
Abstract
The objectives of the SMILE study were to assess anxiety, stress, depression, functional impact and coping behaviours in migraine patients consulting in primary care in France. General practitioners (n = 1467) and 83 neurologists included 5417 consulting migraine patients. Of these patients, 67± were found anxious, of whom 59± were also depressive. Patients with both anxiety and depressive dimensions showed a profile similar to that of chronic migraine patients (severe attacks, poor treatment effectiveness and pronounced stress, functional impact and maladaptive behaviours). A quantitative progression in the levels of stress, maladaptive coping behaviours and functional impact was noted from patients with neither dimension to those with both anxious and depressive dimensions. Stress and maladaptive coping strategies were found to be major determinants of anxiety. Anxious and depressive dimensions were associated with elevated consumption of acute treatments for migraine and low treatment effectiveness. Stress and anxiety should be looked for carefully in migraine patients.
Introduction
Comorbidity of migraine with diverse psychiatric conditions has long been recognized, especially with major depression and anxiety disorders (particularly panic and phobia) (1), and stress is frequently considered to precipitate and exacerbate migraine (2). Population-based cross-sectional studies of prevalence of psychiatric disorders among migraineurs have found increased risks of generalized anxiety (3, 4), panic and major depressive disorders (3–7). A US population-based study reported a 2.7-fold increase in the prevalence of depression among migraine patients compared with non-migraine controls (8), whereas a French nationwide postal survey found a 1.7-fold increase in the prevalence of anxiety and depression (9). Moreover, several works have indicated that psychiatric comorbidity may occur before migraine onset (4, 10) and that it may constitute a risk factor for the evolution from migraine to medication overuse headache (11). On the other hand, recurrent and intense pain may lead to anticipatory anxiety, perceived loss of control and other behavioural or cognitive risk factors for psychiatric syndromes. Therefore, a bidirectional chronology may exist between migraine and psychiatric disorders (5, 7). Results from clinical samples of migraine patients have confirmed that migraine patients more often suffer from anxiety and depression than non-migraine patients. Moreover, these studies have shown that patients with chronic migraine exhibit anxiety and depression more often than those with episodic migraine (12).
Because they add to the burden that migraine inflicts on patients (13, 14), taking psychiatric disorders into account is warranted for adequate migraine evaluation and management and prevention of medication overuse. The objectives of the SMILE study were to evaluate stress, anxiety and depression in the population of migraine patients consulting in primary care and to analyse the potential relationship between anxiety and migraine severity, stress, quality of life and effectiveness of acute migraine treatments. Since there is a relationship in migraine patients between affective disorders (depression) and emotional adjustment (15), the adjustment strategies used to cope with migraine and their relationship to anxiety and stress were also assessed.
Methods
Study design, patient inclusion criteria
SMILE was an office-based, observational study carried out in France by the opinion poll institute TNS Healthcare from November 2005 to July 2006 among general practitioners (GPs) and neurologists. Four thousand physicians were recruited by mail or telephone from a physician database.
Each participating physician was to include, from the date of start of the study, the first four patients consulting for migraine who were aged ≥ 18 years and not currently treated with a prophylactic treatment (because one of the study objectives was to assess prospectively the effects of migraine prophylactic agents on the impact of migraine; these data will be reported in a subsequent article). Patients receiving anxiolytic or antidepressant therapies were not excluded, in order to preserve the representativeness of the study population compared with the population of migraine patients usually consulting in private medical practice. Only patients fulfilling the diagnostic criteria for strict or probable migraine according to the International Classification of Headache Disorders (ICHD-II) were included (16).
Study questionnaires
Physicians completed a questionnaire about personal demography and professional activity. Patients completed a 50-item questionnaire about socio-demography, ICHD-II migraine diagnostic criteria, migraine history and impact on everyday life, existence of affective disorders, stress, coping strategies using psychometric tests (see below), the treatments used for treatment of migraine attacks and their perceived effectiveness.
French validated versions of psychometric scales were used to assess affective disorders, migraine functional impact and coping behaviour. Anxious and depressive dimensions of affective disorders were measured using the Hospital Anxiety and Depression (HAD) scale (17, 18), originally designed for the evaluation of anxiety and depression in patients hospitalized for somatic causes (17). The French version of the HAD scale has been validated in patients hospitalized in an internal medicine department (19). Scores of ≥ 8 were considered to characterize anxiety and depression. This threshold is associated with 82% sensitivity and 94% specificity for anxiety (19) and with 70–78% sensitivity and 68–80% specificity for depression (19, 20). Stress was assessed using the abridged form (PSS4) of the original Perceived Stress Scale questionnaire (21), the most widely used psychological instrument for measuring the perception of stress. Functional impact of migraine was assessed using an abridged version (MSQ4) of the original Migraine-Specific Quality of life questionnaire developed to allow easy use of the questionnaire in general practice (22, 23). Maladaptive avoidance coping strategy was evaluated using the behavioural disengagement subscale of the Brief Coping with Problems Experienced (COPE) inventory (24–26). Brief COPE has been validated in a population of breast cancer patients (27). Maladaptive pain coping strategy was evaluated using the catastrophizing subscale of the Coping Strategies Questionnaire (CSQ) (28, 29). The French version of CSQ has been validated in patients consulting for chronic pain (30). No formal diagnosis of anxiety or depression was made by the study physicians.
Evaluation of acute treatment effectiveness
Effectiveness of the usual treatment of migraine attacks was assessed using the set of four questions designed by the French Society for the Study of Migraine Headache (SFEMC) that enquires about significant migraine relief 2 h after drug intake, treatment tolerability, use of a single drug unit for treatment of an attack, and rapid resumption of normal social, family or professional activities (31). A single ‘No’ response to one of the four questions characterized ineffective acute treatment. Triptans, aspirin combined with metoclopramide, and ergotamine derivatives were considered specific treatments of migraine. Paracetamol, non-steroidal anti-inflammatory drugs, opioids and aspirin alone were considered non-specific treatments.
Data analysis
The percentages of patients with anxious and/or depressive dimensions were expressed as the relative proportions of patients exhibiting HAD anxiety or depression scores of ≥ 8 (both scales spanning the range of 0–21). The PSS4 score was the sum of scores from 1 to 5 on the four items of the questionnaire (scale span 4–20). The MSQ4 score was the mean of scores from 0 to 100 on the four items of the questionnaire (scale span 0–100; low scores corresponding to pronounced functional impact). The Brief COPE avoidance score was the sum of scores from 1 to 4 on the two items of the questionnaire (scale span 2–8). The CSQ catastrophizing score was the sum of scores from 1 to 4 on the four items of the French version of the questionnaire (scale span 4–16) (30). Severity of treated attacks of migraine was evaluated by the patients on a scale of 0–10.
Quantitative variables were described by the mean and standard deviation (
A principal-components analysis (PCA) followed by mixed classification and hierarchical cluster analysis was used to identify homogeneous groups of migraine patients. Thirteen variables (sex, age, migraine history duration, number of days with headache per month, type of migraine—episodic or chronic—severity of treated attacks, number of medication units taken for an attack, treatment effectiveness according to the SFEMC set of questions, PSS4 score, MSQ4 score, COPE avoidance score, CSQ catastrophizing score, presence or absence of mood disorder—anxious or depressive dimension alone, both, or neither anxious nor depressive dimension) were entered in the PCA analysis. From the factor analysis, eight main factorial axes were retained for the subsequent typology analysis.
Independent predictors of anxious dimension were identified using logistic regression analysis allowing for the effects of sex, age, migraine history duration, number of days with headache per month, severity of treated attacks, PSS4 score, MSQ4 score, avoidance score, catastrophizing score, and number of drug units taken for treatment of an attack. Results of the regression analysis are given as the odds ratios and 95% confidence intervals of factors showing a statistically significant effect.
Only for demography and disease history have patients’ characteristics been described separately for patients consulting a GP and those consulting a neurologist. Analyses of mood disorders were performed on the combined groups of study patients.
Statistical results were considered significant or not significant (NS) at P < 0.05 or P > 0.05, respectively.
Results
The 1618 physicians (39.9% of all physicians recruited) who agreed to participate in the study included a total of 6109 patients. After exclusion of 329 patients for incomplete data (one or more missing questionnaires), of 17 patients who returned blank questionnaires, and of 346 patients not satisfying inclusion criteria [age < 18 years, n = 4; non-migrainous according to International Headache Society (IHS) criteria, n = 124; receiving prophylactic treatment for migraine, n = 218], a total of 5417 patients included by 1550 physicians (1467 GPs and 83 neurologists) remained for analysis.
Study populations of physicians and patients
Mean age of GPs (49.0 ± 7.4 years), age class distribution and regional distribution were comparable to the national reference, whereas the men to women ratio was slightly higher than the national reference (82 vs. 76%; P < 0.01). Mean age of neurologists (47.0 ± 8.3 years), age class distribution, sex ratio and regional distribution were also generally comparable to the national reference. The mean number of migraine patients seen in a month was 15.1 ± 11.8 for GPs and 25.2 ± 22.2 for neurologists (P < 0.01).
Of the 5417 patients included in the study, 5169 (95%) consulted a GP and 248 (5%) a neurologist. Most of them (80%) were women (80% of those consulting a GP; 83% of those consulting a neurologist). Mean age was 41.4 ± 12.4 years and significantly greater (P < 0.01) for patients consulting a GP (41.6 ± 12.3 years; fewer patients aged 18–24 years) compared with those consulting a neurologist (36.8 ± 11.9 years; fewer patients aged 55–64 years). Nevertheless, more patients consulting a neurologist had a long history duration of migraine (> 10 years) compared with those consulting a GP (47 vs. 32%; P < 0.01). Overall, mean migraine history duration was 10.9 ± 9.6 years.
Characteristics of migraine in study patients
According to IHS criteria, 4922 patients (91%) had strict migraine and 495 (9%) had probable migraine. Intensity of migraine attacks was considered mild by 3% of patients, moderate by 38% or severe by 66% (some patients had attacks of variable intensity). Mean number of days with headache per month was 7.5 ± 5.0 (range 1–31 days) and 517 patients (9%) had chronic migraine (≥ 15 days with headache per month).
Anxious and depressive dimensions, stress and coping strategies in study patients
According to the scores on the HAD scale, 66% of patients were considered anxious, of whom 59% were also depressive, and 31% were considered neither anxious nor depressive (Table 1). Only 2% were considered only depressive. As most depressive patients are also anxious, the small group of patients with depressive dimension alone was not detailed further. Twelve per cent of anxious migraine patients had chronic migraine (9% of migraine patients with anxiety alone vs. 15% of those with both anxiety and depression; P < 0.01) compared with only 5% of migraine patients with neither anxiety nor depression (P < 0.01).
Patient anxious and depressive dimensions, stress, functional impact and coping strategies in consulting migraine patients as assessed using psychometric tests

P < 0.01 vs. patients with neither anxious nor depressive dimensions.
P < 0.01 vs. patients with anxious dimension alone.
The small differences in numbers of patients according to the psychometric test are due to incomplete records for some patients.
Mean anxiety and depression scores, as well as mean scores for stress, migraine functional impact and maladaptive coping strategies (avoidance, catastrophizing) in all evaluable patients and in the different subgroups of patients with or without mood disorders are presented in Table 1. Results indicate that patients with anxious dimension, and especially those with both anxious and depressive dimensions, had significantly worse scores on all psychometric tests for stress, functional impact and maladaptive coping strategies than those with neither anxious nor depressive dimensions.
The relationship between stress or coping strategies and mood disorders is depicted in Fig. 1. Stress score increased progressively from the group of patients with neither anxious nor depressive dimensions to the group of patients with anxious dimension alone and then to the group of patients with both anxious and depressive dimensions (P < 0.01). Similarly, avoidance and catastrophizing scores increased significantly from the group of patients with neither anxious nor depressive dimension to the group with both anxious and depressive dimensions (both P < 0.01). Conversely, MSQ4 score decreased progressively from the group of patients with neither anxious nor depressive dimension to that with both psychiatric dimensions (P < 0.01) (Fig. 2).
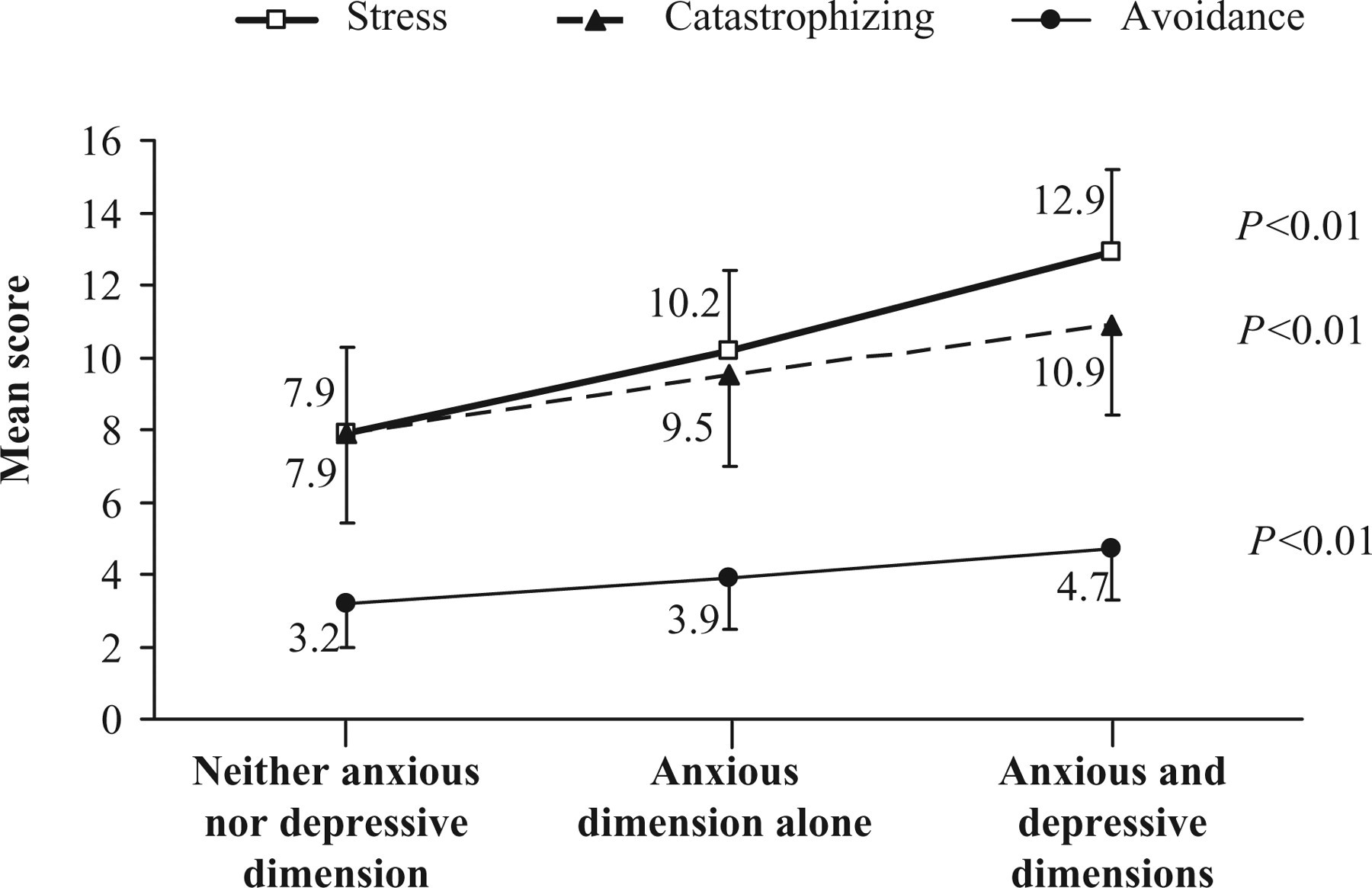
Increase in mean stress, avoidance and catastrophizing scores in the Perceived Stress Scale (PSS) 4 questionnaire, disengagement subscale of the Brief Coping with Problems Experienced (COPE) inventory and catastrophizing subscale of the Coping Strategies Questionnaire (CSQ) questionnaire, respectively, according to the absence or existence of anxious dimension, alone or combined with depressive dimension, in migraine patients consulting in primary care. Statistical significance refers to the progressive increase in each score in the three groups of patients.

Decrease in mean score of migraine impact on everyday activities in the MSQ4 questionnaire according to the absence or existence of anxious dimension, alone or combined with depressive dimension, in migraine patients consulting in primary care. Statistical significance refers to the progressive decrease in MSQ4 score in the three groups of patients. MSQ4, abridged version of the original Migraine-Specific Quality of life (MSQ) questionnaire (22, 23).
Typology of consulting migraine patients
A total of 5067 migraine patients with assessable data at the HAD, PSS4, MSQ4, Brief COPE inventory avoidance and CSQ catastrophizing scales were included in the typology analysis. Four homogeneous groups of migraine patients could be discerned (Table 2).
Typology of consulting migraine patients according to migraine characteristics and the existence of anxious or depressive dimension or both, as determined by principal components analysis followed by mixed classification and hierarchical cluster analysis (N = 5067 patients)

Percentage of patients in each group.
Mean value.
PSS4, Perceived Stress Scale 4; COPE, Coping with Problems Experienced; CSQ, Coping Strategies Questionnaire; MSQ4, Migraine-Specific Quality of life 4.
Most patients in Group 1 (98%) exhibited both anxious and depressive dimensions. They had a medium migraine history duration, number of days with migraine headache per month and severity of migraine attacks. They used many drug units per attack, often non-specific drugs with very poor treatment effectiveness. These patients exhibited elevated stress scores, used pronounced maladaptive coping behaviours and experienced pronounced functional impact of migraine.
Most patients in Group 2 (92%) exhibited the anxious dimension alone. Compared with patients in Group 1, they used slightly fewer drug units per attack with slightly better effectiveness, experienced less stress and functional impact of migraine, and used less maladaptive coping behaviours.
Most patients in Group 3 (98%) exhibited neither anxious nor depressive dimension. They had slightly less severe migraine attacks, used fewer drug units per attack and less maladaptive coping behaviours and experienced better treatment effectiveness, less stress and milder functional impact of migraine.
Finally, all patients in Group 4 (100%) had chronic migraine. More than half of them (58%) showed both anxious and depressive dimensions. They reported a slightly longer migraine history duration, exhibited the highest number of days with migraine headache per month and greatest severity of migraine attacks. They took many drug units per attack, mostly non-specific treatments and seldom specific treatments and triptans, with very poor treatment effectiveness. Like patients in Group 1, they showed a high level of stress, used pronounced maladaptive coping behaviours and experienced marked functional impact of migraine.
Predictive factors of anxious dimension
Logistic regression analysis indicated that PSS4 score (P < 0.0001), avoidance score (P = 0.0003), catastrophizing score (P < 0.0001), number of days with headache per month (P = 0.0004), number of drug units taken for the treatment of an attack (P < 0.01) and migraine history duration (P < 0.05) were positively associated with the anxious dimension. On the other hand, a high MSQ4 score (P = 0.0005) was found associated with a reduced risk of anxious dimension (Table 3). The other factors studied (sex, age, severity of attacks) were not found significantly predictive of the anxious dimension.
Predictive factors of anxious dimension in migraine patients

PSS4 indicates abridged form of the original Perceived Stress Scale questionnaire (21).
Medical management of migraine
Most patients stated that they used to take acute treatments of migraine attacks (Table 4). As first-line treatments of migraine attacks, most patients (61%) stated that they used non-specific treatments and 36% that they used specific treatments, with no significant difference between patients with anxious dimension alone, anxious and depressive dimensions, and neither anxious nor depressive dimensions. However, fewer patients with both anxious and depressive dimensions used triptans, and more of them used opioids.
First-line acute treatments used by patients for a migraine attack

P < 0.05 and P < 0.01, respectively, vs. patients with neither anxious nor depressive dimensions.
P < 0.05 and P < 0.01, respectively, vs. patients with anxious dimension alone.
NSAID, non-steroidal anti-inflammatory drug.
The mean number of drug units (all pharmaceutical forms) taken for first-line treatment of an attack was significantly higher for patients with both anxious and depressive dimensions than those with anxious dimension alone or with neither anxious nor depressive dimensions (Table 4). The mean number of drug units of specific treatments taken for first-line treatment of an attack was 1.7 ± 1.1 vs. 3.9 ± 2.4 units for non-specific treatments (P < 0.01).
The total mean number of drug units taken for the treatment of an entire migraine attack was 4.7 ± 3.7 for all patients who treated the attacks, 3.9 ± 3.4 for those with neither anxious nor depressive dimensions, 4.6 ± 3.3 for those with anxious dimension alone (P < 0.01 vs. patients with neither anxious nor depressive dimensions) and 5.3 ± 4.1 for those with both anxious and depressive dimensions (P < 0.01 vs. patients with anxious dimension alone and those with neither anxious nor depressive dimensions).
Treatment effectiveness determined using the four-item SFEMC questionnaire was found good for only 24% of all patients who treated the attacks. Compared with patients with neither anxious nor depressive dimensions, treatment effectiveness was found good for significantly fewer patients with anxious dimension alone or with both anxious and depressive dimensions (Fig. 3 and Table 4). On average, patients responding ‘No’ to either question of the SFEMC questionnaire exhibited a significantly higher score on the HAD anxiety scale (Fig. 4).

Decrease in effectiveness of acute treatment of migraine attacks according to the absence or existence of anxious dimension, alone or combined with depressive dimension, as assessed by the set of four questions designed by the French Society for the Study of Migraine Headache.

Mean score on the Hospital Anxiety and Depression (HAD) anxiety scale according to the ‘Yes’ or ‘No’ response in each question of the set of four questions designed by the French Society for the Study of Migraine Headache for the determination of effectiveness of an acute treatment of migraine. Statistical significance refers to the comparison of the groups of patients giving ‘Yes’ or ‘No’ responses to each question of the set of four questions.
Discussion
The results of the SMILE study indicate that 67% of patients consulting for migraine are anxious, of whom 59% are also depressive—worthy of note, due to the rather low threshold selected for the detection of anxiety and depression on the HAD scale, the anxious and depressive dimensions detected in this study differ from generalized anxiety disorder and major depressive disorder. Furthermore, study results indicate that anxious patients, especially those with both anxious and depressive dimensions, exhibited higher levels of stress and functional impact on everyday life and used more maladaptive behaviours (avoidance, catastrophizing) than migraine patients with neither anxious nor depressive dimensions. Moreover, in patients with episodic migraine, the number of days with migraine per month, consumption and ineffectiveness of acute treatments were found enhanced in case of coexisting anxious dimension and especially if both anxious and depressive dimensions were present. In patients with episodic migraine and pronounced psychiatric profile and stress, migraine severity and functional impact were as marked as in those with chronic migraine. Stress and maladaptive coping strategies were found to be the major determinants of the anxious dimension in migraine patients, before the number of days per month with migraine headaches.
Anxiety is known to be frequent among migraine sufferers. The relationship between migraine, stress and anxiety is indeed something of a vicious circle. Migraine causes stress by the pain it generates during attacks and, interictally, by the constant fear of an impending attack. The difficulties migraine patients have in managing stress may engender exaggerated fear of attacks and maladjustment, such as catastrophizing during attacks, avoidance of any trigger factors between attacks and, in the long run, chronic anxiety, withdrawal into themselves and depression. Furthermore, anxiety increases sensitivity to stress and aggravates the perception of migraine symptoms, whereas stress is known to be a precipitating factor of migraine attacks. Finally, anticipation of attacks may promote medication overuse by migraine patients, entailing the risk of evolution to chronicity. In this complex relationship between migraine and anxiety, it is difficult to differentiate causes from effects. Detection of anxiety and stress in consulting migraine patients appears, nevertheless, crucial to successful management of migraine in clinical practice.
In the SMILE study, stress, anxious and depressive dimensions and migraine functional impact in study patients were evaluated using classical psychometric tests, some of them in an abridged form (PSS4, MSQ4) to be compatible with their use in the primary care setting. The anxious and depressive dimensions were measured using the HAD scale with a threshold of 8 for the characterization of both mood disorders, since this threshold has been shown to afford optimal balance between sensitivity and specificity (32, 33). MSQ4 was used as an estimate of migraine impact rather than frequency and severity of headaches: although one item of MSQ4 (feeling of being a burden to others) may overlap to a certain extent with affective impact, MSQ4 seemed a more comprehensive estimate of the impact of headaches. Subscales of the Brief COPE inventory (avoidance subscale) and CSQ (catastrophizing subscale) were retained as the most relevant domains for the evaluation of maladaptive adjustment in migraine patients. Catastrophizing has been perceived as a tendency to exaggerate the threat of pain and to feel hopeless about one's ability to deal with pain experience. Catastrophizing in some ways is related to depression, but does not overlap with it (34). Overall, catastrophizing can be considered as a set of negative pain-related cognitions (34) and to predict the life interference attributed to headache (35). Concerning avoidance coping strategies, they have been reported to be associated with high degrees of headache intensity (36). Several other coping strategies have been described, but, in view of the limited number of studies evaluating them, these strategies were considered less determinant for the study of migraine outcomes. Effectiveness of acute treatments of migraine was assessed using the SFEMC set of four questions that has been recommended by the French medical authorities (37).
One salient feature of the SMILE study is the increasing intensity of stress and use of maladaptive coping strategies (avoidance, catastrophizing) and quality of life impairment from migraine patients with neither anxious nor depressive dimensions to those with anxious dimension alone and ultimately to those with both anxious and depressive dimensions. The specific influence of the depressive dimension in this progression is difficult to establish, since the anxiety score also increased from the group with anxious dimension alone to that with both anxious and depressive dimensions. Occurrence of signs of depression thus might characterize only a further step in the evolution of psychiatric disorders in the natural development of the disease.
Typology analysis identified four separate groups of migraine patients: three groups with episodic migraine (Group 1, patients with both anxious and depressive dimensions; Group 2, patients with anxious dimension alone; Group 3, patients with no mood disorder) and one group with chronic migraine (Group 4). Interestingly, the group of patients with chronic migraine (those generally considered as presenting the most pronounced impact on daily life) did not differ notably from the group with both anxious and depressive dimensions (Group 1) for stress, maladaptive coping strategies, functional impact on daily life and ineffectiveness of acute treatments. This suggests that a category of patients with episodic migraine characterized by both anxious and depressive dimensions, emotional disturbances and maladaptive coping strategies (Group 1) may be at very high risk of becoming chronic migraine patients. Prospective studies confirming this hypothesis are required, all the more so since it is of utmost importance to identify the specific risk factors of transformation of episodic migraine into chronic migraine (38). Such patients should be identified in general medical practice and should be prescribed a prophylactic treatment and possibly a stress management therapy targeted at maladaptive coping strategies. Since abridged scales and questionnaires are now available that can be easily used, systematic measurement of anxiety, stress, avoidance and catastrophizing in migraine might be advisable even in general medical practice.
Among 10 putative predictive factors of anxiety, logistic regression analysis identified PSS4, avoidance and catastrophizing scores as most closely associated with anxious dimension, confirming the relevance of using a stress appraisal model (39) for understanding the emotional impact of migraine. The efficacy of relaxation and stress management therapies rests on the validity of this model. Relaxation therapies indeed demonstrated their efficacy in reducing the disability associated with migraine (40). Other identified significant factors contributed only modestly to the prediction of anxious dimension (odds ratios of 0.99–1.04). Noteworthy, severity of attacks does not feature in our list of significant predictive factors. To our knowledge, there is only limited information available in the medical literature concerning the relationship between severity of migraine attacks and psychiatric comorbidity. Similarly to us, Mitsikostas and Thomas (41) have found that anxiety and depression were not related to severity of headaches in headache out-patients, whereas there was a significant association with the frequency and duration of attacks (41). Unfortunately, these analyses combined several types of headache. Frequency of headache was not a parameter available in our study (it was not retained for the study considering that it might be affected by recollection bias), but the number of days with headache in a month emerged as a significant predictive factor, although with a modest odds ratio (1.04), notably lower than that for PSS4 score (1.64).
This study has some limitations. As regards study methodology, SMILE was an open observational study carried out among migraine patients consulting for migraine. That these patients may differ from the general population of migraine patients is reflected by the rather high reported number of days with migraine headaches per month (7.5 days/month). The physicians recruited were aware of the study objectives. Those agreeing to participate were possibly those most interested in the optimization of migraine management. However, this may not have affected the validity of the observed relationships between anxiety and migraine. Some of the psychometric tests used were abridged forms of the original tests, in order to allow their use in the general practice setting. Although not designed for the diagnosis of anxiety and depression, the HAD scale was retained for its easy and very widespread use and the existence of a validated threshold allowing the identification of patients with clinically significant anxiety or depression. The data pertaining to acute treatment of attacks were based on patients’ statements. As regards study results, a weakness of the study may be the difficulty in assessing the actual clinical significance of the differences observed between groups, some of which might be considered of rather small magnitude. On the other hand, a strength of the SMILE study is the very large number of participating physicians and patients, which reinforces the validity of the results.
The results of the SMILE study show an association between migraine and mood disorders, stress, maladaptive coping strategies and impact on everyday life in patients seeking medical attention for their headaches. This observation can in no way be interpreted as a formal demonstration of a causal relationship between migraine and anxiety and/or depression. First, since most previous work that assessed coping and catastrophizing referred to pain or headaches in general, assigning study results exclusively to a very specific condition such as migraine may be an extrapolation to be viewed with caution. Second, in interpreting study results, one must bear in mind that study patients consulted specifically for migraine and may thus represent a particular category of migraine patients having difficulties in managing their disease. Anxiety in these patients may be a concomitant disease or, for example, arise from the perceived inefficacy of acute treatment of attacks, so that it is difficult to establish firmly whether mood disorders are the cause or the result of the relative ineffectiveness of acute treatment of migraine attacks in anxious and depressive patients. A way of addressing this issue would be to determine, in a prospective study, whether or not mood disorders resolve with effective treatment of migraine headaches and whether they influence treatment efficacy. If so, this would again emphasize the importance of assessing anxiety and depression in migraine sufferers in clinical practice.
In conclusion, the SMILE study has shown that a large proportion of migraine patients consulting in primary care present with anxious and depressive dimensions. These patients experience notable degrees of stress, pronounced functional impact of migraine on their professional, family and social life and exhibit maladaptive adjustment behaviours to cope with the burden of migraine. Since stress and maladaptive adjustment behaviours appear to predict anxiety and to be positively related to the functional impact of migraine, medication overuse and poor effectiveness of acute treatments of migraine, these dimensions should be looked for carefully and taken into account for optimal management of migraine.
Acknowledgements
The authors thank Geneviève Bonnelye (TNS Healthcare) for managing the project, Séverine Ricard and Xavier Guillaume (TNS Healthcare) for carrying out the study and statistical work, and Jacques Legeai (Rédasciences-Santé) for his help in writing the article.