
Abstract
We conducted the first population-based migraine survey in Taipei, Taiwan, using a validated questionnaire administered by interviewers during the period from August 1997 to June 1998. Our target population comprised all individuals (age ≥ 15 years) in 1400 randomly selected households. Migraine diagnoses were made according to the classification criteria of migraine without aura proposed by the International Headache Society, 1988, except that attacks with a duration of between 2 h and 4 h were also included. Of the 4434 eligible subjects in the 1211 respondent households, 3377 (76%) completed the questionnaire. After adjustment for age and sex distribution according to the population structure, the prevalence of migraine was 9.1% (F/M 14.4%/4.5%). Fifty-four percent of the subjects with migraine had consulted a physician about their headaches in the past year. However, only 18% of them reported that their migraine had been diagnosed by physicians. This study found that Taipei residents have the highest migraine prevalence of all Chinese populations studied, although it is still in the low range of prevalence compared with the results from Western countries.
Introduction
The effect of racial differences on the prevalence of migraine is still inconclusive (1). Asians have been shown to have a lower prevalence of migraine than Caucasian populations (2–5). Community surveys conducted in several Chinese populations showed a strikingly low migraine prevalence: 0.63–0.69% in the People's Republic of China (PRC) (2, 3) and 1.5% in Hong Kong (4). In contrast, the prevalence of migraine has ranged from 8% to 15% in Western series (6–10). This discrepancy might be due to a variety of factors, including diverse cultural, genetic or environmental backgrounds, and differences in methodology or diagnostic criteria. An important advance in the standardization of migraine diagnosis was the publication of operational criteria by the Headache Classification Committee of the International Headache Society (IHS) in 1988 (11). Although its validity is still questioned, the consistency of migraine prevalence surveys among different Western countries suggests that it is reliable (12). In addition, the use of the IHS criteria improves the validity of cross-cultural comparisons of migraine prevalence.
Using IHS criteria, we found a prevalence of migraine in the Chinese elderly on Kinmen Island, Taiwan (13), which was 4–10 times higher than in the same age groups in the PRC (2, 3) and Hong Kong (4). In addition, a recent survey in Japan (5) also found that migraine prevalence was much higher than that found by surveys done in the PRC and Hong Kong. These findings led us to suspect that the prevalence of migraine in the Chinese might not be as low as previously reported. Therefore, we conducted a community-based survey using the IHS diagnostic criteria to estimate migraine prevalence in the Chinese population randomly selected from households in the Greater Taipei Area of Taiwan.
Subjects and methods
A population-based questionnaire interview was conducted among subjects aged ≥15 years in each randomly selected household sampled from the Greater Taipei Area from August 1997 to June 1998.
Target area
The Greater Taipei Area includes Taipei City and Taipei County. Taipei City is further geographically sectored into 12 ‘Chius’ (i.e. districts), and the County into 29 ‘Shiangs’, ‘Jens’ or ‘Shihs’ (i.e. townships) as the second-level administrative units. Each district or township is further sectored into Lis (in the Chius, Shihs, or Jens) or Ts'uns (in the Shiangs) as the basic administrative units. In total, there were 1377 basic units (Lis or Ts'uns), 1.83 million households, and 4.6 million people aged ≥15 years in the Greater Taipei Area, according to the data on the 1996 year-end population structure reported by the Department of Statistics, Ministry of the Interior (14).
Sampling method
In order to obtain at least 1000 respondent households in this study, we planned to sample 1400 households based on the population structure. Therefore, the household sampling rate was calculated to be 0.075%.
We adopted a stratified two-stage systematic random sampling method. The basic administrative units (i.e. Lis or Ts'uns in the districts or townships) were designated as the primary sampling unit. Each household in the selected primary sampling unit was the secondary sampling unit.
In the first stage of sampling, 10% of the basic administrative units in each district or township were drawn. They were first numbered by their size (i.e. the number of households) and then were sampled using systematic random sampling. In the second stage of sampling, household samples were selected from the sampled units in proportion to the size of the sampled units with a sampling rate of 0.75% (i.e. one per 130 households, as the interval size). Combining the two sampling stages, the overall combined sampling rate was about 0.075% of all the households in the Greater Taipei Area.
Headache questionnaire
The questionnaire was composed of three parts. The first part was demographic characteristics. The second part was a headache profile (30 questions), which was designed to comply with the operational criteria of the headache classification of the IHS (11). The third part included health status, sleep hygiene, and mental health.
The participants were asked about their headache profile during the previous year, based on the IHS classification for migraine, including attack frequency (average number of headache days per week: < 1, 1, 2, 3, 4, or ≥5 days/week), severity (mild, moderate or severe intensity defined as no influence, inhibition, or prohibition of daily activities, respectively), pulsatile or non-pulsatile headache, presence or absence of headache aggravation from climbing stairs or routine physical activities, location (unilateral or bilateral), duration of headache attacks (< 30 min, 30 min to 2 h, 2–4 h, 4–72 h, or > 3 days), and accompaniments (presence or absence of nausea, vomiting, photophobia or phonophobia). They were asked to answer the questionnaire using the more severe type of headache as a standard if they had more than two types of headache. They were also asked if they had had five or more attacks of the more severe type of headache in their lifetime. In addition, four major migraine aura symptoms (visual, sensory, motor, and speech symptoms) were also queried.
The subjects were also asked to rate the level of impairment caused by their headache attacks in their daily activities, social activities, and work or school, using a 0–10 visual analogue scale (VAS). A 10-cm horizontal line was used with marks at both ends, labelled ‘the most severe impairment’ at the right end and ‘no impairment’ at the left end. No further intermediate marks were placed on the lines. In addition, data were collected on medical assistance-seeking behaviour for headache, including physician consultation and the usage of painkillers.
Diagnosis of migraine by the questionnaire
Migraine diagnoses were made according to the diagnostic criteria of migraine without aura (IHS code 1.1) in the IHS classification schema (11). To establish a diagnosis of IHS migraine in this study, five or more attacks in a lifetime were needed. Each attack had to have lasted 4–72 h and had to have any two of the following four pain characteristics: unilateral location, pulsating quality, moderate-to-severe intensity, and aggravation by routine physical activity. In addition, the attacks had to be associated with at least one of the following: nausea or vomiting, or photophobia and phonophobia. In addition to the IHS criteria for migraine, we also included subjects whose attacks lasted for 2–4 h but fulfilled all the other IHS migraine features under the category of ‘modified migraine’, as with the studies done in Japan (5). Modified migraine was also considered a true migraine in this study.
Diagnosis of aura based on the IHS criteria is difficult using data obtained from a questionnaire (5, 15). We adopted the diagnostic method for migraine with aura as used in the Japanese study (5). Migraine with aura was diagnosed only if the subjects' headache characteristics met the classification criteria for migraine without aura (IHS and modified migraine), and if they also had had aura compatible with the IHS criteria for migraine aura (IHS code 1.2). Briefly, their aura had to meet two of the three following criteria: lasting > 4 min; < 60 min; and the interval between headache and aura being < 60 min. It should be noted that whether or not their aura symptoms were due to ‘focal cerebral dysfunction’ was not used as a criterion in this study. The subjects who suffered migraine both with and without aura were included in the migraine with aura diagnostic group. Migraine aura without headache was not included as a diagnostic category in this study.
Clinical validation of the headache questionnaire
At the beginning of the large-scale survey, the validity of the questionnaire was also tested in the field. The first 160 participants, who admitted that they had had headache in the year previous to the interview, were invited to take part in the study for validation of the use of the questionnaire to diagnose migraine. Among them, 142 (89%) were successfully interviewed by neurologists using a telephone semistructured interview within 8 weeks of questionnaire administration. The neurologists independently arrived at a diagnosis using IHS migraine criteria without prior reference to questionnaire data. The validity of migraine diagnosis by the questionnaire was appropriate with an agreement rate of 87% and a κ value of 0.66. The sensitivity of the headache questionnaire was 76%, specificity was 91%, positive predictive value was 74%, and negative predictive value was 91%. The validity of questionnaire-diagnosed migraine aura was not satisfactory, with a κ statistic of 0.41, sensitivity 56%, specificity 94%, positive predictive value 39%, and negative predictive value of 97%.
Survey procedures
Our interviewers visited the sampled households and explained the study objectives and methods to the residents aged ≥15 years, and asked for their oral consent before the interview. In this study, the interviewers administered the questionnaire interview to each participant in person.
Statistical analysis
In this study, the diagnosis of migraine included both IHS and modified migraine, unless otherwise specified. The 1-year prevalence with 95% confidence intervals (CI) is presented as the number of cases per 100 persons. Age (per 5 years) and sex-specific prevalence were also calculated. A goodness of fit test was used to test the sex and age distribution between the participants and the 1996 year-end population structure of the Greater Taipei Area. Since the response rates were different among different age groups and genders, an adjustment was made according to the distribution of the population structure. Student's t-test and χ2 test were used for comparison when appropriate. The validity of the headache questionnaire was assessed by agreement rate, κ statistics, sensitivity, specificity, positive predictive value, and negative predictive value. P < 0.05 was considered statistically significant.
Results
Participants
Of the 1400 sampled households, 1211 households (86.5%) responded. Of 4434 eligible subjects in the respondent households, 3377 subjects (76%) (F/M 1804/1573) participated in the study. The age and sex distribution of the 1996 year-end population and our participants is shown in Table 1. It was noted that the elderly (≥ 65 years old) men outnumbered the elderly women in the population structure. The reason is that a certain proportion of the elderly in Taiwan came from Mainland China in 1949 after the Civil War. They are predominantly male and at present are at an advanced age. When compared with the 1996 population structure, there was a significantly higher ratio of females (53.42% vs. 50.05%, χ2 = 15.4, d.f. = 1, P < 0.001, goodness of fit test) and younger subjects (5 years for each age group) (χ2 = 132, d.f. = 11, P < 0.001, goodness of fit test) who completed the questionnaire interview.
A comparison of the sex and age (≥ 15 years) distribution between the participants in the study and the 1996 year-end census in the Greater Taipei Area

Prevalence of any headache and headache profile in the previous year
Sixty-two percent of the participants (50% of the men and 72% of the women, P < 0.001) admitted that they had had at least one headache during the past year. Among the headache subjects, 65% (72% of the men and 43% of the women) had had an average headache frequency < 1 day/week. However, 4.1% of the subjects (5.3% of the women and 2.8% of the men) had had an average headache frequency of ≥4 days/week in the previous year. Twenty-four subjects (0.7%) (17 women (0.9%) and seven men (0.4%)) complained of daily headaches.
About 23% of the subjects (28% of the women, 17% of the men) had had moderate to severe headaches in the previous year. One-quarter of the subjects (31% of the women, 17% of the men) admitted that they were troubled by their headaches.
Prevalence of migraine in the previous year
The 1-year crude prevalence of migraine was 9.7% (95% CI 8.7–10.7%) (328/3377). The age- and sex-specific prevalence of migraine is illustrated in Table 2. Women (14.2%, 256/1804, 95% CI 12.6–15.8%) had a significantly higher prevalence of migraine than men (4.6%, 72/1573, 95% CI 3.6–5.6%) (χ2 = 88.5, d.f. = 1, P < 0.001), with a women/men ratio of 3.1. In women, the highest migraine prevalence occurred in the age range of 30–34 years (21.1%); in men, it occurred in the age range of 25–29 years (8.3%).
One-year prevalence of migraine in the Greater Taipei Area by age and sex
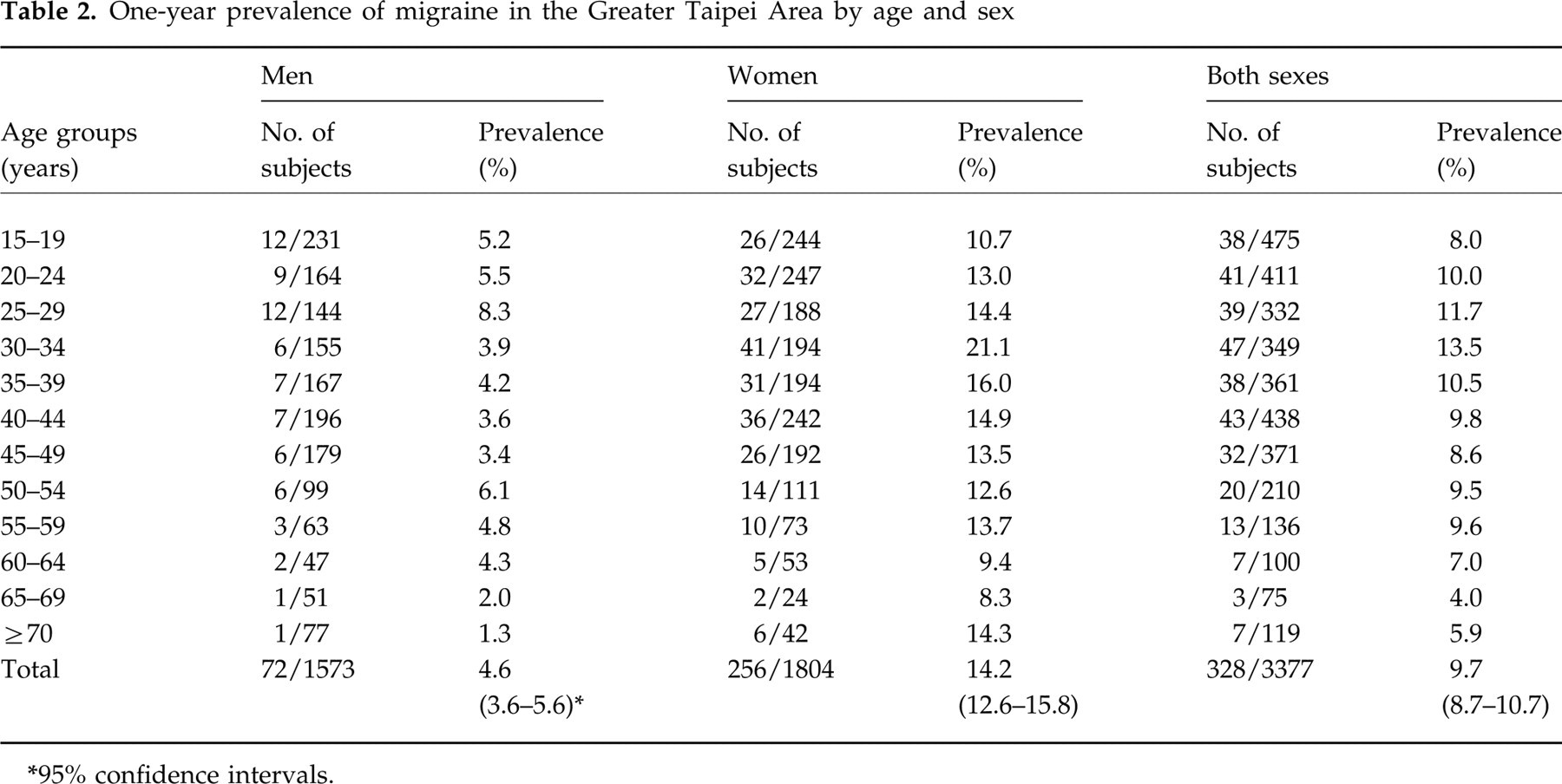
95% confidence intervals.
After adjustment based on the age and sex distribution of the 1996 year-end population structure, the 1-year migraine prevalence was 9.1% (4.5% in men, 14.4% in women).
The prevalence of migraine strictly meeting the IHS criteria (IHS migraine) was 7.7% (95% CI 6.8–8.6%) (n = 261), with 11.2% (95% CI 9.7–12.7%) (n = 207) of the cases occurring in women, and 3.4% (95% CI 2.5–4.3%) of the cases occurring in men, and with a female to male ratio of 3.3. In contrast, the prevalence of migraine according to our modified criteria was 2.0% (n = 67).
Except for age and gender, the prevalence of migraine was not related to personal income, family income, education level, or occupation.
Migraine aura
Of the 328 subjects with migraine, 12.5% had had migraine with aura. The frequency of migraine with aura in male subjects with migraine was significantly higher than that of the female subjects with migraine (24% vs. 9%, χ2 = 10.4, d.f. = 1, P = 0.001). The most frequent aura symptoms were visual aura (78%) followed by numbness of one side of the body (32%).
Accompanying symptoms of migraine
The frequencies of the symptoms accompanying migraine were nausea 59.1% (n = 134), vomiting 34.5% (113), photophobia 67.4% (221) and phonophobia 87.2% (286). The frequencies of the above symptoms in subjects with IHS migraine were similar.
Average headache days among migraineurs
In order to reduce the possible confusion between migraine and non-migraine attacks, subjects were asked about the average number of headache days per week instead of focusing on true migraine attacks. Among the subjects with migraine, the most frequent average number of headache days per week was < 1 day (47%), followed by 1 day (20%) and 2 days (17%). The other frequencies were 3 days (6%), 4 days (4%), and ≥5 days (6%) per week.
Severity of migraine
A total of 82% of the subjects with migraine considered their headache symptoms to be of moderate (44%) to severe intensity (38%). Eighteen percent of migraineurs considered their headache to be of mild intensity.
Ratings of the degree of impairment caused by headache attacks in subjects with migraine using the VAS (0–10) were: daily activities 3.8 ± 2.9, social activities 5.2 ± 2.8, and work or school 5.8 ± 2.7.
Self-awareness and physician consultation for migraine
Sixty-five percent of the subjects with migraine considered that they had had migraine before this survey. In contrast, 37% of the subjects with non-migraine headache also thought that they had had migraine.
In the year immediately preceding the interview, 54% of the subjects with migraine had consulted a physician about their headaches. However, only 18% of them reported that migraine had been diagnosed by physicians.
Discussion
This study is the first community-based migraine survey among the general population in Taiwan. The overall adjusted 1-year prevalence of migraine was 9.1% among people aged ≥15 years in the Greater Taipei Area, with a 14.4% prevalence in women and a 4.5% prevalence in men.
Methodology issue
Several points should be addressed concerning our study methodology.
Sampling and selection bias
The response rate in this study was 86.5% for sampled households and 76% for eligible individuals, which is appropriate for a field study. There was a higher ratio of female participants, which is also common for this kind of study. In addition, since this study was designed and described as a headache survey, it is likely that sample selection was influenced by the inclusion of a greater number of participants with headaches than is representative of the general population. However, our interviewers tried their best to recruit all the eligible subjects in the respondent households to decrease this bias.
Validity of the questionnaire
The validity of the questionnaire used to diagnose migraine was appropriate for such studies. Our questionnaire was designed based on the operational criteria of the IHS. These criteria are more explicit and reliable than the prior criteria of the Ad Hoc Committee on Classification of Headache (12, 16). In line with a previous study done in Japan by Sakai & Igarashi (5), we found in the clinical interview by telephone for the validity study that the subjects with headache usually underestimated their headache duration because they often took medications for or slept off the headache. This is the reason that we adopted the criteria similar to those used by Sakai & Igarashi (5), that the diagnosis of migraine include headache attacks lasting between 2 h and 4 h. As for aura, the validity of the diagnosis of aura by our questionnaire was rather poor, with a low sensitivity and positive predictive value.
Studies of headache in different Chinese populations
Several large-scale community-based headache prevalence studies have been done in the PRC (2, 3) and Hong Kong (4). Cheng et al. (2) and Zhao et al. (3) reported very low migraine prevalence in the PRC, but these studies were done before the IHS criteria were proposed and thus are difficult to compare with IHS-based results. Wong et al. (4) also reported a low prevalence of headache in the Chinese population in Hong Kong, which was only equivalent to about one-sixth of the prevalence of headache in Taipei found in the present study. This major discrepancy may have arisen from several factors, including the differences in study methodology. The study in Hong Kong (4) evaluated 1-year prevalence and used IHS criteria, similar to our study. However, the low prevalence in the Hong Kong study might have been due to (i) exclusion of headache sufferers with one or less attack in the previous year; (ii) a 19% loss rate at the second confirmation visit; and (iii) a high percentage of clinically validated migraineurs (31%) who had a questionnaire-based headache diagnosis of ‘unclassified headache’. It is even harder to compare the results from the two studies from the PRC (2, 3) since they used the Ad Hoc criteria (16) for migraine and only subjects with migraine with aura were included.
Studies from other Asian countries
There have been few epidemiological surveys using IHS criteria in Asia (5, 17). Sakai & Igarashi reported results similar to ours in a nation-wide survey in Japan, with a 1-year migraine prevalence of 8.4% (strict IHS 6.0%) (5). In contrast, Roh et al. reported a very high migraine prevalence (including IHS 1.7) of 22.3% and a low female to male ratio of 1.2 in South Korea (17). The exact causes of these unusual findings are not clear. Roh et al. attributed their results to a low response rate and different genetic or socio-cultural factors (17). However, the misclassification of tension-type headache as migraine should also be considered when the results of the epidemiological survey show an overestimated prevalence and a lower than expected gender ratio.
Studies from Western countries
Except for the study done in Canada (10), most large-scale epidemiological surveys using IHS criteria have been done in Western countries, revealing a quite consistent 1-year prevalence ranging from 10% to 12.1% (5.7–6.1% in men, and 15–17.6% in women) (6–8). Although higher than previous studies done in the other Chinese populations, our results as well as those of the study in Japan (5) are still in the low range of prevalence compared with the results of studies in Western countries, supporting the hypothesis that Asians have a lower migraine prevalence. Interestingly, in the Baltimore County Prevalence Study, Stewart et al. found that the prevalence of migraine was highest among Caucasians (women 20.4%, men 8.6%), followed by African–Americans (women 16.2%, men 7.2%) and Asian–Americans (women 9.2%, men 4.8%) (1).
Symptoms accompanying migraine
Subjects with migraine (both IHS and modified) in our study had a lower frequency of photophobia (67%) than those in previous studies done in Western countries (around 90%) (1, 18). This result was also found in a clinic sample of migraine patients in Taiwan who had an even lower frequency of photophobia (14%) (19). However, the frequency of photophobia was as high as 100% in Asian–Americans with migraine in a study done by Stewart et al. (1). The cause of the different reporting rate of photophobia is unclear. However, since the presence of both photophobia and phonophobia is one of the major criteria for IHS migraine (11), whether or not the low frequency of these symptoms in our studied subjects might have influenced migraine prevalence needs further study.
Age and gender effect
The prevalence of migraine was the highest in men aged from 25 to 29 years and in women aged from 30 to 34 years, which is similar to the findings of most epidemiological studies. The female to male ratio (3:1) is also in line with most previous studies (6–8, 10). The ratio of migraine with aura to migraine without aura was significantly higher in men (1:4) than women (1:9). This result was also reported in previous studies (5, 18). However, it is not a consistent finding (17). It should be noted that the present study is limited by the low validity in reporting aura by our subjects.
Headache frequency
Compared with previous studies (7, 9, 17), our migraine subjects had higher frequencies of headache. Ten percent of them reported having four or more headache days per week. The exact reasons are not fully known. Some indigenous differences in the study design might be contributing factors. Previous studies usually asked the migraineurs to estimate the number of migraine attacks in a year, but in our study we asked the migraine subjects to estimate the total headache days in a week, and all kinds of headache, not only migraine attacks, were included.
Migraine in Taiwan
Unlike previous studies done in the PRC (2, 3) and Hong Kong (4), the present study revealed that migraine is a common and important disorder in Taiwan. If the extrapolation is valid, the estimated number of migraine sufferers in Taiwan is 1.5 million (1.15 million women and 0.35 million men). Migraine has a significant impact on the lives of sufferers, not only in their daily activities but also in their work and social functions.
Since the Chinese word for migraine (unilateral, head, pain) is quite self-explanatory and very commonly used in daily life in Taiwan to denote a ‘one-sided headache’, many migraine sufferers (65%) in this study considered that they had had this illness (i.e. migraine), even though they probably did not exactly know the definition of a migraine attack. Therefore, about 37% of the subjects with non-migraine headache also regarded themselves as having had migraine.
The physician consultation rate (54%) in the year immediately prior to the interview was high in our subjects with migraine. Although this might have been due to the disability caused by migraine attacks, the easy accessibility of physicians and the low cost of each visit provided by the National Health Insurance Programme in Taiwan might also have contributed to this high rate of physician consultation. In contrast, the low migraine diagnosis rate in our subjects with migraine (18%) may reflect either a lack of awareness of the symptoms of migraine on the part of physicians, or cultural factors, which lead physicians in Taiwan seldom to directly inform patients of their diagnosis, if not asked.
Footnotes
Acknowledgements
This study was supported by National Health Research Institute grants (DOH86-HR-633, DOH87-HR-633, and DOH88-HR-633).