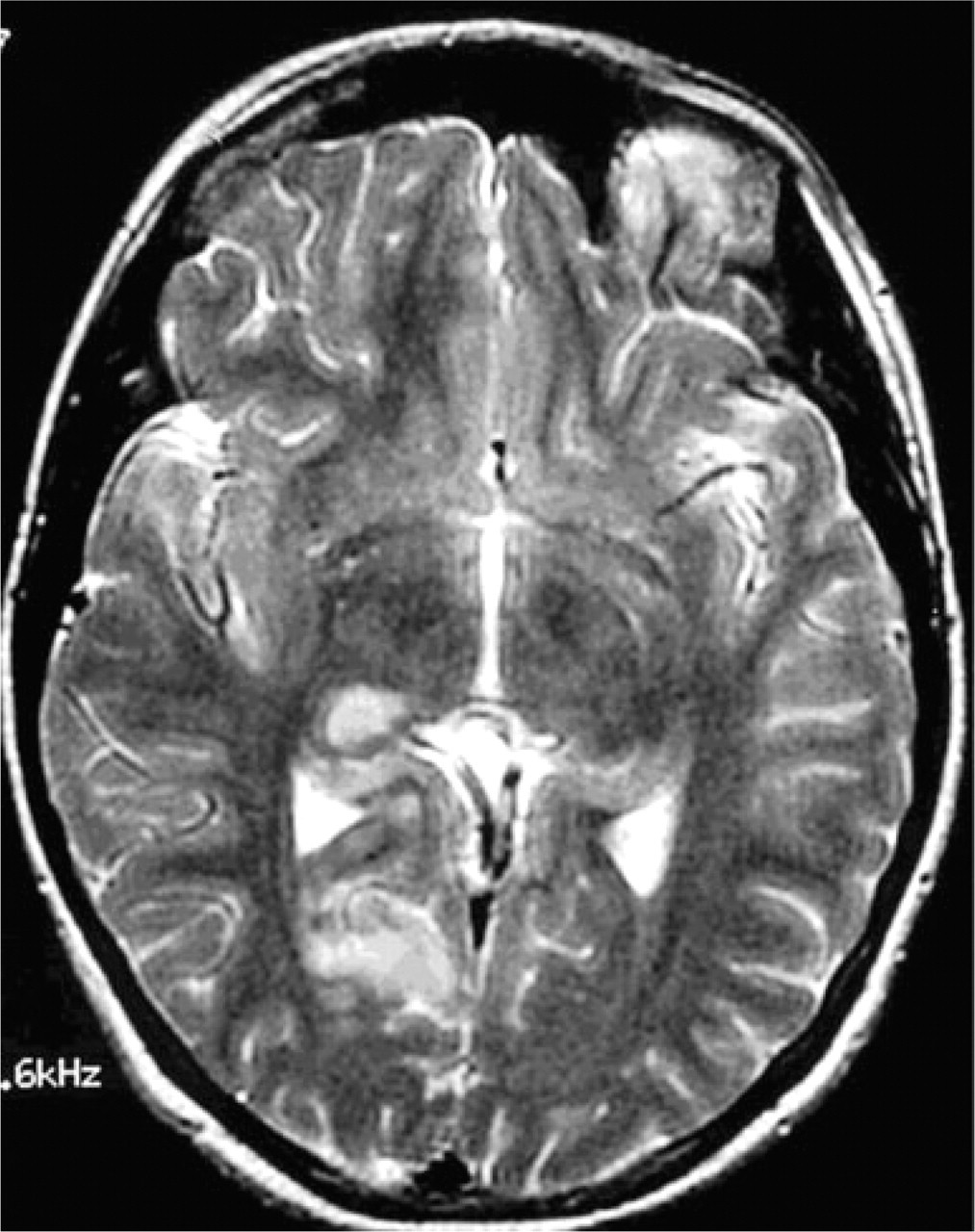
Brain magnetic resonance imaging axial T2 sequences showing cerebral infarction in the right thalamus and occipital cortex.

Brain magnetic resonance imaging coronal fluid-attenuated inversion recovery sequences showing cerebral infarction in the right thalamus and occipital cortex.
Follw-up. Headache disappeared 24 h after admission and paraesthesias on day 5, but the homonymous hemianopia persisted.
Discussion
The patient fulfilled the strictly defined International Headache Society criteria for migrainous stroke (5):
The present attack in a patient with migraine with aura is typical for previous attacks, except that one or more aura symptoms persist for > 60 min.
Neuroimaging demonstrates ischaemic infarction in a relevant area.
The infarction cannot be attributed to another disorder.
The relationship between stroke and migraine is complex and still conflicting. Migrainous stroke is more common in patients aged ≤ 45 years (6), but it can occur in patients > 90 years old (7). The migrainous stroke is more common in young women affected by migraine with aura. Smoking and oral contraceptives seem to increase the risk (8). The posterior circulation territory seems to be more affected (8, 9). In this case, other risk factors for stroke were not present and her prognosis is presumably good (8). In some cases there is a reversible cortical MRI abnormality (10). This finding clearly implies blood–brain barrier disruption, although is not clear whether this disruption relates to hypoperfusion occurring during cortical depression, or to hyperperfusion with vasogenic leakage.
There have been two other cases of migrainous cerebral infarction after postcoital contraception (11, 12). Oestrogen has also led to functional changes in haemostasis as disorders in addition and adhesiveness of platelets and decrease in levels of endothelin (13).
Plan B is a similar postcoital contraceptive regimen available without prescription in the USA, although pharmacist have to verify age. It is in the form of two levonorgestrel pills (0.75 mg in each pill), so oestrogen is not included. Accumulating evidence suggests that a history of migraine with aura may be a relative contraindication to the use of postcoital contraceptive regimens. This case suggests that postcoital contraception with a high dose of oestrogens (Yuzpe regimen) (14) could be a hidden stroke risk factor in young women with migraine. As a history of postcoital contraception may not be volunteered by a woman, questions about use should be asked of any woman with brain ischaemia.