
Abstract
We employed a self-administered questionnaire to investigate exertional headache (EH) in students (ages 13–15 years) from two middle schools in Taiwan. In this study, the diagnosis of EH was made if the headache occurred during or immediately after exercise. In total, 1963 students completed the study (response rate 90.7%). The prevalence of EH was 30.4% (n = 596), was higher in girls and decreased with age. EHs were commonly bilateral (51.4%), pulsating (59.4%) and short-lasting (≤ 1 h in 79%). Only 13.8% of the adolescents with EH took painkillers for the headache. Migraineurs were more likely to have EH than non-migraineurs (47.5% vs. 21.1%, P < 0.001) and their EH had more features of migraine and needed more frequent treatment with painkillers. Only 200 subjects (10.2%) fulfilled the International Classification of Headache Disorders, 2nd edn criteria for primary EH excluding criterion C. Our study disclosed that EH was quite prevalent in adolescents. Migraineurs were vulnerable to EH and had more disabling attacks.
Introduction
Exertional headache (EH) has been recognized for decades; however, consensus on its precise definition has not been reached. In 1932, the term ‘la cephalee a l'effort’ was first used to describe four patients with intermittent paroxysmal headache that occurred only with effort (1). In 1968 Rooke (2) proposed the term ‘benign EH’ for any headache precipitated by ‘exertion,’ such as running, bending, coughing, sneezing, heavy lifting or straining at stool. The headache syndrome Rooke proposed had a prompt mode of onset, lasted for seconds to minutes and occurred predominantly in males > 40 years old. However, this definition for ‘exertion’ is unclear, since the implicated precipitants mentioned by Rooke (2) appear to have diverse mechanisms, involving mainly Valsalva-like manoeuvres, followed by mechanical factors related to the cervical spine and general physical effort. A subsequent study by Pascual et al. (3) reported 72 cases with cough, exertional or sexual headaches, of which 42% were symptomatic. In this series, benign EH specifically referred to headaches that occurred during or after sustained physical exercise, whereas headaches triggered by Valsalva-like manoeuvres as proposed by Rooke were assigned under the category of benign cough headache.
Recently, Sjaastad and Bakketeig (4–6) have reported a large-scale epidemiological headache study on adult parishioners in Vågå, Norway, using semistructured interview. The Vågå study disclosed that the prevalence of EH was 12.3%, with headache characteristics resembling what Pascual et al. (3) reported. In contrast to previous studies, which demonstrated a significant preponderance of men (2, 3), the Vågå study found that EH was more prevalent in women (F/M ratio 1.38). No other community-based study had been conducted to validate their findings. Furthermore, the Vågå study reported that some of the participants had EH early in their lives, and thus the detailed characteristics of the headaches might not be remembered (4–6). Characterizing the ‘early-life’ EH is thus important for a better understanding of the nature of the disease. Here, we report the prevalence and characteristics of EH among students aged 13–15 years, analyse its relationship to migraine and evaluate the applicability of the new diagnostic criteria for primary EH (PEH) proposed in the International Classification of Headache Disorders, 2nd edn (ICHD-2), 2004 (Code 4.3, Table 1) (7).
The ICHD-2 diagnostic criteria for primary exertional headache

ICHD-2, International Classification of Headache Disorders, 2nd edn.
Subjects and methods
Sampling
Study subjects were a convenient sample of students from two public middle schools (Yu-Li and Nei-Pu). In Taiwan, education is obligatory from ages 6–15 years. More than 90% of the teenagers aged 13–15 years attend public junior high schools, and the remainder attend private schools. The study was a sub-project of an epidemiological study on migraine in adolescents (8). All students in these two schools were recruited for this questionnaire survey (n = 2164).
Survey procedures
Letters describing the study's aims and methodologies were mailed to the principals of the sampled schools for their approval. All students in these two sampled schools were invited to answer a self-administered questionnaire.
Questionnaire
The questionnaire included two parts. The first part included a 25-item migraine questionnaire designed according to the criteria proposed by the International Headache Society (IHS), 1988 (9). The details of the validated migraine questionnaire are described elsewhere (8). In brief, the questionnaire included basic demographic data, headache profiles, aura manifestations, painkiller usage, school absence, and menstruation in girls. The second part inquired about the details of EH, including the frequency, location, duration, implicated exercise or manoeuvres, painkiller usage due to EH and the temporal association between headaches and exercise. The frequency of headaches in relation to exercise was classified into: frequent EH (nearly all or > 50% of the exercises would induce headaches), occasional EH (< 50% of the exercises would induce headaches), and no EH. The questions regarding implicated exercises included: (i) exercise types; (ii) degree of strenuousness; and (iii) head injury during exercise. The question regarding implicated manoeuvres included the following items: straining at stool; carrying heavy objects; nose-blowing; cough; and none of the above. The temporal relationship of the headaches with exercise was classified as: headaches occurred only during exercise; only after exercise; and both during and after exercise.
Headache diagnosis
Originally, we used the IHS criteria (9) for migraine diagnosis. However, for further comparisons, we reclassified the subjects according to the ICHD-2 diagnostic criteria (7) for migraine (without aura) (code 1.1), and probable migraine (code 1.6) if attacks fulfilled all but one of criteria A–D for migraine. For brevity, ‘migraine’ was used to designate ‘migraine or probable migraine’ in this communication, whereas ‘non-migraine headache’ denoted that the subject's headache did not meet the ICHD-2 criteria for migraine. Subjects who had both migraine and non-migraine headaches were classified as migraineurs.
In the present study, the diagnosis of EH was made according to the following definition: ‘headaches that occur in close temporal relationship with exercises, either during or immediately following exertion’. The questionnaire we used was designed and administered prior to the era of ICHD-2, but the key questions regarding EH included the core components of the present ICHD-2 criteria for PEH (code 4.3, Table 1), except that we did not inquire whether the headaches occurred ‘exclusively’ during or after exercise and did not occur in other circumstances (criterion C). In this study, we evaluated the applicability of modified ICHD-2 criteria for PEH, i.e. excluding criteria C, in diagnosing EH in our participants.
Statistical analysis
The prevalence of EH was reported as the number of cases per 100 persons with 95% confidence intervals (CI). Student's t-test and χ2 tests were used for comparison when appropriate. A χ2 test for trend analysis was used to analyse the trend among different age groups and numbers of migraine symptoms. P < 0.05 was considered to be statistically significant.
Results
The target population consisted of 2164 students (1098 boys, 1066 girls) in two sampled middle schools. Questionnaires with the key questions regarding the presence of EH unanswered were regarded as incomplete samples and excluded, after which the resulting final sample consisted of 1963 students (985 boys and 978 girls) with a valid response rate of 90.7%. The response rate did not differ between genders (boys 89.7% vs. girls 91.7%, P = 0.103), but was higher in Yu-Li than in Nei-Pu middle school (94.8% vs. 87.4%, P < 0.001) and in higher grade levels [94.8% (grade 9), 90.4% (grade 8), 86.7% (grade 7), P < 0.001].
Prevalence, demographics and characteristics of EH
Overall, 596 students (30.4%) (95% CI 28.4, 32.4) reported that they had EH, only during exercise (n = 113, 19.0%), only after (n = 410, 68.8%) or both during and after exercise (n = 73, 12.2%). Table 2 shows the age- and sex-specific prevalence (%) of EH. Girls had a higher prevalence of EH than boys (36.4% vs. 24.4%, P < 0.001). The prevalence decreased with age (P = 0.007); this trend was significant in girls (P = 0.015) but not boys (P = 0.144). The prevalence of EH did not differ between the two sampled schools (31.1% vs. 29.7%, P = 0.523). Among subjects with EH, Table 3 shows that exercise-induced headache occurred occasionally in most subjects (85.7%) and frequently only in 14.3% [i.e. 4.3% (95% CI 3.3, 5.3) of the total sample]. An inverse relationship between prevalence and age was also found in the frequent EH sufferers [5.9% (grade 7) vs. 4.4% (grade 8) vs. 2.9% (grade 9), P = 0.007]. The prevalence of frequent EH was also higher in girls than in boys (5.3% vs. 3.4%, P = 0.035).
The grade- and sex-specific prevalence (%) of exertional headache

Comparisons between students with frequent exertional headaches, occasional exertional headaches and no exertional headaches
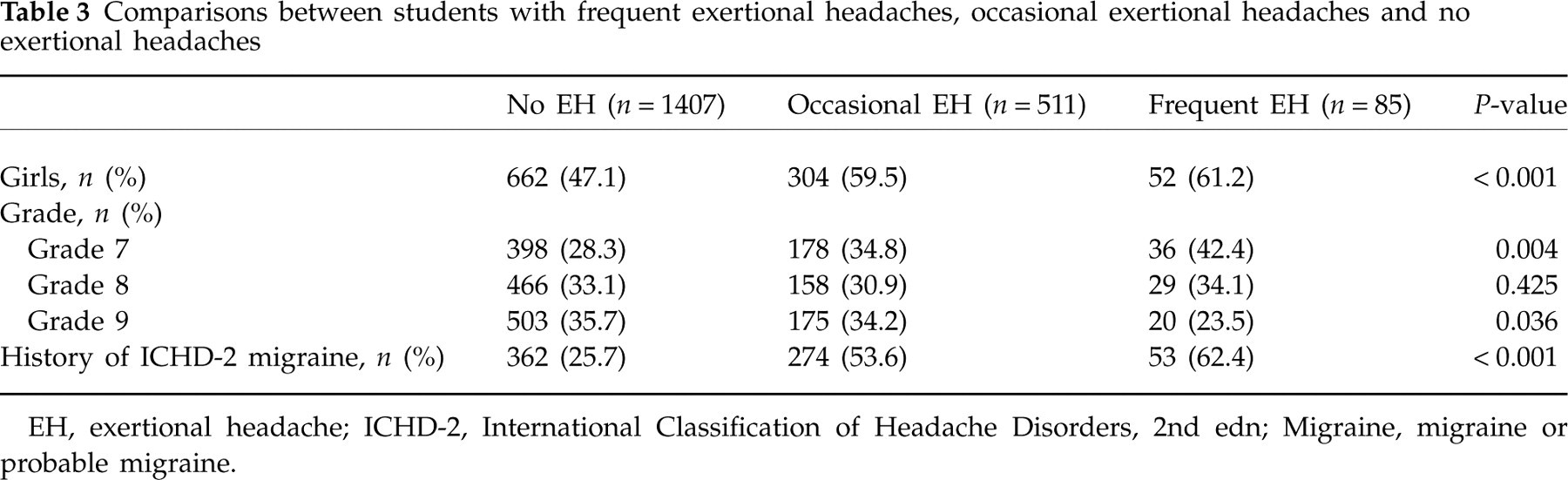
EH, exertional headache; ICHD-2, International Classification of Headache Disorders, 2nd edn; Migraine, migraine or probable migraine.
Table 4 shows the laterality, location, duration and accompanying symptoms of the 596 students with EH. The most common locations of EH were bilateral and frontal. Most (79%) of the headaches were of < 1 h. Vertex location, headache duration > 24 h, pulsating character and accompanying nausea were more likely to occur in frequent sufferers than in occasional ones (Table 4). Approximately 80% of subjects had their EH lasting < 1 h and around 45% < 5 min. About 60% of subjects reported their EH as having pulsating characteristics.
Frequency, laterality, location and duration of exertional headaches

∗ P-value was derived from comparing those with frequent exertional headaches with those with infrequent exertional headaches.
EH, exertional headache.
Types of exercises
The most commonly reported exercises that would lead to headaches included track and field (n = 198, 33.6%), basketball (n = 102, 17.3%), other ball games except basketball (n = 52, 8.8%) and swimming (n = 32, 5.4%). Of note, during the study period, there were no swimming pools in these two schools. Twenty students (3.4%) reported that any kind of exercise could induce their headaches, and 132 (22.4%) reported that their headaches occurred only when the exercise was strenuous. In addition, 47% of students with EH reported that Valsalva-like manoeuvres would also induce their headaches, which, in order of frequency, were cough (n = 109, 18.6%), carrying heavy objects (n = 42, 7.2%), nose blowing (n = 38, 6.5%) and belly laugh (n = 24, 4.1%).
EH and migraine
Among all participants, 689 (35.1%) were diagnosed as having ICHD-2 migraine based on their questionnaire, including 205 (10.4 %) migraine and 484 (24.7%) probable migraine. The overall prevalence of ICHD-2 migraine in students with EH was higher than in those without EH [54.9% vs. 25.7%, odds ratio (OR) 3.4, P < 0.001], but the difference was not significant between frequent and occasional sufferers (P = 0.134) (Table 3). In the same context, subjects with migraine were more likely to have EH than those without (47.5% vs. 21.1%, OR 2.7, P < 0.001).
However, migrainous features were generally uncommon in EH except for the pulsating character (Table 4). About 19.3% (n = 115) had their EH fulfilling ICHD-2 migraine criteria with a higher frequency in frequent than in occasional EH sufferers (29.4% vs. 17.6%, P = 0.012). The characteristics of EH in subjects with migraine were more likely to be migraine attacks per se than those without migraine (Table 5), whereas EH in subjects without migraine had fewer migrainous features and were more likely to have briefer attacks (< 5 min) (Table 5); these subjects had a higher ratio of boys (42.2% vs. 31.4%, P = 0.042) but a similar grade level distribution (P = 0.225, χ2 for trend) when compared with those with migraine.
Comparison of exertional headache characteristics between exertional headache sufferers with or without migraine history

EH, exertional headache; ICHD-2, International Classification of Headache Disorders, 2nd edn; Migraine, migraine or probable migraine.
Overall, 103 (17.3%) sufferers had EH with no migrainous features. These subjects, when compared with those with one or more migrainous features, also had a higher ratio of boys (51.5% vs. 37.9%, P = 0.011), lower frequency of pre-existing migraine (9.7% vs. 19.3%, P = 0.021), less chance of being frequent sufferers (7.8% vs. 15.6%, P = 0.038), and a higher chance of having headaches over the frontal (25.0% vs. 14.6%, P = 0.006) or vertex regions (26.7% vs. 15.3%, P = 0.013). In contrast, there was no difference between these two groups of patients regarding their grade levels, occurrence during or after exercise, different exercise types or Valsalva-like manoeuvres, or headache duration (data not shown).
We also grouped students according to the six migrainous symptoms (unilateral, throbbing, aggravation by or avoidance of physical activity, severe in intensity, ‘nausea or vomiting’, and ‘photophobia and phonophobia’) for their other headaches. Figure 1 shows that the prevalence of EH increased in subjects with higher numbers of migrainous symptoms (P < 0.001, χ2 for trend).
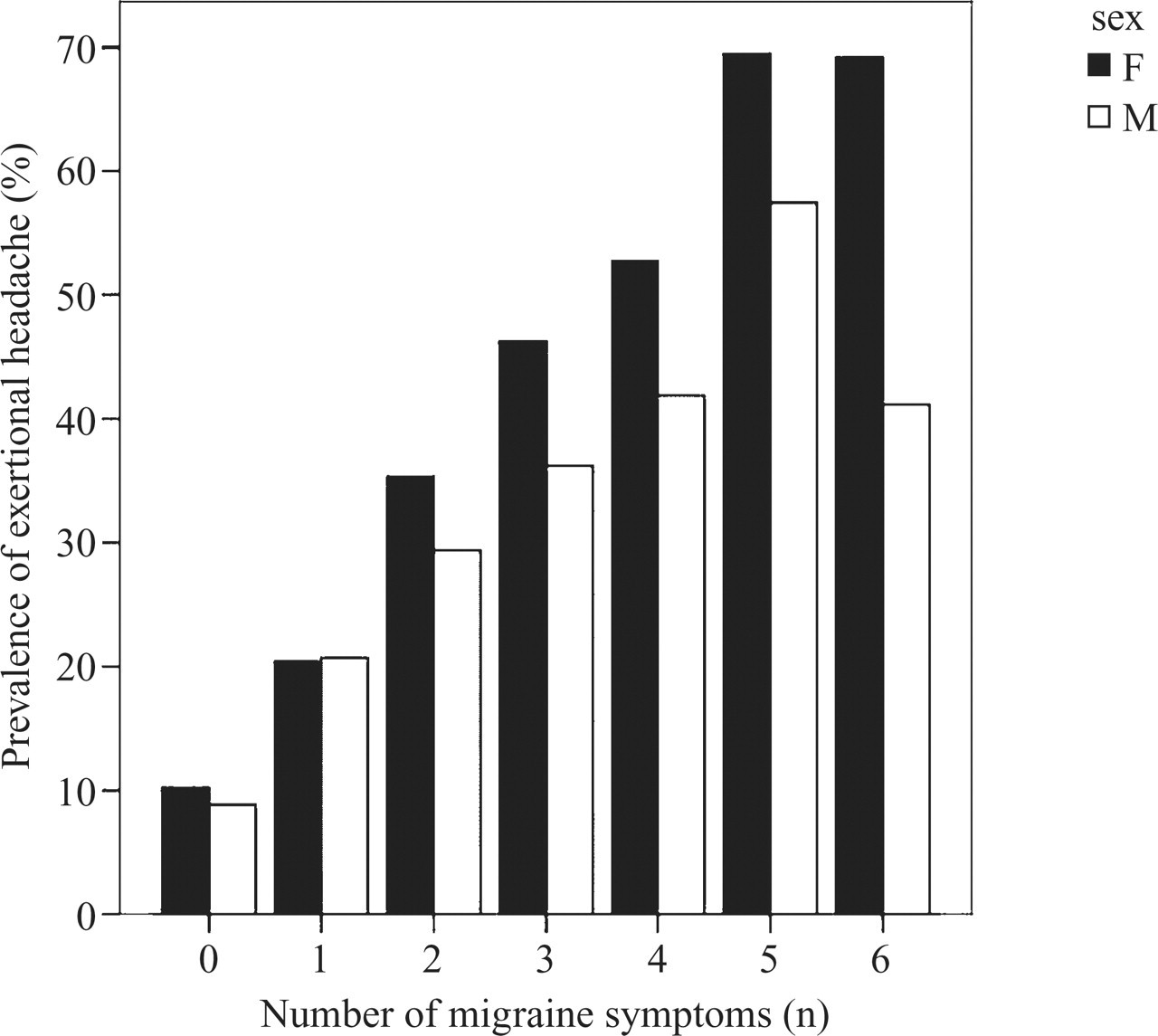
Correlation between the prevalence of exertional headache, the number of migraine symptoms and gender.
Use of painkillers
Seventy-eight (13.8%) students had used painkillers to relieve their EH. The percentage of painkiller usage was higher in those with frequent EH than in occasional sufferers (21.7% vs. 12.4%, P = 0.024). Those with EH meeting ICHD-2 migraine criteria were also more likely to have painkiller usage (39.7% vs. 16.4%, P < 0.001) than those with non-migrainous EH.
Field testing of the characteristics of EH with the modified ICHD-2 criteria for PEH
Field testing of the modified ICHD-2 criteria for PEH (Table 1) in these patients showed that only 59.4% could fulfil the ‘pulsating headache’ characteristic described in criterion A and 54% could fulfil the duration defined in criterion B. Of subjects who failed to meet criterion B, 46% were due to a shorter duration of attacks, i.e. < 5 min. Overall, only 200 students (33.6%) could meet the modified ICHD-2 criteria for PEH. Hence, the prevalence of modified ICHD-2 PEH was 10.2%. Frequent EH sufferers were more likely to have modified ICHD-2 PEH than occasional ones (49.4% vs. 30.9%, P < 0.001). Students with modified ICHD-2 PEH were more likely to have migraine attacks as EH (37.0% vs. 10.4%, OR 5.1, P < 0.001) and use painkillers (24.6% vs. 8.3%, P < 0.001) than those with EH not meeting the criteria.
Discussion
The present study is the first large-scale study to investigate EH in adolescents, which demonstrates that EH (or exercise-induced headache) is common among adolescents, with a prevalence of 30.4%. The definition we used for EH was headaches occurring during or after exercise, which was similar to that used by Pascual et al. (3) and the Vågå study. However, the prevalence in our study was much higher than in the Vågå study (12.3%). One possible explanation is that our study cohort was limited to only adolescents. A trend of decreasing prevalence of EH with increasing age was found in our study, which may in part explain the discrepancy. Recall bias of early-life experiences and being less physically active should also be considered. Nevertheless, female predominance in our study is the same as that reported in the Vågå study, suggesting that male preponderance in prior hospital-based studies could be due to sampling or reporting bias (2, 3).
Most of our participants with EH had attacks lasting < 1 h, but long-lasting (> 1 h) headaches were not infrequent, as observed in the Vågå study (6). However, the findings of a high frequency of unilaterality and low frequency of pulsating headache contradict the findings of previous studies (2–6). Such differences might be partially explained by the intrinsic differences of the study cohorts, such as age. However, these speculations await further proof. Furthermore, nearly half of our patients had headaches that could be elicited by short-lasting Valsalva-like manoeuvres; this was not seen in the Vågå study (4–6) and also deviated from the proposals of Pascual et al. (3). Rather, this finding implies that there might be an overlap between the headaches precipitated by short Valsalva-like manoeuvres and by long strenuous or exhaustive exercise. In fact, exercise such as swimming is not only aerobic but also involves isotonic or isometric activities (holding breath), simulating Valsalva manoeuvres. Valsalva manoeuvres can also sometimes be strenuous, such as carrying heavy objects. In addition, some subjects might have interpreted headache-aggravating factors such as Valsalva manoeuvres as precipitating factors, which might then have resulted in overestimation of these factors as causes of EH.
Owing to the design of the questionnaire, criterion C of the ICHD-2 criteria for PEH could not be evaluated in our study. However, even excluding criterion C, the modified ICHD-2 diagnostic criteria for PEH were still not exhaustive in diagnosing our adolescents with EH (33.6%), even in those with frequent attacks (49.4%). The finding that up to 40% of sufferers had a non-pulsating EH reduced the applicability of criterion A and provides a direction for further criterion revision. Furthermore, a high proportion (46%) of very short-lasting EH (< 5 min) made criterion B less sensitive in diagnosing EH in our adolescent cohort. One possible explanation is that it is difficult for adolescents to estimate precisely the duration of their headaches, particularly if the duration is brief. Taking the criterion more loosely, more EH would be able to meet this criterion. On the other hand, it is also possible that pulsating and shorter headache duration are implicit characteristics among headaches in adolescents when compared with adults, as has been noted for migraine. Further revision for the ICHD criteria should take this into account.
The high comorbidity of EH and migraine implies that a selected group of subjects are more vulnerable to variable paroxysmal intracranial disorders. Probably owing to the susceptibility to the implicated exercises, sufferers with pre-existing migraine tended to have EH exhibiting characteristics akin to those of migraine, whereas sufferers from EH alone were more likely to have EH bearing fewer migrainous features. The number of migrainous features might thus represent a spectrum of a disease continuum, with one end being EH without any migrainous features. In addition, even with the finding that half of the migraineurs were comorbid with EH, only a minority of exercise-induced headaches (19.3%) could actually fulfil the diagnosis of ICHD-2 exercise-induced migraine. In other words, exercise could be a trigger of migraine, but most headaches induced by exercise were phenotypically different from migraine even in migraineurs. To improve the diagnostic accuracy of EH patients with migraine, further revision of the ICHD-2 should stress the importance of excluding headaches with full-blown migrainous features from the criteria for EH. It had been proposed that EH might be caused by aberrant vasodilation during or following exercise as a consequence of impaired myogenic cerebrovascular autoregulation (10). Such aberrant vasodilation could probably initiate a migraine cascade, as the vascular theory of migraine has long proposed (11).
Furthermore, our study has disclosed that painkiller usage was uncommon in EH sufferers, even in those with frequent attacks. This finding suggests that EH is not a disabling headache disorder in most sufferers. However, the minority who used medical treatment were those with EH bearing more migrainous features or exercise-induced migraines. These subjects are the target population that clinicians should be aware of, for whom prophylaxis for EH with medications or biobehavioural strategies such as sports training, proper warm-up before exercise, or hydration with sports drinks might be helpful. The implementation of acute treatment depends on the severity and disability of the attack. For sufferers with mild to moderate EH, paracetamol or non-steroidal anti-inflammatory drugs, especially indomethacin, albeit based on only small case studies (12), can be considered. For those with EH with more migrainous features, namely the more severe form of EH, or even exercise-induced migraine, specific antimigraine therapy such as triptans might be imperative. However, current evidence does not mandate us to provide any treatment guidelines. Further studies focusing on the treatment issues are necessary.
Some limitations of the study should be addressed. First, the migraine diagnosis was obtained by questionnaire rather than physician diagnosis. Nevertheless, the sensitivity and specificity are appropriate for a field study (8). Second, this analysis treated all sufferers as ‘primary’ EH instead of ‘symptomatic’ unless focal neurological symptoms were reported. However, we are not sure whether the EHs disclosed in the present study were all ‘benign’; a possibility of ‘symptomatic’ EH could not be completely ruled out by our study design.
Footnotes
Acknowledgements
This study was supported in part by a grant from V97A-039.