
Abstract
Headache symptoms account for 1-3% of admissions to an emergency department (ED). Most patients affected by a primary headache (PH) have migraine, although they are often misdiagnosed as ‘headache not otherwise specified’. We investigated the possibility of using ID-Migraine (ID-M) to improve migraine recognition in the ED setting. We planned a pilot study involving ED out-patients with a diagnosis of PH. Diagnoses of a blinded headache expert were subsequently matched with the ID-M results. We tested ID-M on 230 patients (199 PH, 31 secondary headaches). Considering only PH, ID-M exhibited a sensitivity of 0.94 and specificity of 0.83 with a positive predictive value (PPV) of 0.99. The ID-M is a simple migraine screener with high sensitivity, high specificity and high PPV, even in an ED-derived population. Methodical use of this tool in an ED setting may, once a secondary headache has been excluded, lead to rapid diagnosis of migraine.
Keywords
Introduction
Headache is one of the most common medical complaints reported by adults. It is also the fifth most common reason for visits to the emergency department (ED), accounting for 2.7% of admissions (1). The management of patients with severe/disabling headaches in the ED represents a diagnostic and therapeutic challenge for emergency department physicians (EDP) (2). The diagnosis of headache in an ED is hampered by numerous obstacles, the main one being the numerous pathologies whose primary symptom may be headache, which range from flu to devastating subarachnoid haemorrhage.
Diagnosis in the ED is usually based on multiple data: vital parameters, a brief anamnestic history (main pathologies and presence of a recent head trauma, if any), general and neurological examinations; other data are provided by blood tests, brain computed tomography scan and other examinations. Alterations in any of these examinations indicating a secondary headache leads to further tests aimed at diagnosis and treatment. If the results of the medical investigation are instead normal, particularly in patients with a previous history of headache, a generic diagnosis of headache is made, although no specific type (migraine, tension-type, cluster, etc.) is defined.
This approach, combined with the personal experience in pain therapy of the EDP, may explain the frequent use of the ‘migraine cocktail’ (association of multiple pain killers) to stop a migraine attack instead of more targeted treatment (e.g. triptans, ergots or antiemetics).
A diagnosis upon discharge of generic primary headache (PH), benign headache or headache not otherwise specified (NOS) is frequent, as shown by Morgenstern (3) and Gupta (4), and confirmed by our group (80% of headaches diagnosed as NOS in our ED) (5). This unspecific diagnosis negatively influences not only the acute treatment of migraine in the ED, but also its subsequent management in primary care, thereby perpetuating the state of underdiagnosis and increasing the burden of migraine. One explanation may be that once EDPs have excluded a secondary headache, they are unlikely to complete the diagnostic process because of the difficulty they encounter in using the International Headache Society (IHS) criteria in this setting. Indeed, we consider, as do Fiessler (6) and Gupta (4), that although the International Classification of Headache Disorders, 2nd edn (ICHD-II) criteria are more flexible than the ICHD-I, particularly following the introduction of the ‘probability’ category, they remain excessively complex and too time-consuming for EDPs.
In our experience, although migraineurs are the most frequent users of the ED (74% of primary headache) (5), they are often misdiagnosed. In an attempt to improve the accuracy of the diagnosis in the ED, we used a simple migraine screener, ID-Migraine (ID-M) by Lipton et al. (7), on out-patient ED subjects discharged with a diagnosis of PH with a view to extending the use of this screener to a more extensive trial in the ED. ID-M (7) proved to be a valid and reliable screening instrument for migraine headaches. Its easy application and its operating characteristics, which have previously been demonstrated in the primary care setting, suggest that this screener may be able to improve significantly the rate of migraine diagnosis even within the emergency care setting.
The test is based on a self-administered, simple and dichotomic questionnaire that takes into consideration the main clinical characteristics of migraine: (i) nausea or sickness to the stomach, (ii) photophobia and (iii) disability caused by pain in daily activities. The advantages of this tool, in primary care, are its high sensitivity of 0.81 [95% confidence interval (CI) 0.77, 0.85], its specificity of 0.75 (95% CI 0.64, 0.84) and its positive predictive value (PPV) of 0.93 (95% CI 89.9, 95.8) (7).
The aim of the study was to evaluate the sensitivity and specificity of this screener in a population of headache patients recently (0–48 h) discharged from the ED with a diagnosis of PH and examined in our headache centre. This procedure was agreed upon with the EDPs, before the efficacy of this instrument was assessed in a similar setting, so as not to interfere with their diagnostic procedures.
Methods
Our headache centre is a subdivision of the ED and serves as a post-acute headache clinic. The role of the headache centre is to diagnose the headache type, manage and educate patients on their headache, prescribe the best acute treatment and, if required, recommend prophylactic therapy after a monitoring period. Patients discharged from the ED with a diagnosis of PH are admitted to our centre within 48 h and examined by a neurologist specialized in headache, who makes the diagnosis, according to ICHD-II criteria, and selects the therapy on the basis of good clinical practice and national–international guidelines. Moreover, patients have a follow-up visit within 30 days so that the course of their headache can be verified.
With a view to assessing the reliability of ID-M in the ED, we planned a pilot study outside the ED, involving out-patients discharged from the ED with a diagnosis of PH, and then admitted to our headache centre.
We administered the Italian version of ID-M, previously validated by Brighina et al. (8), comprising a self-administered and dichotomic questionnaire based on three questions regarding the presence of nausea, photophobia and disability during headache. The test outcome is defined positive when the answer to at least two out of the three questions is ‘yes’.
A headache expert blinded to the test made a diagnosis, according to ICHD-II criteria, on the basis of standard anamnestic data. The data used by the ED to make a diagnosis before discharging the patients were obtained from GIPSE, a computerized database of clinical and anamnestic data used in the ED.
Patients who did not speak Italian fluently were excluded from the study owing to the obvious difficulties that would arise when translating the ID-M screener, as were subjects with an ICHD-II diagnosis of probable migraine, because the screener has not been validated to diagnose this category.
Patients with a definite diagnosis of migraine and other forms of primary and secondary headaches were included in the statistical analysis.
Patients gave their informed consent to participate in the study, which was approved by the local ethics committee.
We tested the reliability of ID-M by analysing two different groups: (i) exclusively patients with an IHS diagnosis of primary headache; (ii) the whole patient population, including primary and secondary headaches. This approach was used because ID-M had not previously been applied to a mixed population.
Data were subsequently matched, the results of the questionnaire were compared with the diagnoses of a headache expert, and the results were then statistically analysed using
Results
Between January and August 2006, a population of 245 patients, admitted to our headache centre from our hospital ED, were enrolled in the ID-M pilot study. The most frequent discharge diagnosis, made by our EDPs, was headache NOS, which accounted for 83.6% of the population. The other diagnoses were migraine in 8.4%, cluster headache (CH) in 3.5% and other forms of facial pain in 4.4% (tension-type headache, trigeminal neuralgia, etc.).
The mean age of the population was 37 years (
Patients with a definite diagnosis of migraine (i.e. excluding probable types) and other forms of primary and secondary headaches were included in the study.
When the group of primary headaches (199 patients with migraine, CH, CTTH) was analysed, ID-M displayed a sensitivity of 0.94, specificity of 0.83, PPV of 0.99 and NPV of 0.31.
When we extended the evaluation of ID-M to the population of secondary headaches, the data we obtained were similar, with a sensitivity of 0.9, specificity of 0.96, PPV of 0.99 and NPV of 0.57.
When only secondary headaches were considered, ID-M was positive in nine (29%) out of 31 patients. Five of these nine patients were affected by hypertensive headache, three by cervicogenic headache and one by Horton arteritis.
Table 1 shows the relationship between the number of positive items in the ID-M questionnaire and the type of headache.
ID-Migraine (ID-M) results and type of headache
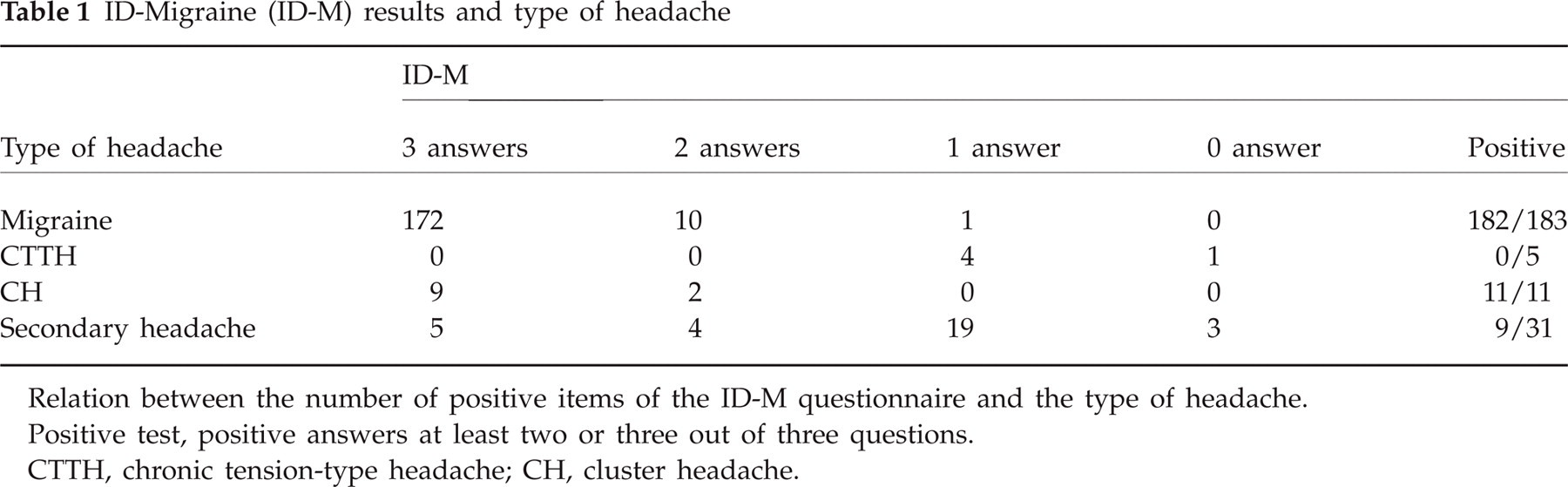
Relation between the number of positive items of the ID-M questionnaire and the type of headache.
Positive test, positive answers at least two or three out of three questions.
CTTH, chronic tension-type headache; CH, cluster headache.
Worthy of note are the false positives, which are represented by secondary headaches (9/31), and in particular by CH (11/11), with nine out of 11 patients answering ‘yes’ to all three questions.
Discussion
This study suggests that the screener designed by Lipton et al. (7) to be used in primary care may also be useful in the ED setting as a means of improving the accuracy of PH diagnosis made by EDPs, thereby passing, by asking only three questions, from an unspecific diagnosis of headache NOS to a first-level diagnosis of the headache type (migraine).
Since 30% of secondary headaches may be positive to ID-M, this screener should be used only after all possible causes of symptomatic headaches had been excluded by the EDP.
The history and physical examination are important means of distinguishing primary from secondary headaches, and above all of identifying the ‘red flags’ associated with life-threatening/dangerous causes of secondary headaches. The physical and neurological examinations, and a complete assessment of vital signs, must be performed in every patient with a headache complaint. Any ‘red flags’ associated with secondary headaches can be recalled easily with the mnemonic SNOOP (Systemic symptoms or disease, Neurological signs or symptoms, Onset sudden, Onset before age 5 or after age 50, Pattern changes from prior headaches). The strict application of these rules is likely to reduce the risk of misdiagnosis.
The results yielded by ID-M in the ED-derived population in our study are comparable to those reported in primary care (7), with a sensitivity of 0.9 regardless of whether secondary headaches were included, a specificity of 0.83, which reached 0.96 if secondary headaches were included, and a PPV of 0.99 regardless of whether secondary headaches were included. These results highlight the versatility of this screener, as shown by the similarity of the main statistical results obtained in the primary and emergency care settings.
Whereas Brighina et al. obtained a NPV value of 0.83 when they validated the Italian version of the screener (8), we obtained a NPV of 0.31 in the PH population, which increased to 0.57 when secondary headaches were included in the emergency group. This discrepancy between our results and those reported by Brighina et al. may, we believe, be ascribable to an unusually high prevalence (4.7%) of CH in our study population.
Indeed, as shown in Table 1, all patients affected by this type of headache answered ‘yes’ to at least two questions in the screener, thus resulting as false positives. This result is not unexpected if we consider that the test is based on clinical features that are typical of, although not exclusive to, migraine. In fact, it is widely known that a CH attack is described by patients as the ‘worst’ pain, which negatively influences daily activities (first item), and is associated with nausea in 40% of patients (second item), phonophobia in 12–39% and photophobia in 5–72% (third item) (9, 10). However, as ID-M has not, to our knowledge, been used to diagnose or test CH patients in previous studies (11–13), this observation warrants confirmation in future studies.
Also worthy of note is the fact that the NPV increases to 0.57 in a mixed population (primary + secondary headache types), which suggests that this test may also be used by EDPs to improve the diagnostic accuracy of secondary headaches. However, ID-M must be considered as a supporting tool within the ED setting, not as a substitute to the diagnostic procedure normally adopted by EDPs.
Indeed, the use of this tool as a final test before discharge from the ED, as proposed in our study, may minimize misdiagnosis, reducing diagnostic errors by the EDP by approximately 70%, as we observed in our population (Table 1).
In conclusion, the use of ID-M in our ED-derived population improves the diagnostic accuracy of migraine from 9% to as much as 99%, thus offering both patients and general practitioners (GP) markedly more information.
In a future scenario, the routine use of ID-M within the ED setting may, once a diagnosis of secondary headache has been excluded, offer a quick, simple, first-level diagnosis of PH, and in particular of migraine, the most common headache in the emergency setting. Indeed, the use of ID-M in the ED would reduce both the costs and the time required for a correct diagnosis, thereby improving the management of migraineurs and offering them the most effective treatment for their headache more quickly.
We should bear in mind that migraine is included in the top 20 causes of disability worldwide (World Health Report, 2001) (14), and that it is in the ED that a high number of migraine treatment-naive patients are recruited and many migraine misdiagnoses are made.
The ability to make a more accurate diagnosis of migraine in the ED would reduce the burden of both migraine (14, 15) and migraine malpractice, raise awareness among patients and GPs, and thus improve the management of this disorder.