
Abstract
Despite the recent advances in the understanding and classification of the chronic daily headaches, considerable controversy still exists regarding the classification of individual headaches, including chronic migraine (CM) and medication overuse headache (MOH). The original criteria, published in 2004, were difficult to apply to most patients with these disorders and were subsequently revised, resulting in broader clinical applicability. Nonetheless, they remain a topic of debate, and the revisions to the criteria have further added to the confusion. Even some prominent headache specialists are unsure which criteria to use. We aimed to explain the nature of the controversies surrounding the entities of CM and MOH. A clinical case will be used to illustrate some of the problems faced by clinicians in diagnosing patients with chronic daily headache.
Keywords
Introduction
The delineation of formal criteria for medical disorders is essential for both clinical and research purposes. In order to practice evidence-endorsed clinical medicine and to do quality research, it is mandatory that physicians and researchers use valid, reliable, agreed-upon diagnostic criteria for the clinical entities in question. The first edition of the International Classification of Headache Disorders (ICHD-I) was published in 1988 (1) by the International Headache Society (IHS) in an effort to standardize criteria for headache disorders worldwide. Since its inception, the ICHD-I has been generally accepted by headache specialists internationally as the gold standard for classification of headache disorders. As might be expected, not everyone agreed on the details.
Although the ICHD-I represented a major advance in the understanding and classification of headache disorders, it was difficult to apply to patients with headaches of long duration (≥ 4 h/day), on more days than not [called the chronic daily headaches (CDH)]. As a result, those patients had to be given multiple diagnoses. Commonly, they would be diagnosed with chronic tension-type headache (CTTH) and given a second diagnosis of migraine for superimposed, severe headaches. They would often require three or four different diagnoses, which is impractical in clinical practice and probably fails to correspond to disease biology. The process also violated the medical principle of diagnostic parsimony and was extremely cumbersome to utilize even for the most well-intentioned of headache clinicians (2, 3).
In the years following the publication of ICHD-I, numerous field trials were undertaken to validate or dispute the criteria for the different headache disorders (4–8). The cumulative result of this research was an evolution in the understanding and characterization of CDH and its nomenclature, leading to its refinement. In 2004, the ICHD-II was published (9). Although CDH was not included as a formal diagnosis, several different forms were described. They included chronic migraine (CM), medication overuse headache (MOH), CTTH (the only CDH incorporated in the ICHD-I), new daily persistent headache (NDPH) and hemicrania continua (HC). Since then, the criteria for MOH have already been twice revised (10, 11) and a revision for CM has also recently been published (11). Furthermore, the specific characterization of NDPH is sometimes disputed.
Because of multiple revisions in the criteria, there exists a great deal of confusion and continuing controversy, even among prominent headache specialists, about the current official criteria for CM and MOH. Therefore, we will endeavour to explain the nature of the controversy and highlight the current acceptable classification. We will also present our opinion on the usage of the most recently published criteria. A clinical case will be used to demonstrate the difficulties that clinicians face in diagnosing CM and MOH today. We hope this will enable clinicians to understand and more easily classify frequent headache disorders they see in their offices.
The chronic daily headaches—an overview
CDH syndromes comprise a group of headache disorders that occur on ≥ 15 days/month, for ≥ 4 h/day for > 3 months. As mentioned, different forms of long-duration CDH in the ICHD-II include CM, CTTH, MOH, HC and NDPH. Whereas CM, CTTH, HC and NDPH are primary headache disorders, MOH is classified in the ICHD-II as a secondary headache. ICHD-II precludes the diagnosis of any of these headache types other than MOH if the patient is overusing acute medication. In these situations, the proposed diagnosis is just MOH. MOH and CM are discussed in extensive detail below. CTTH is generally bilateral, pressing or tightening in quality, and mild to moderate in intensity, without exacerbation with movement. Associated features include no more than one of photophobia, phonophobia or mild nausea, and neither moderate nor severe nausea or vomiting. HC is an indomethacin-responsive headache characterized by unilateral, continuous pain that fluctuates in intensity. Ipsilateral autonomic features frequently accompany exacerbations of pain. Although HC was previously classified as a trigeminal autonomic cephalgia, it is no longer characterized as such due to its continuous nature (12). As the name implies, NDPH is daily and unremitting from onset. Its features are otherwise the same as for CTTH. NDPH can appear in either a self-limited form that generally resolves after several months without intervention, or a refractory form that does not respond to treatment. There is still considerable debate over the classification and clinical description of NDPH, as only a few studies describing the clinical features have been published (13).
Another classification system, the Silberstein and Lipton (S-L) criteria (14), divides the CDHs into transformed migraine (TM), CTTH, HC and NDPH, with subtypes reflecting whether or not there is acute medication overuse. The S-L criteria were used largely before the publication of the ICHD-II, since the ICHD-I did not include CM. Many still consider the S-L approach clinically more intuitive and are using it in their research and publications. That is largely because TM with medication overuse captures the longitudinal changes in patients over time, and is based on the clinical experience that evolving migraine (TM or CM) may or may not occur in the context of medication overuse.
The evolving ICHD approach to CM (see Table 1)
The evolving diagnosis of chronic migraine (CM)

ICHD-II (9) included criteria for CM, which was classified as a complication of migraine. The original criteria for CM required headaches to meet criteria for migraine without aura on ≥ 15 days/month, for ≥ 3 months, without medication overuse. However, this system was heavily criticized by clinicians attempting to categorize their patients with CDH. The criteria were felt to be overly restrictive in that they required the daily headache to meet criteria for migraine without aura on ≥ 15 days/month, which did not apply to most patients they saw with CDH. Even episodic migraine lasting for 2–3 days does not necessarily meet IHS migraine criteria each day of the attack (15).
Subsequent proposals for CM
The problems associated with diagnosing CM clearly called for a revision in the criteria. To address these issues, several alternative criteria for CM were subsequently proposed. One of these proposals (3) suggested that CM criteria should also include days of probable migraine (PM), and that CM could be diagnosed in the context of medication overuse. PM, as defined by the ICHD-II, is diagnosed in patients who have attacks fulfilling all but one of the criteria for migraine. Another proposal called for a diagnosis of CM in patients with ≥ 15 days of headache per month, of which ≥ 50% of the headache days were migraine or PM (Silberstein, in a presentation to the Classification Committee of the American Headache Society, 2005). A third proposal called for diagnosis of CM in patients with ≥ 15 headache days per month, of which ≥ 8 days were migraine or PM (Bigal et al. in a presentation to the Classification Committee of the American Headache Society, 2005). Field testing of the ICHD-II CM criteria and the three proposals was undertaken (16), using the S-L TM diagnosis as a reference point. Of 399 patients with TM with medication overuse, only 10.2% had ≥ 15 days of migraine. An even smaller proportion of patients with TM without medication overuse fulfilled criteria for CM (5.6%). The percentage of patients with TM with medication overuse who fulfilled criteria for proposals 1–3 was 37, 81 and 91%, respectively. Given the statistical significance of these results, the suggestion was made to revise the criteria for CM.
Revised criteria for CM
Subsequently, in 2006, the Headache Classification Committee published more inclusive criteria for CM, in which the disorder is defined by headaches on ≥ 15 days/month, for ≥ 3 months, of which ≥ 8 of the days fulfil criteria for migraine without aura or were successfully treated with acute care medications such as ergots or triptans (11). The article has been posted under the ‘Guidelines’ section of the IHS website, and the criteria have been endorsed by the Chairman and subcommittee chairs of the ICHD-II Classification Committee. Though these criteria are intended for the Appendix of the ICHD-II, they have not yet been included at the time of this publication. Once these criteria are validated by field testing, they will be incorporated into the main section of a future edition of the ICHD, although this may be many years away. One study (17) has already shown that when using TM without medication overuse as a reference point, 92.4% of those patients met criteria for CM using the 2006 revised criteria, compared with 5.6% that qualified as CM with the ICHD-II. At present, some headache clinicians are already using these revised CM criteria in practice, as they intuitively make the most sense, but many others are not.
Herein lies the crux of the confusion: whereas some physicians consider the revised 2006 criteria official, given their endorsement by the Headache Classification Committee, others believe that those criteria are not official until they are incorporated into the body of the ICHD. This means that not all headache specialists are using the same criteria, making current headache classification and therefore diagnoses very uneven throughout the world. In light of the fact that there may not be an ICHD-III for many years, this lack of consensus could continue for a long time, creating ongoing confusion in diagnosis and clinical trials.
Medication overuse headache (see Table 2)
The evolving diagnosis of medication overuse headache (MOH)
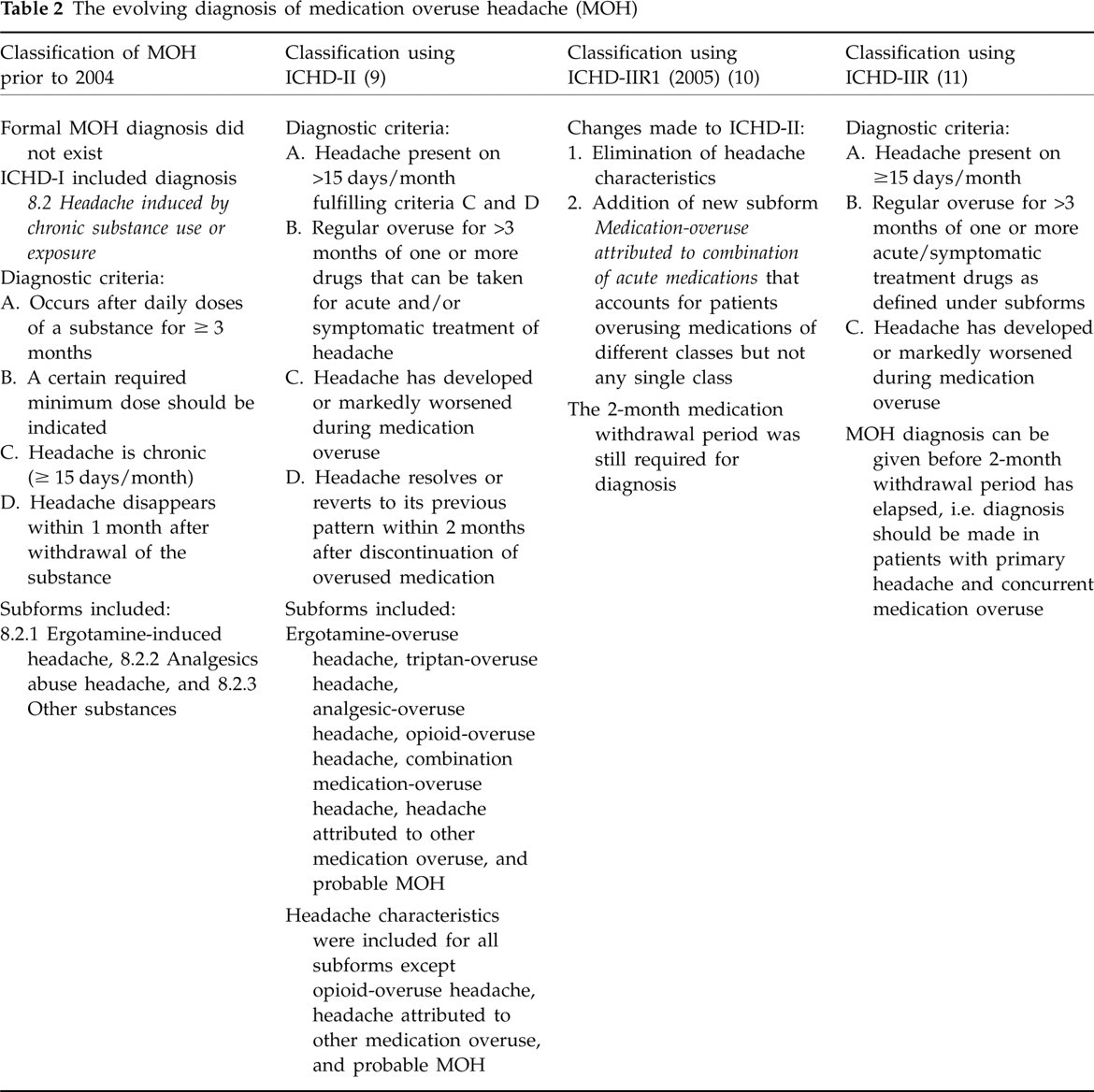
Prior to 2004, most doctors referred to MOH as rebound headache. The MOH diagnosis itself did not exist. Instead, the ICHD-I included the section ‘Headache associated with substances or their withdrawal,’ under which Headache induced by chronic substance use or exposure and Headache from substance withdrawal (chronic use) were subtypes. Criteria for Headache induced by chronic substance use or exposure specified that this was a chronic headache (≥ 15 days/month), which occurred after daily doses of a substance for ≥ 3 months, and disappeared within 1 month after withdrawal of the substance. The diagnosis could only be made retrospectively, after withdrawal of the offending drug. Subtypes included 8.2.1 Ergotamine induced headache, 8.2.2 Analgesics abuse headache, and 8.3.3 Other substances. Criteria for Headache from substance withdrawal (chronic use) stated that the headache occurred after use of a high daily dose of a substance for ≥ 3 months, occurred within hours after elimination of the substance, was relieved by renewed intake of the substance, and disappeared within 14 days after substance withdrawal. Subforms included 8.4.1 Ergotamine withdrawal headache, 8.4.2 caffeine withdrawal headache, 8.4.3 Narcotics abstinence headache and 8.4.4 Other substances.
In the ICHD-II (9), MOH was defined as a headache present on ≥ 15 days/month, with regular overuse for > 3 months of one or more drugs used for acute and/or symptomatic headache treatment. Criteria also required MOH to develop or markedly worsen during the period of medication overuse, and resolve or revert to its previous pattern within 2 months after discontinuation of the offending agent. Therefore, detoxification was required to make an official diagnosis. This meant deferring a diagnosis on a new patient for ≥ 2 months. Subtypes of MOH attributed to different medications, including ergotamine, triptans, analgesics, opioids and combination agents (simple analgesics combined with opioids, butalbital and/or caffeine) were delineated. Those criteria also specified the number of usage days per month that were required to classify a patient with a particular type of MOH. Usage of ergots, triptans, opioids or combination analgesics on ≥ 10 days/month was required to make the diagnosis of MOH, while ≥ 15 days/month were needed for simple analgesic-overuse headache. In addition, the typical headache features associated with each MOH subtype were described in detail and were extremely controversial, probably inaccurate and not universally accepted.
According to the ICHD-II, if medication overuse was present, but the other criteria for CM were met, then the diagnoses of probable MOH and probable CM were both given. If headaches persisted 2 months after withdrawal of the overused medication, then a diagnosis of CM was given, as CM could not be diagnosed in a patient with overuse. If the headaches improved, then MOH was confirmed, albeit retrospectively, and the patient was reclassified, often as episodic migraine. Most considered this system cumbersome and not representative of what they were seeing clinically.
In 2005, a revision to the ICHD-II criteria for MOH were published (ICHD-IIR1) (10). The major changes were the elimination of the headache characteristics for each MOH subtype, and the inclusion of a new subform called MOH attributed to combination of acute medications. This new subform allowed for the diagnosis of MOH in patients who were overusing medications of different classes, but not any single class. A 2-month period of withdrawal was still required before a definitive diagnosis of MOH could be made, and patients continued to be given a diagnosis of PM until that time.
Problems with the ICHD-IIR1
Although the various changes improved the classification, published studies showed that many CDH patients could still not be easily classified (2). The ICHD-II and ICHD-IIR1 were cumbersome in that patients overusing medication, a large proportion of the CDH population, were given three diagnoses (probable CM, probable MOH, and migraine with or without aura) during the period of medication withdrawal. It was also awkward, because MOH could not be diagnosed until after the overused medication had been stopped and therefore could not be diagnosed while the patient actually had the disorder. Because of these multiple diagnoses and the uncertainty of the diagnoses during medication withdrawal, these patients could not be included in clinical trials. As a result, there was a lack of carefully designed clinical trials to guide the optimal management of these patients.
Criteria for MOH were again revised by the Headache Classification Committee in 2006 (11), eliminating the requirement that the headache resolves within 2 months after the discontinuation of the overused medication. Accordingly, if a patient has headache on ≥ 15 days/month in the setting of > 3 months of regular overuse of one or more acute care medications, and the headache has developed or markedly worsened during the period of medication overuse, then a diagnosis of MOH can be made. If the headache persists after 2 months of withdrawal, then a new diagnosis of CM is given. In effect, the controversial, temporary terms ‘probable CM’ and ‘probable MOH’ are eliminated.
Like the newest criteria for CM, this latest revision of the MOH criteria is intended for the appendix of the ICHD-II, but has not been included yet. Although Professor Jes Olesen, Chairman of the Classification Subcommittee of the IHS, has been working on a complete version of the ICHD-IIR, it has yet to be published (Olesen J, personal communication, 2008). For now, the article including the latest MOH criteria (11), which is the same article outlining the new appendix criteria for CM, is posted under the ‘ICHD’ section of the IHS website. Because these criteria are not yet included in the actual text of the ICHD-II, much confusion exists as to whether they are considered official and should be used at this time. As with the new criteria for CM, some clinicians are already using these newest MOH criteria, whereas others are not.
Clinical case
A 42-year-old woman presents with daily headache for the past 5 years. Her headaches started when she was in her mid 20s. Initially, she had one to two headaches per month, frequently around her menses. Headaches were located in the left temple, severe, and generally lasted 8–12 h, untreated. Associated features included photophobia and phonophobia, and occasional nausea. Ibuprofen was usually effective in decreasing the intensity of the headaches, but did not terminate them.
Over the years, her headache frequency increased to five to seven per month. When triptans became available, the patient started using sumatriptan 6-mg subcutaneous injections, which usually aborted the headache completely within 1 h. If complete relief did not occur, she would use 400 mg of ibuprofen every 4 h until the headache abated. Headache frequency continued to increase, and the pain became progressively less responsive to triptans and ibuprofen. Approximately 5 years ago, a daily pattern emerged, which has persisted despite seven adequate trials of preventive medications, including β-blockers, tricyclic antidepressants, and three antiepileptics. At present she has a low-grade, featureless, holocephalic headache all day, every day. She has severe exacerbation of throbbing pain, usually involving the left orbito-temporal area, lasting 6–12 h two to three times per week, associated with nausea and photophobia. She uses 1–2 tablets of frovatriptan 2.5 mg at least 3 days per week, and 2–6 tablets of ibuprofen 200 mg daily.
Case discussion
This patient has CDH, given the presence of headache on > 15 days/month. The underlying headache, which started in her 20s, meets criteria for migraine without aura. Over time, the headaches have transformed from an episodic pattern into a chronic one, consistent with and most likely as a result of medication overuse. The debatable issue here is how to classify her headache disorder(s).
Using ICHD-II, without the newest 2006 criteria, the antecedent headache would be coded 1.1 Migraine without aura, and because of the ongoing overuse of triptans and ibuprofen, probable MOH would be diagnosed. Although the chronic headache has evolved from migraine without aura, she presently does not fit ICHD-II criteria for CM, given that she does not have 15 days of migraine per month, and also given that she has ongoing medication overuse. If, after a 2-month period of acute medication withdrawal, the headache reverts to an episodic pattern, the diagnosis of MOH can be made (retrospectively only). If no change in the daily pattern occurs after withdrawal of the acute medications, then a diagnosis of CTTH would have to be made, even though the antecedent headache is clearly migraine without aura. She would then also be given a diagnosis of 1.1 Migraine without aura.
Using the 2006 criteria, the antecedent headache would still be migraine without aura. However, MOH (as opposed to probable MOH) could be diagnosed during the period of overuse. If the headache pattern remains chronic after a 2-month period of medication withdrawal, then the MOH diagnosis would be dropped and a diagnosis of CM (15 days of headache per month, with ≥ 8 days of migraine without aura per month) could be made. This eliminates the cumbersome term ‘probable’ and allows for the diagnostic terminology to correspond to the clinical progression from episodic to chronic migraine (although a term like transformed chronic migraine might have been more descriptive). Using these revised criteria obviously allows for more streamlined and intuitive headache diagnosis.
Please see Table 3 for several brief clinical case scenarios.
Clinical scenarios
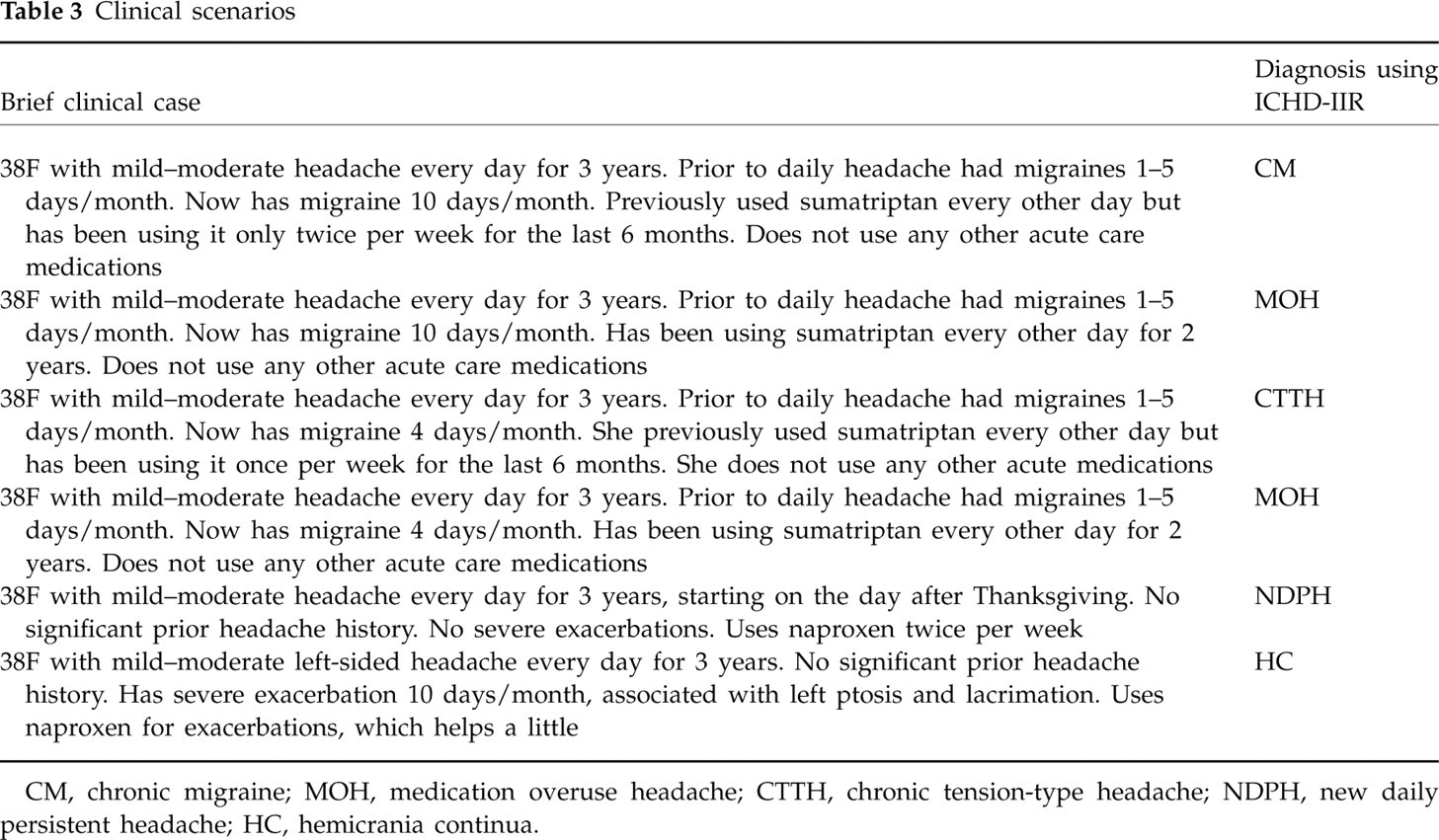
CM, chronic migraine; MOH, medication overuse headache; CTTH, chronic tension-type headache; NDPH, new daily persistent headache; HC, hemicrania continua.
Continued controversies (see Table 4)
Unresolved issues and potential problems

CM, chronic migraine; MOH, medication overuse headache; TM, transformed migraine.
Though ICHD-IIR appears to address most of the problems associated with ICHD-II, debatable issues regarding the classification system still exist. For example, the association between CM and MOH is controversial. Currently, it not clear whether MOH is a cause or result of migraine progression, although evidence points towards MOH as a risk factor for CDH (18–20). As such, the designation of MOH as a separate entity in the ICHD-II is controversial. Second, although the ICHD-IIR criteria for CM seem to correlate well with TM, the association may not be as strong in the general population, since the use of migraine-specific medications (triptans and ergots) occurs in a far smaller proportion of the general population (approximately one-third) than in headache subspecialty care (up to 80%) (17, 18). Also, if CM is based on the use of specific medications (triptans and ergots), the prevalence will be higher in countries where those medications are readily available to patients, compared with countries such as Canada that use step-care (21) and South American countries, where triptans are not usually as heavily promoted or affordable. Also very few countries other than the USA and Canada have butalbital-containing medication, which accounts for a significant proportion of the overused medications in those countries (22, 23). Lastly, the classification may not correlate with biology, in the absence of a biological marker for migraine.
Conclusion
The diagnosis and classification of headache disorders continues to evolve as our understanding of the natural history of CDH improves. However, during this period of expanding knowledge, researchers and clinicians face a significant conundrum: without diagnostic criteria that have been validated by clinical experience and trials, and/ or are widely accepted by headache specialists internationally, it is difficult to conduct reliable research and to diagnose accurately. By extension, without good clinical research, clinical guidelines cannot be established for the treatment of patients suffering from different forms of CDH. Our understanding is that the 2006 criteria (11) are the current official criteria and should be used for research purposes and in the clinical setting. Although the frequent revisions in the criteria can be confusing to any clinician, even the headache specialist, they reflect the dynamic nature of headache research today.
In conclusion, it is our strong opinion that we should adopt the changes delineated in ICHD-IIR for the diagnosis of CM and MOH immediately, not years from now. Furthermore, we need to spread the information about the new criteria and its adoption far and wide so we can all diagnose these common conditions more effectively and consistently. This can be done with the help of the IHS, the American Headache Society, the European Headache Foundation, headache journals, and the teaching of doctors with interest and knowledge in headache.
Footnotes
Acknowledgements
We thank Professor Jes Olesen for his comments regarding this manuscript. No pharmacological support has been received for this paper.