
Abstract
The amplitude and habituation of the click-evoked vestibulo-collic reflex (VCR) was found reduced between attacks in migraineurs without complaints of ictal or interictal vertigo or dizziness, compared with healthy subjects. As a next step we recorded VCR in 17 migraine patients (eight with migraine without aura and nine with migraine with aura) who presented ictal migrainous vertigo according to the criteria defined by Neuhauser et al., using a method described previously. Migraineurs with migrainous vertigo have similar VCR abnormalities as patients without vertigo, i.e. a decreased global amplitude and absence of habituation. Potentiation seemed more pronounced in migraineurs with vertigo (7.46 ± 18.6), but the difference was not significant.
Introduction
Between attacks the most reproducible abnormality of brain function in migraine is lack of habituation to repetitive sensory stimuli (1). The latter has been demonstrated for a number of cortical evoked responses, but also for some brainstem reflexes (2). In a recent study we found that amplitude and habituation of the click-evoked vestibulo-collic reflex (VCR) was reduced in migraineurs between attacks compared with healthy subjects (3). We selected for this study patients without complaints of ictal or interictal vertigo or dizziness. As a next step, it seemed of obvious interest to perform a similar study in patients with migrainous vertigo, in order to determine if they disclosed the same, possibly more pronounced, VCR abnormalities or different changes such as delayed or absent responses that were found in basilar-type migraine (4).
Methods
We recruited 17 migraine patients (eight with migraine without aura and nine with migraine with aura) who presented ictal migrainous vertigo according to the criteria defined by Neuhauser et al. (5). Thus, the patients had to report rotational vertigo or subjective illusionary sensations of motion, and not just dizziness, which is not a vestibular symptom. The VCR was obtained and analysed using the method described previously (2, 6, 7). Briefly, while 225 clicks (0.1 ms, 3 Hz, 95 dBnHL) were delivered monaurally, the VCR was recorded with surface electromyography (EMG) over the tonically contracted ipsilateral sternocleidomastoid muscle. The responses were sequentially averaged in three blocks of 75. The VCR was recorded as a biphasic waveform with an initial positivity (p13), followed by a negativity (n23). The p13–n23 amplitude was measured on the raw and baseline EMG amplitude-corrected traces of 225 responses and in each block of 75 responses. Habituation was calculated as the percentage change of p13–n23 amplitude between the 1st and 3rd block of averagings. The results in patients with migrainous vertigo were compared with those reported in migraineurs without vertigo (see 1) using Student's t-test (Table 1). Before using the t-test, we compared the difference of variance between the two groups with an expected value (Fisher's F value; for n1 = 17, n2 = 25, F = 2.83). If the ratio between variances was > F, we used Cochrane's test for P = 0.05. For information, the VCR measures obtained in Allena et al. (3) for healthy volunteers are shown in Table 1 as historical normative data.
Vestibulo-collic reflex measures (mean ±
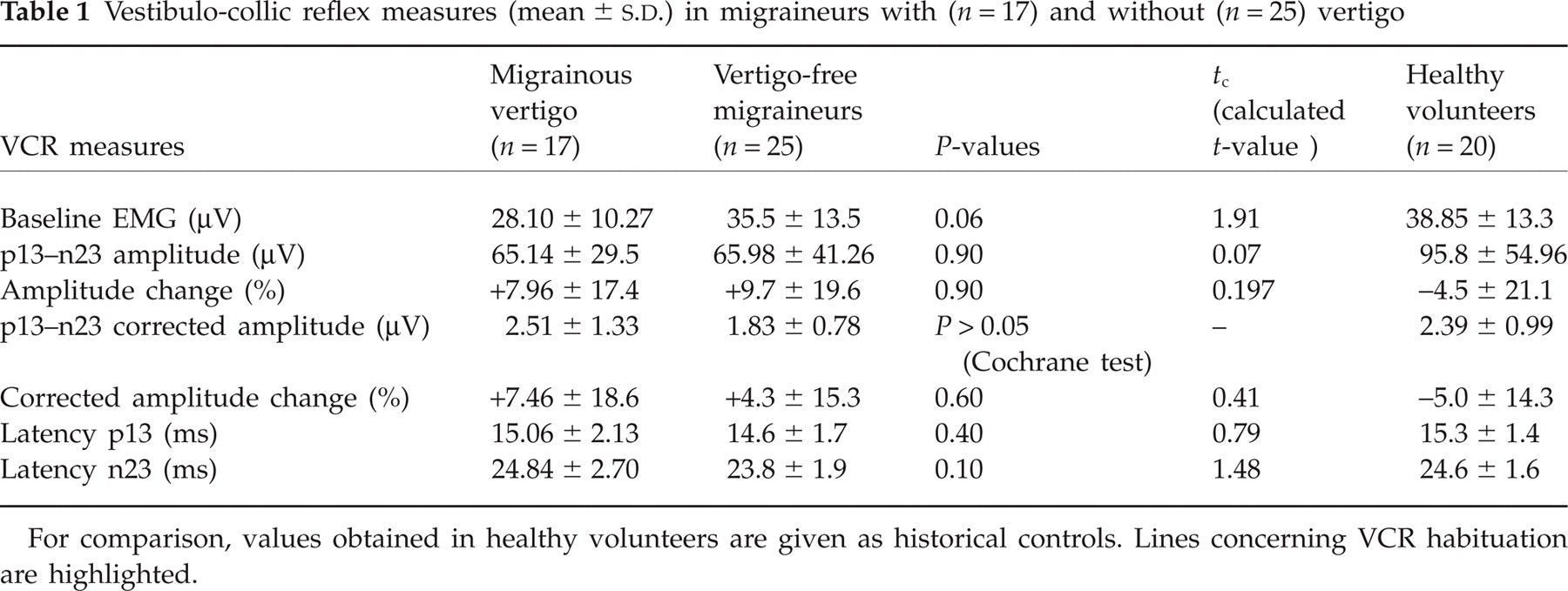
For comparison, values obtained in healthy volunteers are given as historical controls. Lines concerning VCR habituation are highlighted.
Results
There were no statistical differences in amplitude (raw and corrected), p13 and n23 latencies or VCR amplitude changes over three blocks of averagings between the groups of subjects. Like those without vertigo, patients with migrainous vertigo had on average a reduced p13–n23 amplitude and habituation both for raw and for EMG-corrected values (see Table 1), whereas p13 latency was within normal limits. As a matter of fact, habituation was replaced by an amplitude increase over the three blocks of averagings, i.e. by potentiation. On corrected VCR amplitude changes, potentiation seemed more pronounced in migraineurs with vertigo, but the difference was not significant.
Discussion
This study has shown that migraineurs with migrainous vertigo have similar VCR abnormalities to patients without vertigo, i.e. a decreased global amplitude and absence of habituation. VCR latencies are normal, contrary to the results reported in basilar-type migraine (3). These results suggest that the VCR abnormalities found in migraine are unlikely to be a marker for a clinically relevant vestibular dysfunction. They are most probably the expression in the VCR brainstem circuit of the neuronal dysexcitability also found interictally in evoked and event-related potential studies (1).
Footnotes
Acknowledgements
This study was supported by the EU Eurohead (LSHM-CT-2004-504837), by research grant 3456304F of the Belgian National Fund for Scientific Research to J.S. and by a department-to-department fellowship of the European Federation of Neurological Societies to A.R.