
Abstract
The aim of this study was to evaluate determinants of consultation for migraine in a representative sample of the French general adult population. We interviewed 10 032 subjects, of whom 1534 fulfilled the International Headache Society diagnostic criteria for migraine. These were categorized into migraine, probable migraine and chronic migraine. Information was collected on consultation experience; 436 subjects (28.4%) had never consulted for headache, 473 (30.8%) were in active consultation and 625 (40.7%) had previously consulted but lapsed. Subjects with chronic migraine showed the highest active consultation rates (51.8%). All subjects completed rating instruments for headache [Headache Impact Test (HIT)-6], psychiatric (Hospital Anxiety and Depression Scale scale) and psychological [Brief Illness Perception Questionnaire (BIPQ), Brief COPE Inventory and Coping Strategy Questionnaire] variables. The strongest determinants of active consultation were BIPQ scores, HIT-6 scores and migraine type. Consultation was associated with maladaptive coping strategies (social support, emotional expression and acceptance). Determinants of remaining in consultation were catastrophizing coping scores and previous consultation experience.
Introduction
Migraine is one of the most frequently encountered forms of episodic primary headache, being particularly common in women and young adults. Recent epidemiological studies in France have identified point prevalence rates of 17% (1) and 21% (2), consistent with prevalence rates found in other industrialized countries (3).
Migraine can be an invalidating condition, associated with deteriorated quality of life (4–6), lost productivity (7, 8) and a collateral impact on the family and associates (9). The direct and indirect costs of migraine are elevated (10, 11), with the total annual direct cost of migraine in France having recently been estimated to be >€1000 million (12).
Nevertheless, efficacious treatments for migraine exist, notably since the introduction of triptans (13), and appropriate treatment has been shown to improve quality of life (14, 15), limit lost productivity (16, 17) and to be cost effective (18).
In spite of the availability of effective treatments, rates of diagnosis, consultation and treatment for migraine are low. A US study performed in 1989 revealed that only 38% of subjects in the general population who fulfilled criteria for migraine had actually received a formal diagnosis of migraine (19). This proportion had risen to only 48% 10 years later following introduction of diagnostic guidelines and more effective treatments (20). Consultation rates in migraineurs in the general population in France have been estimated at 57% in the GRIM2000 study (12), conducted in 1999, and 60% in the FRAMIG 3 study (2), conducted in 2003. Moreover, in the FRAMIG 3 study, only 34% of subjects who had consulted were still in active consultation at the time of the study. In the FRAMIG2000 study, only 18% of migraineurs were being medically followed for their headaches (21). Another study in a primary care setting revealed that only 28.4% of patients fulfilling International Headache Society (IHS) diagnostic criteria for migraine who were consulting a general practitioner for whatever reason were being treated for their headaches (22). According to the multinational MAZE study (2000), only 10% of migraineurs who had consulted for migraine were prescribed a triptan and only 36% were entirely satisfied with their treatment (23). In France, 8% of migraineurs were using triptans at the time of the GRIM2000 study in 1999 (24), and this proportion had not risen by 2003 when the FRAMIG 3 study was conducted (2).
The determinants of consultation in subjects with migraine are poorly understood. The American Migraine Study of 1989 interrogated 2479 migraineurs identified in a general population survey about consultation through a questionnaire (25). Older age, female gender and headache severity were associated with a higher probability of consultation. A study in Taiwan (26) has identified older age, low education levels, living in a rural area, the presence of associated symptoms, time off work and cardiovascular comorbidity as variables favouring consultation. In a Chilean study (27), female gender, younger age and low education levels were associated with consultation.
We have had the opportunity to explore motivations for consultation and determinants of consultation in the context of the GRIM 3 survey, a large general population-based survey of migraine in France. The principal objective of the study was to identify the determinants of consulting a physician in subjects in the French general population experiencing migraine headaches. In addition, we investigated the factors that determined whether subjects continued in medical care for their headaches after an initial consultation.
Methods
This was a descriptive epidemiological study performed in a representative sample of the French adult general population between March and May 2005. A national representative sample was screened in order to identify migraineurs, who were interviewed in depth to collect data on impact of headache, psychological aspects, comorbid anxiety or depression and healthcare resource utilization.
Make-up of the study sample
A representative sample of the French adult population reporting headache was formed by face-to-face interview with a target population of 10 000 individuals aged ≥18 years representative of the national population in terms of gender, age, employment status, place of residence (nine geographical regions and five community size classes) according to the most recent census data from the French National Statistics Office (INSEE, 1999). A quota method was used to ensure uniform representation of each socio-economic category in the final sample.
Interviews
Face-to-face interviews were conducted in the subject's home by trained interviewers from Institut de Sondage Lavialle, an international polling institute, as part of an omnibus survey that asked specific health-related questions within a much wider multisubject questionnaire. This system is thought to provide greater motivation and more neutral responses to questions on medical subjects. The CAPI/POLLUX (Computer Assisted Personal Interview) system was used to ensure exhaustive, accurate and unambiguous data collection. Thirteen screening questions were asked during the interview in order to identify individuals with migraine. Replies to these questions allowed a diagnosis of migraine made.
Attribution of headache diagnosis
A diagnostic algorithm was used to attribute one of three headache diagnoses on the basis of replies to the screening questions and the revised IHS criteria for headache classification (28). These three types of headache were migraine (IHS categories 1.1 or 1.2, referred to as ‘strict migraine’), probable migraine (IHS category 1.6) and chronic daily headache with migrainous features (CDH-M). The diagnostic algorithm used for strict and probable migraine has been described in our previous national migraine prevalence survey (1). In the case of CDH-M, subjects were required to fulfil both criteria C and D for migraine without aura (IHS 1.1) and a specific chronicity criterion. This chronicity criterion diverged from that used in the previous studyto take into account the new IHS classification. In the present study, the chronicity criterion for CDH-M was headache on >15 days/month during >3 months (corresponding to IHS category 1.5.1, chronic headache). In our previous study, the corresponding definition for CDH-M was headache on 30 days/month. It should be noted that this information was obtained from general declarative data from the participants, namely positive replies to two questions ‘Do you suffer from headaches?’ and ‘Do these headaches occur on more than 15 days per month during more than three months?). Headache diaries were not used to collect prospective data.
Data collection
Individuals identified as having migraine headaches were further interrogated about their migraine in a subsequent part of the same interview and a number of psychometric rating scales were completed. These were the six-item Headache Impact Test (HIT-6) (29, 30), the Hospital Anxiety and Depression Scale (HAD) (31, 32), the catastrophizing subscale of the Coping Strategy Questionnaire (CSQ) (33), the Brief COPE Inventory (34, 35) and the Brief Illness Perception Questionnaire (BIPQ) (36), all used in their French translations. Extensive data for the psychological rating scales are provided in the Appendix.
Information was also collected on physician consultations for headaches. Subjects were asked if they had ever consulted for their headaches and, if so, whether they had done so in the previous year. Reasons for consultations were identified using predefined response categories. The time between first symptoms and the initial consultation was recorded. Data on consultations will be the focus of the present report.
For subjects having consulted for their headaches, a treatment satisfaction score was derived using an ad hoc questionnaire designed for this study. This was calculated as the sum of reply scores to the following five questions: (i) ‘Is medical treatment useful for combating headaches?’; (ii) ‘Do doctors take your headaches seriously?’; (iii) ‘Does your doctor listen to you about headache problems?’; (iv) ‘Does your doctor take the time to explain your headache treatments to you?’; and (v) ‘Are you satisfied with the way your doctor treats your headaches?’. There were four response modalities for each question, corresponding to a four-point Lickert scale ranging from 1 (yes, very much) to 4 (no, not at all). Possible scores could thus range from 5 (most satisfied) to 25 (least satisfied).
Statistical analysis
Preliminary statistical power calculations were performed in order to determine the number of subjects to include. In order to identify a determinant of consultation present in ≥15% of subjects associated with an odds ratio (OR) of ≥1.5, and with an α risk of 0.05 and a statistical power (β risk) of 80%, it would be necessary to evaluate ≥1577 subjects with migraine. Given a prevalence of migraine in the general population of 17% (1) and a loss of 7% due to lack of exploitable data, it would be necessary to screen 10 000 individuals in the general population.
Three study populations were identified: subjects who had never consulted for migraine (non-consulting group, NC), subjects who had consulted at some time in the past but had not done so in the year preceding the survey (lapsed consultation group, LC) and subjects who were still in consultation at the time of the survey (active consultation group, AC). Pairwise comparisons were made between the NC group and the combined LC + AC group (consulting group, C) and between the LC and AC groups.
Categorical variables were compared with the χ2 test or with Fisher's exact test in case of low (<5 in any group) sample size, ordinal variables by the Kruskal–Wallis test and quantitative variables by the Mann–Whitney U-test or by analysis of variance. ORs with 95% confidence intervals (CIs) were determined where appropriate.
Variables whose distribution varied between the consultation groups at a probability level of 0.10 were retained for an exploratory stepwise multivariate logistic regression analysis. ORs with 95% CIs were determined from the final model for each variable.
Two-sided statistical tests were used throughout and a probability level of 0.05 was considered statistically significant. All data were analysed centrally using software from SAS (Cary, NC, USA; version 8.2).
Ethics
The study was performed according to international and French regulatory guidelines and current codes of Good Epidemiological Practice. Since patient care was not altered by inclusion in the study, ethics committee approval was not necessary. With respect to data confidentiality, the study was declared to the Commission Nationale d'Informatique et Libertés.
Results
Subjects
During the screening phase, 10 032 subjects were interviewed. Of these, 2740 reported suffering from headaches, 1534 of whom fulfilled diagnostic criteria for migraine. When asked about medical consultation for migraine, 28.4% of migraineurs reported that they had never consulted for their headaches and 40.7% that they had not consulted over the previous year (Fig. 1). The remaining 473 subjects (30.8%) were in active consultation at the time of the study. The probability of consulting compared with never consulting and of remaining in consultation compared with no longer being in consultation varied significantly across diagnostic groups (P < 0.001; χ2), with subjects with CDH-M having the highest active consultation rates and those with probable migraine the lowest (Table 1). The demographic characteristics of the study sample are presented in Table 1. The majority of subjects were female (77.8%) and young adults (mean age 40.5 years).

Subject populations evaluated in the study. The percentages are calculated with respect to the 1534 migraineurs.
Consultation status according to age, gender and migraine diagnosis
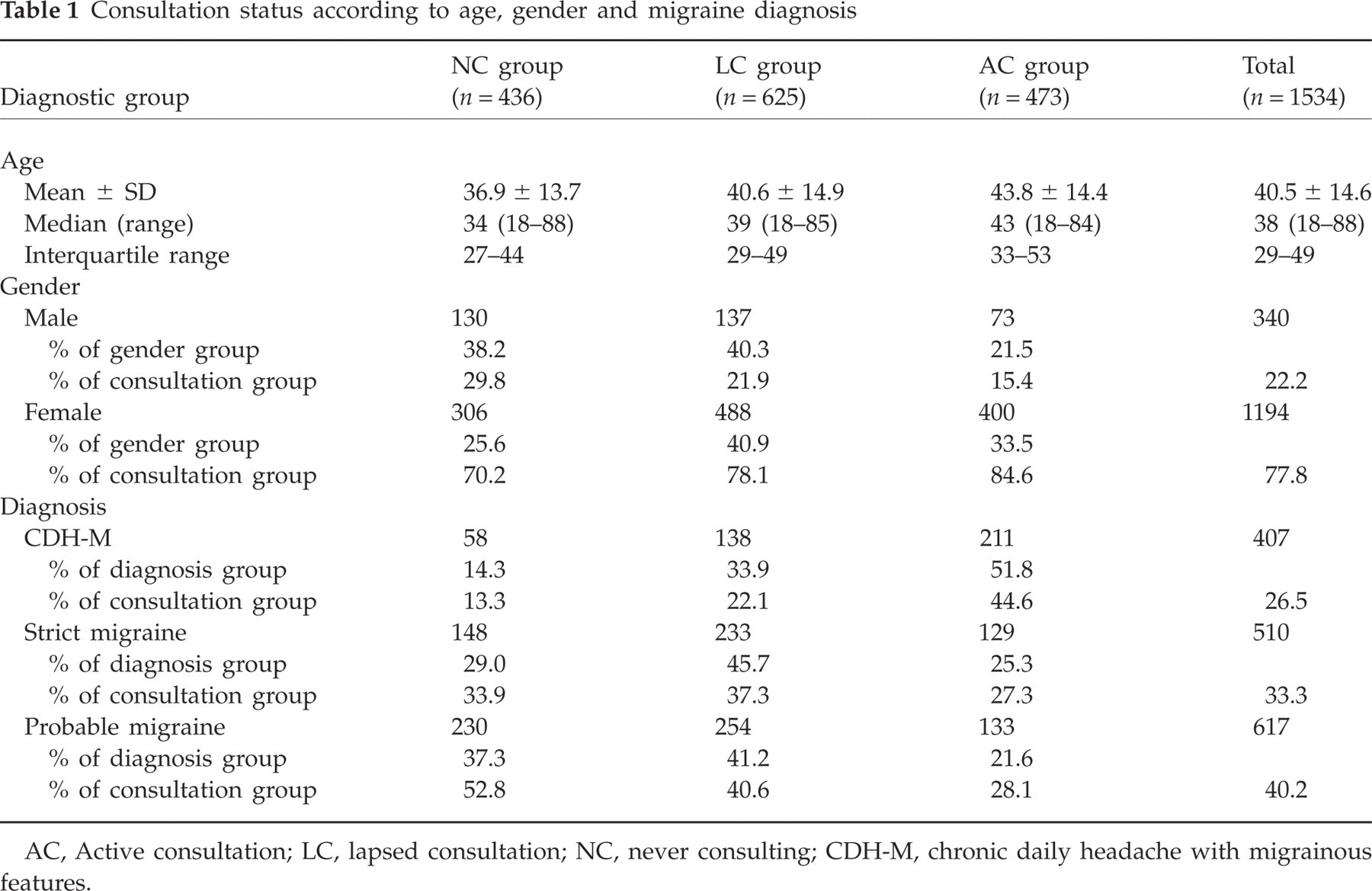
AC, Active consultation; LC, lapsed consultation; NC, never consulting; CDH-M, chronic daily headache with migrainous features.
Reasons for consultation
For patients who did not consult, the reasons for not doing so were principally related to self-medication, insufficiently frequent headaches and scepticism about the potential benefit of consultation (Table 2).
Reasons for not consulting for migraine headache

More than one reason could be cited.
OTC, Over the counter.
For patients who did consult, most (54.6%) did so within 1 year of the onset of the headache pathology. This proportion was higher in those patients who were still in active consultation (65.8%) compared with the lapsed consultation group (42.9%). Headache was the principle reason for consultation in 67.7% of cases. In 69.8% of cases, a diagnosis of migraine was given during the first consultation.
For patients who did consult, headache severity, frequency and duration were the most frequently cited reasons (Table 3). Most subjects consulted on their own initiative (82.2%) or following advice from friends or family (18.4%).
Headache features leading to consultation for migraine headache

More than one reason could be cited.
Univariate analysis of consultation patterns
All sociodemographic and clinical variables collected, as well as scores on all the psychometric rating scales completed, were tested for association with likelihood of lifetime consultation (NC vs. LC + AC groups) and of active consultation (LC vs. AC groups).
Sociodemographic variables associated with a higher probability (P < 0.05) of lifetime consultation and of remaining in active consultation were female gender, older age groups, being retired or otherwise professionally inactive, being divorced or separated, having a higher level of education and living in rented or collective (i.e. apartment) accommodation. Living in communities of small population size was associated with a higher probability of ever consulting but not of remaining in active consultation. Income was a specific determinant of the probability of remaining in active consultation, this being higher in subjects with lower incomes (<€1220/month).
Consultation rates differed markedly according to migraine headache type (Table 1), with subjects with CDH-M making up 51.8% of the active consultation group. In contrast, 52.8% of subjects who had never consulted fell into the probable migraine group (47.2%). In addition, subjects who reported suffering from other types of headache also were more likely to have consulted a physician for migraine headache (14.8% of subjects in the LC + AC group compared with 11.5% in the NC group; P = 0.089). Later onset of headache duration was associated with a higher probability of being in active consultation. In the LC group, 56.3% were aged <20 years at the time of headache symptom onset compared with 43.7% in the AC group.
Greater headache impact as measured with the HIT-6 was associated with an increased probability of having ever consulted and still being in consultation (Table 4). The proportion of subjects with substantial or severe impact (HIT-6 score >55) was nearly twofold higher in the AC group than in the NC group. An increased probability of having ever consulted and still being in consultation was also observed in subjects with clinically relevant anxiety (HAD anxiety score >8). Clinically relevant depression (HAD depression score >8), in contrast, was associated with a higher probability of remaining in active consultation, but not with that of ever having consulted. Higher scores on the BIPQ score, the CSQ catastrophizing scores, as well as high social support, emotional expression, avoidance and religion scores and low acceptation score on the Brief COPE Inventory, were associated with an increased probability of having ever consulted and still being in consultation. Higher treatment satisfaction scores were associated with a higher probability of no longer remaining in consultation.
Rating scale scores predictive of consultation identified in univariate analysis

NC, Never consulting group; LC, lapsed consultation group; AC, active consultation group.
Probability values in bold (<0.10) correspond to values retained for the multivariate analysis.
A number of consultation-related variables were associated with a higher probability of remaining in active consultation. For example, a delay of <1 year between headache onset and consultation was more frequently reported by patients in active consultation (68.1% of subjects compared with 44.4% in the LC group; P < 0.001). Headaches were more likely to be the principal reason for consultation for patients still in active consultation (72.0% of subjects in the AC group compared with 64.4% in the LC group; P = 0.009). Those subjects who were provided with a diagnosis during the first consultation were more likely to have lapsed (72.1% of subjects in the LC group compared with 67.0% in the AC group; P = 0.07), as were subjects who consulted on the advice of their family or friends rather than on their own initiative (73.0% of subjects compared with 12.3% in the AC group; P < 0.001). Satisfaction with the headache management offered by the physician was also higher in patients in active consultation (60.5% of subjects in the AC group reported being very satisfied compared with 48.3% of subjects in the LC group; P < 0.001).
Multivariate analysis of consultation
The variables identified in the univariate analysis were entered into a stepwise multivariate logistic analysis to eliminate covariates. This model retained nine variables as determinants of lifetime consultation (Table 5). The mean total score on the BIPQ was the strongest determinant. The only sociodemographic variables that were retained were age, population size of the community and homeowner status. Migraine diagnosis and headache impact were determinants of consultation. Among the psychological variables, scores on the Brief COPE social support and emotional expression, acceptance and positive reinterpretation dimensions were retained.
Variables predictive of consultation identified in multivariate analysis ranked in order of appearance in the stepwise model

Odds ratios correspond to the probabilities of having ever consulted (AC and LC groups combined) compared with never having consulted (NC group). Response modes shown in italics did not provide odds ratios significantly different from unity with respect to the reference response mode.
The variables identified as determinants of active consultation on multivariate analysis differed from those identified for consultation per se (Table 6). The only shared variable was headache diagnosis. The strongest determinant of active consultation was the CSQ catastrophizing score. More rapid consultation and headache duration and frequency as reasons for consulting were associated with increased probability of staying in consultation, whereas consulting on the advice of another was associated with a higher chance of relapse. Treatment satisfaction (lower treatment satisfaction scores) was associated with a higher probability of remaining in active consultation. Retired and invalid subjects were more likely to remain in consultation, as were subjects in lower income brackets, whereas students and the unemployed were more likely to relapse.
Variables predictive of active consultation identified in multivariate analysis ranked in order of appearance in the stepwise model

Odds ratios correspond to the probabilities of being still in active consultation (AC group) compared with being no longer in consultation (LC group). Response modes shown in italics did not provide odds ratios significantly different from unity with respect to the reference response mode.
Discussion
This study has revealed that, in a sample of 1534 individuals fulfilling diagnostic criteria for migraine identified in the French general population, 30.8% were in active consultation for migraine and 71.6% had consulted at some time during their lives. These figures are somewhat higher than in previous general population studies in France (2, 12), where lifetime consultation rates of around 60% were reported. Consultation rates were highest in patients assigned a diagnosis of CDH-M and lowest in those assigned a diagnosis of probable migraine, in agreement with the two previous studies in France (2, 37).
The principal motivations for consultation given were headache features such as duration, severity and frequency. This is in agreement with the findings of the American Migraine Survey (25). The principal motivations for not consulting were satisfaction with self-medication, relative tolerability of headaches and the belief that consultation would be of no use. The majority of subjects claimed to consult on their own initiative rather than on the advice of someone else.
A large range of sociodemographic, clinical and psychological variables was investigated for association with probability of consultation. This is the first time that this has been investigated in a European population, although general population data for some of these variables are available for Taiwan (26), USA (25) and Chile (27). Identified sociodemographic variables associated with a greater probability of consultation were older age, owning one's own home and living in small communities. Age and small communities were also identified in the Taiwanese study (26) and age in the American study (25). In contrast, the Chilean study (27) found that younger subjects were more likely to consult. The extent and determinants of home ownership are likely to be highly variable between different countries. On the other hand, no association between income level and consultation was observed, suggesting no economic barriers for access to healthcare for people with migraine in France. This contrasts with many other pathologies, where people with low incomes or living in rural areas are underprivileged in terms of access to healthcare (38, 39).
The only clinical variable that influenced consultation was the HIT-6 score, with patients reporting greater impact being more likely to consult. An association between consultation and HIT-6 scores has also been suggested in a previous study of the properties of the HIT-6 instrument in France (22). Taken together with the higher probability of consulting in patients with the most severe headache types, this observation suggests that those patients most in need of care are in fact receiving it and thus that healthcare supply in migraine effectively targets the most unwell.
Psychological variables were chosen to cover three principal domains of attitude to disease, namely coping strategies, illness perceptions and locus of control. The questionnaires were chosen to be sufficiently brief and simple to use to be administered as part of a battery of questions by a lay interviewer and were required to be available in a validated French translation. Although these instruments have not been used widely in migraine studies, they have been used extensively in a wide variety of other pathologies. The BIPQ is the short form of the standard instrument to evaluate illness perceptions. The Brief COPE is a widely used concise rating scale for cognitive and behavioural coping strategies, which covers all dimensions of coping with the exception of catastrophization. The CSQ catastrophization items were added to the test battery to cover this aspect. Extensive data on psychological variables obtained from this study will be published elsewhere.
Amongst the psychological variables, the BIPQ score and three coping strategies (subjects with high scores on the acceptance and on the social support and emotional expression dimensions of the Brief COPE) and low scores on the positive reinterpretation dimension were associated with a higher probability of consultation. The BIPQ, which measures cognitive representations of illness severity, together with the scores on the HIT-6 score, which is a measure of migraine severity itself, were the two strongest determinants of consulting. Acceptance, social support and emotional expression, which are considered as ‘passive’ coping strategies, have frequently been associated with inadequate functional and psychosocial adaptation to chronic pain (40). A recent study in students with migraine has found that beliefs about social support are also associated with consulting for migraine (41).
This suggests that patients with maladaptive coping strategies are more likely to consult for migraine, and also that consulting is not considered by the patient as a problem-solving strategy leading to establishing a therapeutic alliance with the physician, but rather as a passive request for help. Physicians should be aware of this and take the opportunity of talking to patients about coping with headache.
Physicians should also evaluate the emotional dimension of headache during consultations and, if necessary, address this. Pharmacological treatments should be restricted to patients fulfilling diagnostic criteria for depression or anxiety disorders. It may be helpful for physicians, particularly in the case of migraine specialists, to be familiar with and implement the most common standard psychosocial interventions. If emotional distress cannot be managed directly by the physician, referral to a psychotherapist or clinical psychologist should be considered. Psychosocial support, including cognitive behavioural therapy, can be proposed to help patients cope better with their migraine headaches, in particular focusing on reducing catastrophization. Patients should be helped to consider their migraine as a treatable condition. In addition, developing self-management training skills may be useful in helping patients take responsibility for their headache management and increase their sense of control over their illness, which is associated with better outcome (42, 43). Importantly, the physician should be prepared to change the headache treatment if an appropriate response is not obtained.
Surprisingly, measures of anxiety and depression with the HAD were not associated with consulting. This may be because the HAD identifies state rather than trait anxiety and depression, which may be less well correlated with sustained behaviour patterns than a trait marker. In this context, it might have been more appropriate to use a questionnaire that measures lifetime psychiatric symptomatology more accurately. Nevertheless, the HAD has been widely used in the past in studies of pain and headache. Alternatively, HAD scores may be close covariates of coping strategies and thus may not be identified independently from these in the multivariate analysis. The observation of a significant association between HAD anxiety scores and consulting in the univariate analysis would be consistent with this hypothesis.
In addition, factors associated with remaining in consultation were analysed. This aspect of consultation has not been investigated in previous studies. Interpretation of this analysis should, however, take into account that the population of lapsed consulters is likely to include both patients who found a satisfactory response to their headaches and no longer feel the need to consult and patients who were unsatisfied with the treatment offered. The former group may be revealed in our sample by the higher proportion of patients in the LC group compared with the AC group who received a diagnosis of migraine at their first consultation, and the lower proportion who consulted primarily for their headaches. The latter patient group can be recognized in the higher treatment satisfaction scores (i.e. less satisfied) in the LC group compared with the AC group.
In contrast to the determinants of consultation, staying in consultation is not driven by headache severity (as measured by the HIT-6 scores) or by coping variables with the exception of catastrophizing. Catastrophizing has been considered as being related to emotional distress (44) and may thus covary with the HAD depression and anxiety scores that were identified in the univariate analysis. On the other hand, particular patterns of first consultation seemed to be important, such as a short delay to initial consultation, duration and frequency of headaches as a motivation to consult, and a decision to consult taken by the subjects themselves rather than acting on advice from someone else. This last observation has been made previously in other pathologies. Income was also identified as a significant associated variable, with patients on low incomes being more likely to remain in active consultation. The explanation for this observation is unclear. The other sociodemographic variable associated with being in active consultation was employment status, with active consultation being more likely in subjects who were retired, invalid or not working, and less likely in students and those out of work. This pattern reflects consultation patterns in the general population and is not specific for migraine.
The results obtained raise many questions which were not addressed in the study, such as differences in consulting patterns between primary and specialist care, the influence of treatment outcome on consultation patterns, attitudes to care or disease perceptions, and the role of family members with migraine on attitudes to care. These would be interesting to investigate in future studies.
In conclusion, this study demonstrates that consultation rates for migraine in the French general population are relatively high. The strongest determinants of consultation were headache severity and perceptions of headache. Sociodemographic variables appear to play a less important role. Moreover, consultation seems to be associated with maladaptative coping strategies, indication the importance of addressing educational and behavioural management.
Competing interests
This study was initiated and financed by GSK Laboratory, France. F.N-O. and A.E.H. are employees of GSK laboratory. M.L-M., H.M., A.P. and F.R. have received consultation fees from GSK Laboratory for their contribution to the design, implementation and interpretation of the study. F.M. has received emoluments from GSK Laboratory for carrying out the analysis of the data.
Appendix: Additional information on rating scales
Hit-6
The HIT-6 instrument is a six-item questionnaire which yields an impact score on a linear scale with minimum and maximum possible values of 36 and 78, respectively. On the basis of this score, subjects can be assigned to one of four impact grades. These are little or no impact (Grade 1; score ≤49), moderate impact (Grade 2; score 50–55), substantial impact (Grade 3; score 56–59) and severe impact (Grade 4; score ≥60).
HAD
The HAD is a 14-item questionnaire assessing severity of anxiety and depression, seven items relating to anxiety and seven to depression and each scored on a four-point Lickert scale. Possible scores for each pathology dimension range from 0 to 21, with a higher score reflecting greater severity. A score >8 on either score corresponds to clinically relevant anxiety or depression.
CSQ
The CSQ was designed to evaluate cognitive and behavioural coping strategies in chronic pain syndromes, and contains several dimensions and subscores. The Catastrophization subscore of the CSQ was used in the present study It contains four items each scored on a four-point Lickert scale, yielding a total score ranging from 4 to 16, with higher scores indicating greater difficulty coping.
Brief COPE
The Brief COPE was developed to assess the different ways in which people respond to stress. It contains 14 scales of two items each which measure conceptually distinct aspects of coping, nine reflecting functional strategies and five reflecting dysfunctional strategies. Each item can be scored on a four-point Lickert scale. The total scores on each scale were normalized on a scale of zero to 100.
BIPQ
The BIPQ investigates cognitive perceptions of illness and contains eight items scored on a 10-point Lickert scale and a ninth open-response item. The sum of the mean scores on the eight items is used to generate the total BIPQ score.