
Abstract
The objective of this analysis was to describe psychological and cognitive variables in subjects with migraine and to identify those associated with chronicity. Data were collected from 10 000 subjects during face-to-face interview. Subjects with episodic migraine (n = 1127) or chronic daily headache (n = 407) with migrainous features were identified using an algorithm based on the International Classification of Headache Disorders, 2nd edn classification. Data on headache impact was obtained with the Headache Impact Test-6, on psychological distress with the Hospital Anxiety and Depression Scale, on coping with the Coping Strategy Questionnaire catastrophizing score and the Brief COPE inventory, on illness perception with the Brief Illness Perception Questionnaire and on locus of control. Psychological variables associated with chronicity include perceived headache impact, psychological distress, the use of catastrophizing and avoidance coping strategies and an externalized locus of control. In conclusion, maladaptive coping strategies should be taken into account in the management of patients with migraine. Longitudinal studies will be necessary to address the causality of the relationship observed.
Introduction
Migraine is a common and incapacitating episodic neurological disorder (1) associated with considerable handicap in terms of pain and distress, impaired quality of life and lost productivity (2). In addition, significant psychiatric comorbidity occurs in migraine sufferers (3–5), with important therapeutic implications (6). In particular, much evidence has accumulated for an association between migraine and anxiety or depression (7–10). Chronic daily headache (CDH) corresponds to a particularly incapacitating form of headache (11), and subjects with such headaches may present more psychological distress than those with classical episodic migraine.
It is interesting to investigate coping strategies and illness perceptions in patients with migraine, since the use of adaptive coping skills may reduce the risk of emergence of comorbid anxiety or depression. The coping strategy used has been shown to be associated with emotional reactivity in migraine in several studies (12–19). An association between migraine headaches and maladaptive coping strategies, notably catastrophizing, has previously been demonstrated (15, 20). Little published data exist on illness perceptions in migraine. Page et al. (21) have used the Illness Perception Questionnaire (IPQ) to study illness perceptions in patients with CDH and found that patients with psychological distress expect their headaches to have more personal consequences and to last longer than patients without.
It is possible that perceptions and attitudes towards headache, such as the choice of coping strategy, may differ between patients with classical migraine and CDH. We have recently had the opportunity to test this hypothesis in a large, general population-based survey of migraine recently performed in France. The principal objective of the study was to identify the determinants of consulting a physician. Data on consultations (22), as well as on treatments (23), have been published previously in this journal. However, during the study, information on psychological and cognitive features was collected systematically, allowing us to perform an exploratory study on psychosocial characteristics and chronicity of migraine headache. The present report describes the findings of this study.
Methods
This was a descriptive epidemiological study performed in a representative sample of the French adult general population between March and May 2005. A national representative sample of the general population was screened in order to identify migraine sufferers, who were interviewed in extenso to collect data on impact of headache, psychological aspects, symptoms of comorbid anxiety or depression and healthcare resource utilization. The methods used have been described extensively in a previous publication (22).
Constitution of the study sample
A target sample of 10 000 members of the French adult population was constituted who were aged ≥ 18 years and were representative of the national population in terms of gender, age, employment status, place of residence (nine geographical regions and five classes related to the population size of the town, village or city of residence) according to the most recent census data from the French National Statistics Office (1999). The survey was conducted by Institut de Sondage Lavialle, an international polling institute (http://www.islavialle.fr). A quota method (24–26) was used to ensure uniform representation of each socioeconomic category in the final sample. In this method, a hypothetical target sample is constituted which is structured in such a way as to match the overall French adult non-institutionalized population in terms of the four stratification variables (age, gender, employment status and place of residence). Each interviewer was assigned a territory and instructed to recruit a quota of subjects for each stratum, in accordance with the distribution of individuals in the hypothetical target sample. The total number of subjects to be recruited by the interviewer was weighted according to the total population of the territory. The investigator visited households in the territory in a random order to identify a member of the household matching one of the strata, who is invited to participate. In case of refusal, the next household is visited. Once the target quota of subjects for each stratum is reached, recruitment is complete for that territory. Study samples constituted by the quota method are thus de facto representative, in terms of the prespecified quota criteria, of the general population.
Interviews
Face-to-face interviews were conducted in the subject's home by trained interviewers as part of an omnibus survey that asked specific health-related questions within a much wider multisubject questionnaire. This system is thought to provide greater motivation and more neutral responses to questions on medical subjects. Interviewers were specifically trained to carry out the interviews before the start of the survey. The CAPI/POLLUX (Computer Assisted Personal Interview) system was used to ensure exhaustive, accurate and unambiguous data collection. Thirteen screening questions were asked during the interview in order to identify individuals with migraine. Replies to these questions allowed a diagnosis of migraine to be assigned.
Attribution of headache diagnosis
A diagnostic algorithm was used to attribute one of three headache diagnoses on the basis of replies to the screening questions and the International Classification of Headache Disorders, 2nd edn (ICHD-II) criteria for headache classification (27). This has been described in detail in a previous publication concerning this study (22). These three headache types were migraine (ICHD-II categories 1.1 or 1.2), probable migraine (ICHD-II category 1.6) or CDH with migrainous features (CDH-M). For the present analysis, the migraine and probable migraine groups were collapsed into a single ‘episodic migraine’ group. In the case of CDH-M, subjects were required to fulfil both the criteria for strict or probable migraine and a specific chronicity criterion derived from the ICHD-II classification, namely headache on > 15 days per month during > 3 months (corresponding to ICHD-II category 1.5.1, chronic headache).
Data collection
Individuals identified as having migraine headaches were then asked about their migraine headaches in a subsequent part of the same interview, and a number of psychometric rating scales were completed. These were the six-item Headache Impact Test (HIT-6) (28, 29), the Hospital Anxiety and Depression Scale (HAD) (30, 31), the catastrophizing subscore of the Coping Strategy Questionnaire (CSQ) (32, 33), the Brief COPE Inventory (34, 35) and the Brief Illness Perception Questionnaire (BIPQ) (36, 37), all used in their French translations. The total duration of the interview was between 30 and 40 min. For individuals who did not fulfil criteria for migraine, the interview was stopped after the screening questions.
Psychometric rating scales
The HIT-6 instrument (29) is a six-item questionnaire that yields an impact score on a linear scale with minimum and maximum possible values of 36 and 78, respectively. On the basis of this score, subjects can be assigned to one of four impact grades. These are little or no impact (Grade 1; score ≤ 49), moderate impact (Grade 2; score 50–55), substantial impact (Grade 3; score 56–59) and severe impact (Grade 4; score ≥ 60). The HIT-6 questionnaire was derived from a number of existing headache-related questionnaires using item response theory. It has been validated in a number of cultural settings (38) and has since been used widely in epidemiological studies (39) and as an outcome measure in clinical trials (40). Elevated scores on the HIT-6 have been shown to be correlated with headache severity and poor quality of life (41).
The HAD is a 14-item questionnaire assessing severity of symptoms of anxiety and depression, seven items relating to anxiety and seven to depression and each scored on a four-point Likert scale. Possible scores for each pathology dimension range from 0 to 21, with a higher score reflecting greater severity. The scale was originally developed to detect states of depression and anxiety in the setting of a hospital medical out-patient clinic, but has since been used widely in both primary care and general population settings. The HAD is one of the most widely accepted scales for evaluating emotional distress in non-psychiatric populations, used in > 1000 studies to date. Two systematic reviews (42, 43) have evaluated the psychometric properties of the HAD and concluded that the scale provided clinically relevant results as a screening tool for emotional distress and performed well in somatic, psychiatric and primary care patients as well as in the general population. In particular, the factorial structure of the scale discriminating between an anxiety and a depression dimension was found to be justified. For the authors of the scale, a score > 8 on either score corresponds to clinically relevant anxiety or depression. In subsequent validation studies (43, 44), this threshold has been found to have the optimum sensitivity and specificity for detection of generalized anxiety disorder or major depressive disorder identified by other diagnostic instruments, including the Diagnostic and Statistical Manual of Mental Disorders-IV (45).
The Brief COPE was developed to assess the different ways in which people respond to stress and was derived from a longer questionnaire, the COPE, developed a decade previously. It contains 14 scales of two items, each of which measures conceptually distinct aspects of coping. Each item can be scored on a four-point Likert scale. The total scores on each scale are normalised on a scale of 0–100. The Brief COPE was originally validated in a population of hurricane victims in the USA, and yielded Cronbach coefficients of internal validity ranging from 0.5 to 0.9 according to the scale (34). It has since been used widely in its original American version in healthcare studies relating, for example, to drug addiction, ageing, breast cancer, depression, surgery and AIDS. The 28 items are generally reduced to a restricted number of dimensions, identified by factor analysis. The Brief COPE has been translated into French and Spanish and validated in these languages. The French version of the Brief COPE was validated in a population of healthy university students and the factorial structure re-analysed using structural equation modelling (35). In this analysis, the psychometric properties of the questionnaire were found to be good. Since university students represent a quite different population from the subjects with headache evaluated in the present study, we re-determined the factorial structure of the Brief COPE using data collected in the study. This follows recommendations of the authors of the questionnaire to generate specific dimensional structures for a given study population. This determination used principal component analysis with varimax rotation of the correlation matrix of the 28 items in the Brief COPE.
The CSQ was designed to evaluate cognitive coping strategies in chronic pain syndromes. It was originally validated in patients with chronic back pain and found to be internally reliable (32). A number of factorial analyses have shown it to contain several dimensions which are relatively stable between different patient groups and can be rated independently using specific subscores (32, 46, 47). The catastrophizing subscore of the CSQ was used in the present study, since it has been shown to have robust construct validity (48) and to be pertinent for individuals with headache (12, 17). Moreover, it represents a coping dimension that is not explored in the Brief COPE. In the French version (33), it contains four items, each scored on a four-point Likert scale, yielding a total score ranging from 4 to 16, with higher scores indicating strong reliance on this strategy.
The BIPQ was developed from the longer 80-item Revised Illness Perception Questionnaire (IPQ-R) (49) and is based on the self-regulatory model proposed by Leventhal (50, 51). It investigates cognitive perceptions of illness and contains eight items scored on a 10-point Likert scale and a ninth open-response item on disease identity. These items were designed to sum up different dimensions of perceptions of illnesses, covered by multiple items in the original IPQ or IPQ-R. They correspond to different cognitive representations of causes and consequences of disease, cure and control, and the duration of illness. The sum of the mean scores on the eight items can be used to generate the total BIPQ score. The question exploring the disease identity dimension was adapted for headache, since this item is disease-specific (49). The questionnaire was originally validated in six patient groups and showed good test–retest reliability, moderate to good associations with the corresponding dimensions of the IPQ-R and good concurrent, predictive and discriminant validity (36). Although the BIPQ has been translated into French (37), as far as we are aware no study has yet been reported using the French version of the questionnaire. For this reason, the data collected in the study were used to assess the internal consistency of the French version of the BIPQ, as a preliminary approach to validation.
In order to explore the locus of control, subjects were asked to rank three statements about personal health in order of most agreement. These statements were: personal health depends principally on medical advances (personalized external locus of control), personal health depends principally on actions that I take to look after myself (internal locus of control) and personal health depends principally on chance (impersonal external locus of control).
Statistical analysis
Categorical variables were compared with the χ2 test or with Fisher's exact test in case of low (< 5 in any group) sample size, ordinal variables by the Kruskal–Wallis test and quantitative variables by analysis of variance for normally distributed variables or by the Mann–Whitney U-test for variables departing from normality. Odds ratios (ORs) with 95% confidence intervals (CIs) were determined where appropriate.
Psychological variables whose distribution varied between the episodic migraine and CDH-M groups at a probability level of 0.10 were retained for a stepwise multivariate logistic regression analysis. ORs with 95% CIs were determined from the final model for each variable. In order to address the possibility of spurious findings generated by the stepwise model, we performed a supportive analysis using a hierarchical hybrid model with forward and backward regression. Variables were entered into the model at four levels, with variance being controlled at each level after accounting for variance in the previous levels. The first level included clinical variables that are temporally or logically most relevant or not subject to change, as well as age and gender (namely age, gender, headache and other clinical headache characteristics). The second level included HAD scores and CSQ catastrophizing score, the third level included the BRIEF COPE items and the HIT-6 impact score, and the fourth level the individual BIPQ item scores.
Two-sided statistical tests were used throughout, and a probability level of 0.05 was considered statistically significant. All data were analysed centrally using software from SAS (SAS Institute Inc., Cary, NC, USA; version 8.2).
Ethics
The study was performed according to international and French regulatory guidelines and current codes of Good Epidemiological Practice. Since patient care was not altered by inclusion in the study, ethics committee approval was not necessary. With respect to data confidentiality, the study was declared to the ‘Commission Nationale d'Informatique et des Libertés’.
Results
Subjects
During the screening phase, 10 032 subjects were interviewed. Of these, 2740 reported suffering from headaches, 1127 of whom fulfilled diagnostic criteria for episodic migraine group and 407 for CDH-M. The sociodemographic characteristics of the study sample are presented in Table 1. The majority of subjects were female (77.8%) and young adults (mean age 40.5 years). A significant difference in the gender distribution between the two diagnostic groups was observed (P = 0.003), the female predominance being most pronounced in the CDH-M group. There were no such significant differences observed for age distribution.
Sociodemographic properties of the study population according to diagnostic group

CDH-M, chronic daily headache with migrainous features; ICHD-II, International Classification of Headache Disorders, 2nd edn.
∗A significant difference between the two headache groups.
Subjects with episodic migraine presented a significantly higher level of income and education (P < 0.001) compared with the CDH-M group, were more likely to be in employment (49.2% vs. 43.5%; P < 0.01) and to own their own home (37.8% vs. 28.0%; P < 0.001). They were less likely to live alone (37.3% vs. 46.0%; P = 0.002), to be divorced or separated (10.8% vs. 20.2%) or to be not working for health reasons (1.9% vs. 5.9%). No differences were seen between the two diagnostic groups in terms of place of residence (administrative region of France or population size of the community).
The clinical features of migraine headaches are also described in Table 1. Subjects fulfilling diagnostic criteria for CDH-M were more likely to present associated signs of migraine than those in the episodic migraine group, with the exception of lateralization and nausea or vomiting. The latter symptom was more frequent in the episodic migraine group. The age of onset of headache disorder was younger in the episodic migraine group. In 40% of subjects with episodic migraine, headache frequency was reported to be one or two headaches per month (Fig. 1).
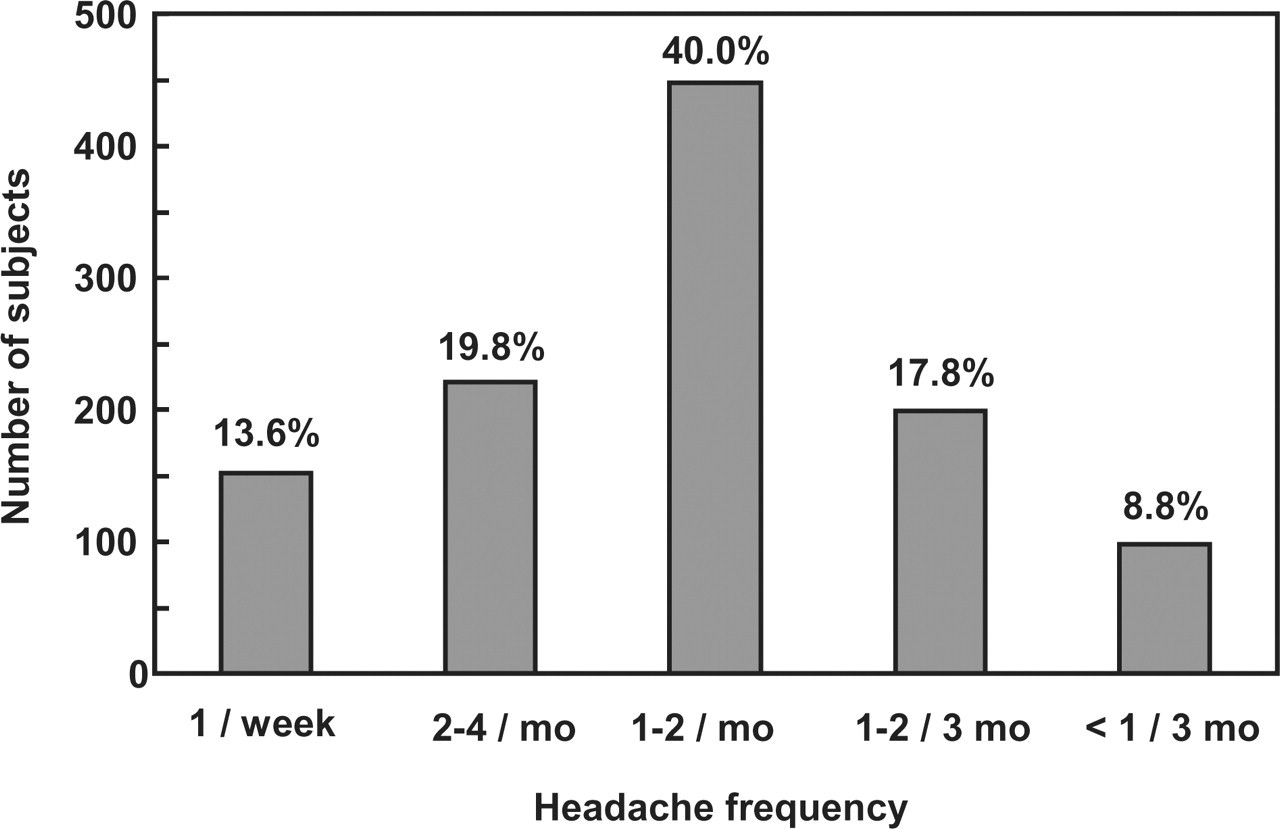
Headache frequency in the episodic migraine group.
HIT-6 headache impact test
Mean scores on the HIT-6 instrument were 57.0 ± 9.1, with over half the subjects (56.8%) reporting severe or substantial impact (Fig. 2). Both mean HIT-6 impact scores and distribution across impact groups differed significantly (P < 0.001) between the episodic migraine and CDH-M groups, with greatest impact being reported in the latter group. The proportion of subjects with severe or substantial impact was 85.3% in the CDH-M group compared with 46.6% in the episodic migraine group.
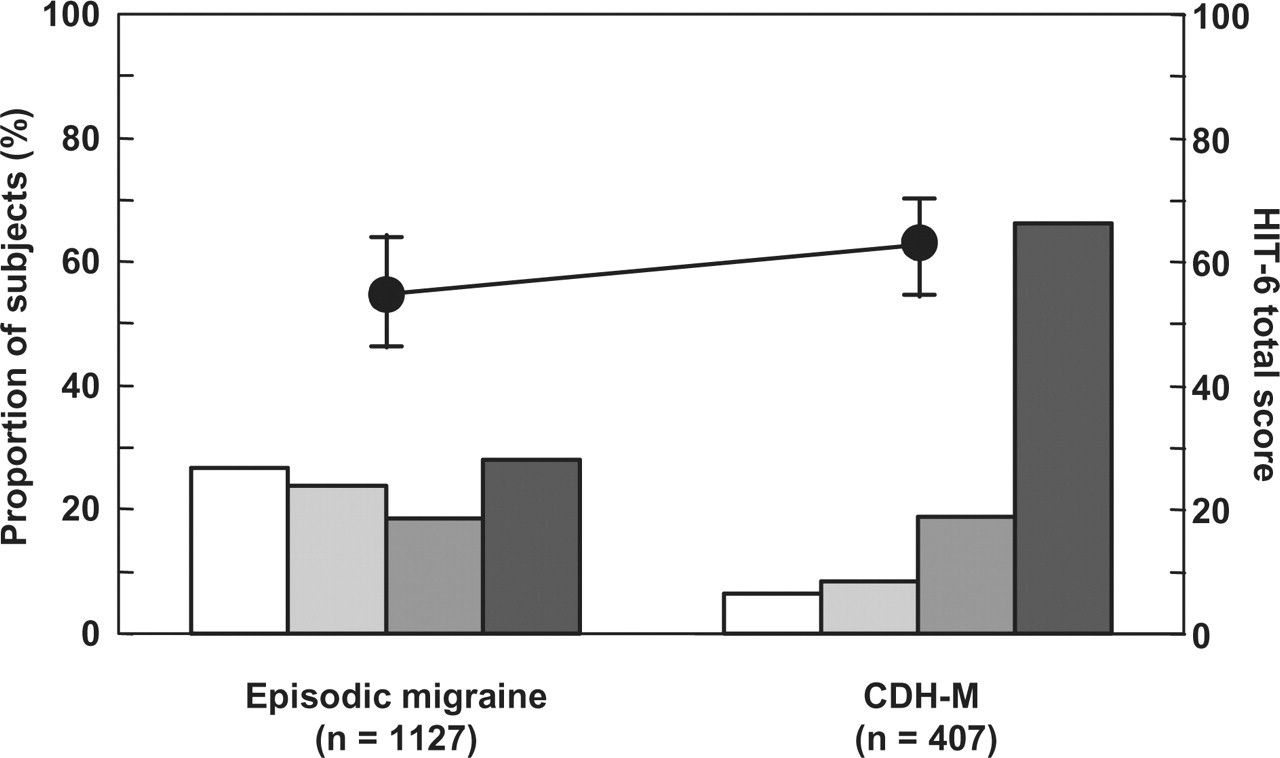
Scores on the Headache Impact Test (HIT)-6 scale in the study population according to diagnostic group. The round symbols represent mean ±
Hospital anxiety and depression scale
Mean HAD emotional distress scores were 14.1 ± 6.5 (Table 2). Scores on the anxiety dimension, but not the depression dimension, were above the threshold of 8 considered to represent clinically relevant symptoms. Scores were significantly higher (P < 0.001) in the CDH-M group. The proportion of patients with HAD scores > 8 was also significantly higher (P < 0.001) in the CDH-M group (Table 2).
Scores on the Hospital Anxiety and Depression scale according to headache diagnosis

IQR, interquartile range; CDH-M, chronic daily headache with migrainous features.
Coping
The mean CSQ catastrophizing score was 8.1 ± 4.5, with higher scores being reported in the CDH-M group (mean ±
The factorial analysis of the Brief COPE inventory identified six dimensions that explained 50% of the total variance in the data (Table 3). Increasing the number of dimensions improved the quality of fit only minimally (< 5% of additional variance explained). Two items were excluded from the structure as they had saturation coefficients of < 0.45 on all dimensions. The internal consistency of the resolved structure, as measured by Cronbach's α coefficient, was 0.83.
Factor analysis of the Brief COPE scores obtained in the overall study population (n = 1534)

For two of the coping dimension subscales, namely the social support seeking and emotional expression and avoidance dimensions, scores differed between the episodic migraine and CDH-M groups, being significantly higher (P < 0.001) in the CDH-M group (Fig. 3).

Dimension scores on the six dimensions of the Brief COPE Inventory according to headache diagnosis. Data represent mean values ±
Perception of illness
The internal consistency of the French version of the BIPQ, as measured by Cronbach's α coefficient, was 0.68. Mean total scores on the BIPQ were 5.7 ± 1.6 in the episodic migraine group and 6.8 ± 1.3 in the CDH-M group. This difference was statistically significant (P < 0.001). Mean scores on the individual items are presented in Fig. 4. Significant differences in scores between the two diagnostic groups were observed on all items except the treatment control and understanding items, with greatest illness impact being observed in the CDH-M group.

Item scores on the Brief Illness Perception Questionnaire according to headache diagnosis. Data represent mean values ±
When asked about ‘the most important factors that cause your headaches’, the most frequent replies were stress (39.2%), heredity (10.8%), menstruation (9.3%), emotional state (4.4%) and chance (4.3%). Subjects with CDH-M more frequently replied ‘stress’ (47.7% vs. 36.1% in the episodic migraine group) and subjects with episodic migraine more frequently replied ‘menstruation’ (11.5% vs. 3.2% in the CDH-M group).
Locus of control
There were also significant differences in what the patients considered to be the most important determinants of personal health (P < 0.001). Subjects in the CDH-M group were more likely to think that this depended primarily on medical advances or chance and less likely to think it depended on looking after one's self compared with the episodic migraine groups, indicating a more externalized locus of control (Fig. 5).

Perceived determinants of personal health according to headache diagnosis. Open columns, episodic migraine; filled columns, chronic daily headache with migrainous features. Nineteen subjects did not consider any of the three determinants to be most important. The distribution of subjects across locus of control categories was significantly different (P < 0.001) between the two headache diagnosis groups.
Multivariate analysis of variables associated with chronicity
The psychological variables whose distributions varied between the episodic migraine and CDH-M groups were entered in a stepwise multivariate logistic analysis to eliminate covariates. This model retained five variables that were independently associated with chronicity (Table 4). The strongest association was observed for the HIT-6 headache impact score, followed by the BIPQ total score. The other variables retained were the HAD emotional distress score, the CSQ catastrophizing score and the locus of control. Since the gender distribution differed between the episodic migraine and CDH-M groups, and gender may influence some of the psychological variables of interest, the logistic analysis was repeated including gender as a test variable. This retained the same variables as the original analysis with similar odds ratios (data not shown), whereas gender was not retained (OR 1.21, 95% CI 0.85, 1.17).
Given the strong association between the BIPQ total score and chronicity, we repeated the analysis using the individual BIPQ item scores rather than the total score. In this model, the BIPQ identity score was the variable with the strongest association with chronicity (OR 1.30, 95% CI 1.22, 1.38; P < 0.0001). Two other BIPQ items were also retained in this model, the Timeline score (OR 1.11, 95% CI 1.05, 1.18; P = 0.0002) and the Treatment control score (OR 0.92, 95% CI 0.87, 0.96; P = 0.0003).
Finally, we performed a hierarchical hybrid regression, in order to assess contributions of the more experimental variables (such as the BIPQ items) only when variance introduced from unambiguous (such as gender) or better validated variables (such as the HAD score) had been accounted for. The variables retained in this model are presented in Table 5. In general, this model identified the same variables as in the stepwise model, notably the most strongly associated variables such as the HIT-6 score and the BIPQ identity item score.
Variables associated with chronicity identified in multivariate analysis ranked in order of appearance in the stepwise model
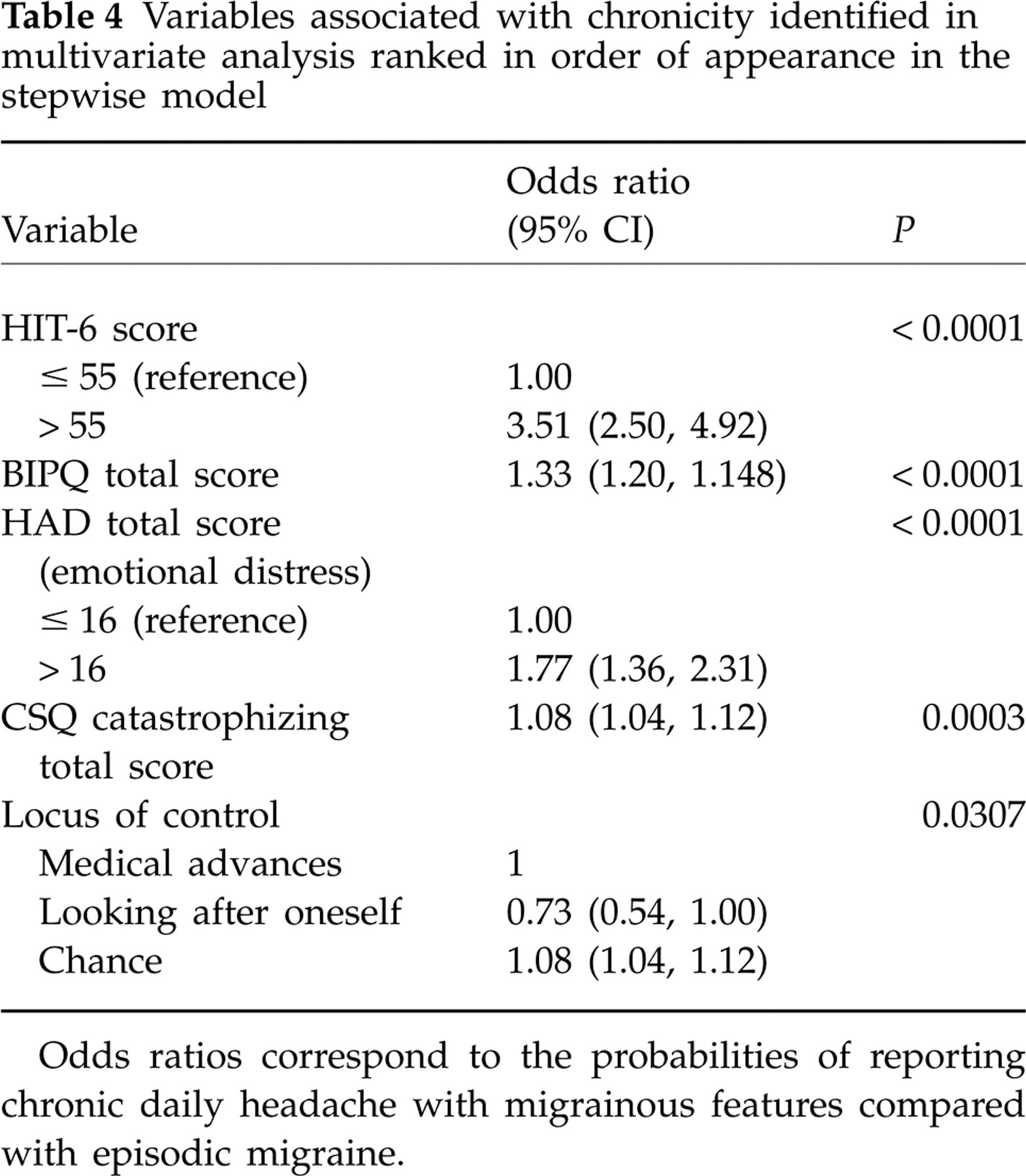
Odds ratios correspond to the probabilities of reporting chronic daily headache with migrainous features compared with episodic migraine.
Variables associated with chronicity identified in multivariate analysis using the hierarchical hybrid regression model
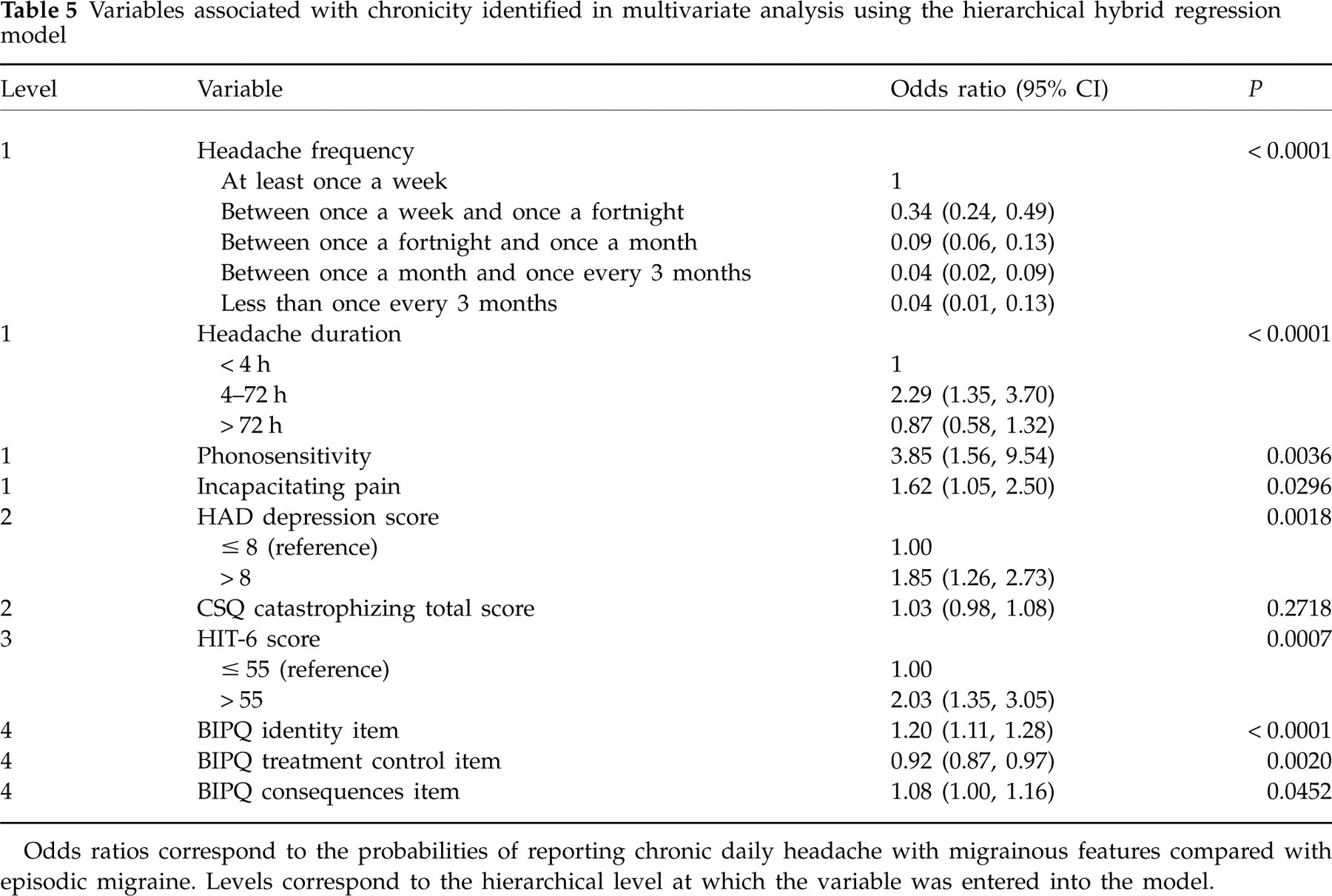
Odds ratios correspond to the probabilities of reporting chronic daily headache with migrainous features compared with episodic migraine. Levels correspond to the hierarchical level at which the variable was entered into the model.
Discussion
In this exploratory study of psychosocial variables and chronicity of migraine headaches conducted in the French general population, we identified several variables which differed between subjects with CDH-M and those with classical migraine, with greater impairment being observed for the CDH-M group. These variables are perceived headache impact, emotional distress, coping strategies, illness perceptions and the locus of control.
One of the most striking differences concerned headache impact, as measured with the HIT-6, where 85% of subjects in the CDH-M group fell into the severe or substantial impact brackets, compared with 47% in the episodic migraine group.
Psychological distress was higher in the CDH-M group compared with the episodic migraine group. Mean depression scores remained in the normal range. Nevertheless, the proportion of subjects with HAD depression scores above the threshold for clinically relevant depression was over twice as high in the CDH-M group. In a previous study, we have observed an increased prevalence of mood or anxiety disorders in patients with medication overuse headache compared with those with classical migraine (4). Moreover, these disorders had a tendency to occur before the transformation from migraine into medication overuse headache. Others have also postulated that psychiatric comorbidity is associated with poor prognosis in migraine headaches (52). It has also been suggested that treating comorbid anxiety and depression is a critical component of strategies to prevent transition to chronicity in episodic migraine sufferers (53). Although in our present cross-sectional study no conclusions can be drawn about the temporal relationship between psychiatric comorbidity and chronicity, these results underscore the importance of screening for anxiety and depressive disorders in migraine patients.
Concerning the relationship between coping strategies and chronicity, we observed more catastrophizing in subjects with CDH-M, as well as some differences between the two groups on items of the Brief COPE inventory, although the latter were not retained in the multivariate logistic analysis. In particular, subjects with CDH-M were more likely to use support seeking and emotional expression or avoidance than subjects with episodic migraine. The clinical significance of differences of this magnitude is unclear. No difference was observed in the use of adaptive strategies (positive reinterpretation, problem-directed coping and acceptance) between the episodic migraine and CDH-M groups. In addition, our data show an association between high headache impact and high emotional distress, on the one hand, and high catastrophizing scores on the other.
These findings are consistent with previous studies that have demonstrated more recourse to maladaptive coping strategies in subjects with chronic headaches or transformed migraine (13, 54–57). In particular, Rollnik et al. (55) have suggested that disadvantageous coping strategies might contribute to transformation of tension-type headaches to chronic forms. Support seeking and emotional expression represents a maladaptive emotional coping strategy centred on helplessness, reliance mainly on others for resources to control pain and looking for compassion from others. Many studies have shown an association between use of such a strategy and poor adjustment to pain and excessive pain perceptions (58, 59). Avoidance coping is also a maladaptive strategy and is the principal target of cognitive behavioural therapy. In the fear-avoidance model, avoidance coping is considered to be the principal barrier to better adjustment to chronic pain (60–62).
Using the BIPQ, we found that subjects with CDH-M considered themselves to have less personal control over their headaches than subjects with episodic migraine, whereas they scored higher on the consequences, timelines, identity, concerns and emotional response items. On multivariate analysis, the total BIPQ score represented the variable with the second strongest association with chronicity after the HIT-6 score. The individual BIPQ items most strongly associated with chronicity were the timeline and identity items.
Concerning the locus of control, we found this to be more externalized in subjects with CDH-M rather than episodic migraine. Previous studies in migraine have found that an externalized locus of control is associated with greater disability (63–65) and more comorbid depression (64). An externalized locus of control may be predictive of poor adaptation to headache pain. For example, Martin et al. (64) have shown an association between an externalized locus of control and the use of catastrophizing coping strategies. Our findings, showing a cluster of externalized locus of control, maladaptive coping strategies, disability and psychological distress in the CDH-M group, are consistent with these observations. A personalized external locus of control (physician, powerful other) may lead to excessive reliance on analgesics for self-medication of headaches, thus providing a potential mechanism for the transformation of episodic into chronic headaches (64, 66). The locus of control thus represents a cognitive representation of health and disease that should be taken into account in the treatment of subjects with migraine. Indeed, it may be possible to optimize the benefit of cognitive behavioural therapy if the representation of the locus of control is redirected before initiating therapy in subjects with a highly externalized locus of control.
This study has a number of strengths and weaknesses. Strengths include the large number of subjects and the fact that it was conducted in the general population. The use of face-to-face interviews and computer-assisted data collection enable exhaustive data to be collected, which would not have been possible using, for example, a postal survey. As a consequence, the differences in psychological factors observed are likely to be representative of headache sufferers in France. Weaknesses include the fact that the instruments used have not been extensively studied in headache populations before, so the clinical significance of the differences observed is a matter of conjecture. This limitation is compounded by the absence of a ‘no headache’ control group, which precludes evaluating how specific the observations may be to migraine headache. In addition, the cross-sectional nature of the study precludes drawing any inferences about the causality of the associations observed. Whether the psychological features are a cause or a consequence of chronicity has important implications for treatment, and this cannot be addressed in the study. As with all epidemiological surveys, bias due to the refusal of individuals to participate in the survey cannot be excluded, particularly since some of the psychological variables studied may influence willingness to participate in surveys. However, this bias could be minimized to some extent by the use of a quota method, ensuring that all sociodemographic groups were adequately represented, and by the use of an omnibus survey whereby interviewees were unaware at the beginning of the interview that they would be asked about their headaches. The use of single-item measures, such as the locus of control measure and the BIPQ dimensions, is of some concern. Such measures are less reliable for measuring a construct than a multi-item profile. Moreover, unlike multi-item scales, where random error associated with individual items tends to cancel itself out, this error may make an important contribution to variance when single-item measures are used in multiple regression models. Finally, the output from the stepwise multiple regression procedure is sensitive to the specific distribution of input variables in the sample, and thus may not be highly generalizable. This approach may also introduce type I error in later stages of the iteration, inflating the importance of certain variables. We have tried to control for potential problems associated with stepwise multiple regression by reiterating the analysis using a hierarchical model, which, at least for the most strongly associated variables, yielded similar findings. Nevertheless, the model merits replication in other samples.
The objective of this study was to identify differences in psychological factors between CDH and episodic migraine. A number of such factors have been identified, and it would be of interest to evaluate whether these factors could be combined into a single composite measure of psychological impact. A number of statistical methods are available to segregate and combine items from different questionnaires to generate a measure that discriminates two groups of interest in the most powerful way possible. For example, the HIT-6 instrument was developed in this way from a large bank of source questionnaires using item response theory (28). Such a measure could then be used to identify patients who could be targeted for psychological follow-up or behavioural interventions, or to look for correlations with other headache features that might be markers of a risk for chronicity. The evaluation of such a measure would also be helpful from a psychometric point of view, since it may be more reliable than the single-item measures used in the present study for measuring a construct.
It is important to emphasize that although cross-sectional surveys such as this can identify variables associated with headache chronicity, they can only suggest hypotheses about how such variables contribute to headache evolution. In order to evaluate these hypotheses and thus draw conclusions about causality, dedicated longitudinal studies are needed.
Headache sufferers using maladaptive coping strategies may be appropriate for targeting behavioural interventions aimed at developing more adaptive coping strategies such as acceptance and, above all, at reducing maladaptive coping strategies. In particular, our results suggest that these should aim to reduce the use of catastrophizing and avoidance strategies. Empirical support for such an approach is extensive (67), and several studies have provided evidence for the benefit of behavioural interventions in improving pain perceptions in migraine or tension-type headache (68–72). Nevertheless, further research is required to identify the most effective strategies to prevent progression of episodic to chronic headaches (73).
In conclusion, we have identified a number of psychological variables that are associated with chronic headache. These include higher levels of emotional distress as well as the use of catastrophizing and avoidance coping strategies and an externalized locus of control.
Footnotes
Competing interests
The study was initiated and finances by GSK Laboratory, France. F.N-O. and A.E.H. are employees of GSK laboratory. M.L-M., H.M., A.P. and F.R. received consultation fees from GSK Laboratory for their contribution to the design, implementation and interpretation of the study. F.M. received emoluments from GSK Laboratory for carrying out the analysis of the data.