
Abstract
Frontal sympathetic skin responses (F-SSRs) were recorded to investigate sympathetic nervous system activity in migraine headache (MH). Thirty-five patients with unilateral MH and 10 healthy volunteers were studied by evoking bilateral F-SSRs with electrical stimulation of the median nerve in attack, post-attack and interictal periods. The mean latencies were longer and the maximum amplitudes were smaller on the symptomatic side compared with the asymptomatic side (P < 0.05 for both amplitude and latency) in attack and in interictal periods. In five patients, F-SSRs were absent bilaterally, in four patients the responses were absent only on the symptomatic side during the attack period. In the post-attack period, F-SSRs on the symptomatic side had higher amplitudes and shorter latencies compared with the asymptomatic side (P < 0.01 for both amplitude and latency). There is an asymmetric sympathetic hypofunction on the symptomatic side in attack and interictal periods, whereas there is a hyperfunction in the post-attack period.
Introduction
A wide variety of experimental data indicate that dysfunction of the sympathetic nervous system (SNS) exists in migraine sufferers. However, it has been reported that migraine is associated with a sympathetic hypofunction (1–6), sympathetic hyperfunction (7, 8), sympathetic and parasympathetic hyperfunction (9) or sympathetic instability (10, 11). To investigate sympathetic dysfunction in migraine sufferers, various procedures—sympathetic skin responses (SSRs) on palm skin, superior ophthalmic nerve stimulation by soapy or saline eye drops, pupillary functions, thermographic asymmetry, measurement of frontal blood flow, sweat estimation on frontal region, heart rate variability, etc.—were employed. Among them, SSR is an easy and non-invasive test to analyse SNS function (12, 13). Although SSRs from palm and plantar skin have been extensively researched, there are only a few studies where forehead SSRs were evoked by electrical stimulation (14–16) and none of the above-mentioned studies was on migraine headache (MH). In two successive studies performed in our laboratory, we demonstrated that SSRs from many facial sites as well as frontal location can be recorded in a relatively symmetrical fashion from palm and plantar skin alike (17); and facial SSRs can be used to evaluate autonomic nervous system (ANS) function in some diseases (18).
In this study, we recorded bilateral frontal SSRs (F-SSRs) in normal control subjects and in unilateral migraine sufferers. We tried to find the nature of SNS dysfunction on the symptomatic frontal region of unilateral migraine patients that is different from the asymptomatic side and from control subjects; and we also aimed to investigate the changes in SSRs occurring in attack, in post-attack and in interictal periods of migraine.
Materials and methods
Subjects
The sample of unilateral migraineurs consisted of 29 women and six men who met the International Headache Society (2004) criteria for migraine with aura (n = 12) or migraine without aura (n = 23) (19). They all reported that the majority of their headaches recurred on the same side. The subjects with unilateral headache recurring on either side with similar frequency were excluded. The mean age of the patients was 31.8 ± 9.3 years (range 18–52). The control group consisted of eight women and two men without a history of MH, who reported a few and short-lasting, mild headaches. The mean age of the control group was 32 ± 10.9 years (range 19–54). The patients had no other illnesses other than migraine, and the control subjects were all healthy. Informed consent was obtained from each subject and the protocol was approved by the local ethics committee.
In the patients group, 19 patients had right-sided and 16 had left-sided headache. Headache frequency ranged between one per month to six per month (mean frequency 3.3 ± 1.53 per month), and the mean of the disease duration was 7.4 ± 7 years (range 0.17–28).
All of the patients were taking analgesic and anti-emetic medication during attacks of headache and none of them was taking prophylactic treatment for MH at the time of examination. We assigned the patients into three groups: (i) patients in their attack stage (within the first day of the headache, during moderate or severe pain), (ii) post-attack stage (within 3 days following the attack) and (iii) patients in the interictal stage (> 1 week since the last headache attack). In attack recordings, subjects were asked to estimate pain intensity numerically on a 0 (no pain) to 10 (the most unbearable pain) scale. Each patient was called to check if they had developed an attack during the next day after post-attack and interictal recordings. No subject reported an attack. In post-attack recordings, none of the patients had pain. During all recordings, the side of the ongoing headache or the side of the recent headache was confirmed at each time.
The duration of illness, the side of headache, the frequency of headache, the stage of the disease at the time of examination, and pain scores during attack recordings in each patient are shown in Table 1. Fifteen patients were examined in two or three different periods. However, we could not record the responses of the same cycle of headache in each patient. In four patients attack, post-attack and interictal recordings, in another four patients, attack and interictal recordings, in six patients attack and post-attack recordings, and in one patient post-attack and interictal recordings could be done (see Table 1 for the patients who could be examined in the same cycle of headache). A total of 17 patients were in their attack period. They all had moderate or severe pain during recordings (≥ 5). The mean of the pain score was 7.1 ± 1.3 (range 5–10). Post-headache responses were recorded in 21 patients, and 16 patients were in the interictal stage while recordings were done.
The duration of illness, side of headache, frequency of headache in 1 month, stage of the disease at the time of examination, and pain scores during attack recordings

Unilateral responder.
Non-responder.
Numbers in bold indicate patients who could be examined in the same cycle of headache.
A, attack; PA, post-attack; I, interictal.
SSR recordings
SSRs were recorded between 09.00 and 17.00 h. The subjects lay in a comfortable supine position in a quiet, well-lit air-conditioned room maintained at 24 ± 1°C. The skin temperature of each subject was > 32°C. The subjects were instructed to keep their eyes open, not to breathe deeply, cough, talk or move their head during the procedure.
The experiment was performed with a Nicolet Viking IV channel electromyograph. SSR recordings were made with standard surface electrodes made from Ag-AgCl (10 mm diameter, Nihon Kohden, NM-312S). The frequency bandpass was 0.2–100 Hz. The time window for recording was 5 s and the gain was 500 μV per division.
The electrical stimulation (square pulse with 0.2 ms duration and 25 mA intensity) was applied over the right median nerve at the wrist. In subjects without any recordable response, we increased the intensity level by 10 mA (maximum 100 mA) until the responses occurred and reached a stable form. Subjects who showed no response on either side after receiving 10 consecutive electrical stimuli of an intensity of 100 mA were considered unresponsive. The stimuli were delivered at irregular intervals at least 20 s apart.
The recording location is shown in Fig. 1 (16). In each subject, the right and left sides of the frontal region were studied and bilateral F-SSRs were recorded (Fig. 2). After eliciting the first response, 10–15 stimuli were delivered to each subject. Subjects were grouped as ‘bilateral responders’, ‘unilateral responders’ and ‘non-responders’ based on the appearance of response. Bilateral responders had SSRs on both sides; unilateral responders had responses on just one side, without any recordable response on the other side; non-responders did not have any response on either side. In subjects with spontaneous responses, these responses were recorded for 20 s. In non-responders and unilateral responders, the appearance pattern of response couples was confirmed by the spontaneous responses and also by means of deep inspiration at the end of each session.

Forehead SSR: the active electrode was placed to the frontal bone and the reference was placed approximately 3–4 cm lateral to and 2 cm down from the active one. SSR, sympathetic skin responses.
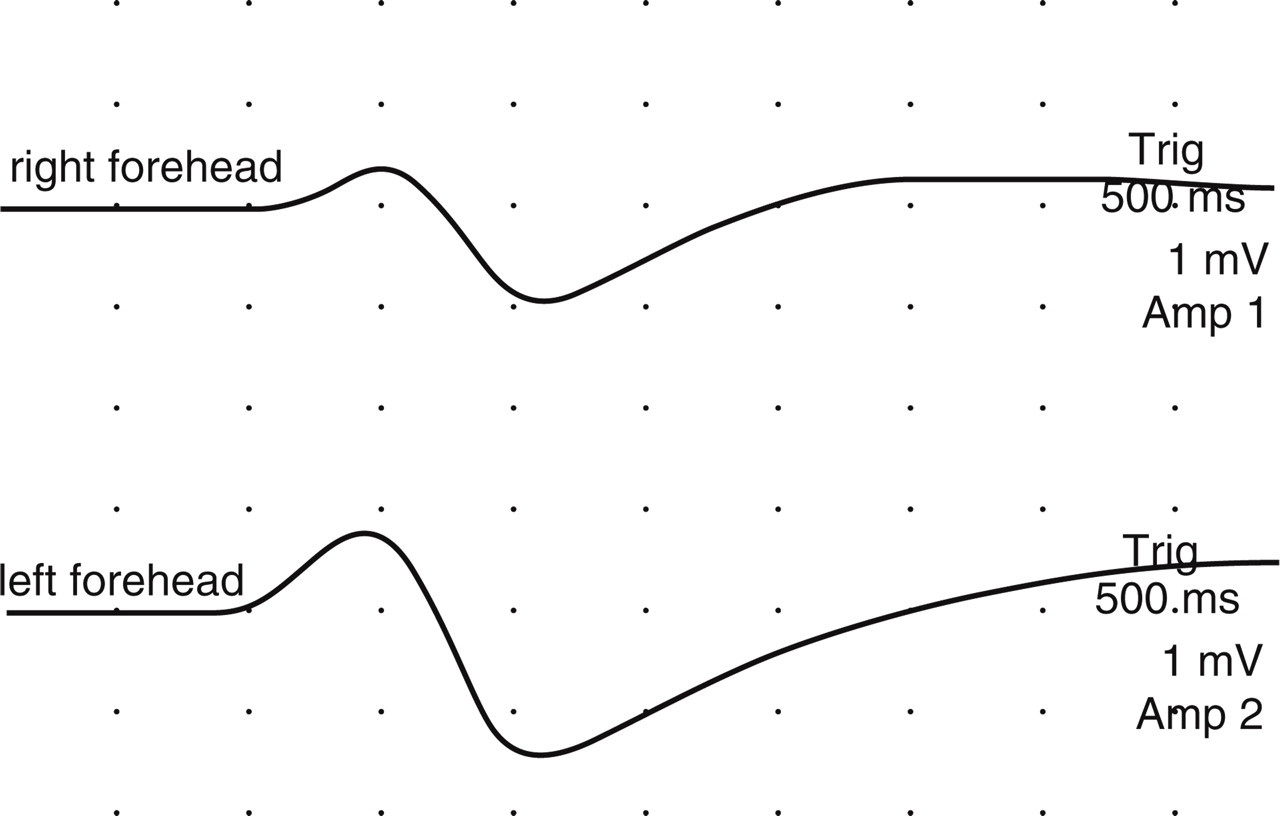
Right and left forehead sympathetic skin responses of a normal subject.
A SSR was considered to be present when its amplitude was > 50 μV and its latency was similar for at least two of the subsequent stimuli. The peak-to-peak amplitude and onset latency were measured for each response. The first 10 response pairs, recorded from right and left sides evoked by electrical stimulation, were taken into account in bilateral responder patients and in control subjects; and maximum amplitude and mean latency were calculated for each session in each subject.
We observed that the responses appeared whenever the subjects laughed or were startled by a sudden noise. However, responses were distorted slightly because of movement artefact while laughing. Such responses were excluded from the analyses.
Statistical analyses
In statistical analyses, the mean latencies and maximum amplitudes of the right and left sides evoked by electrical stimulation in control subjects, and the symptomatic and asymptomatic side responses in patient groups, were compared using a two related sample test (Wilcoxon signed ranks test). Only bilateral responder patients' data were used in comparison tests and correlation coefficients (Spearman's test) were calculated. Data from control subjects and MH patients were compared using the Mann–Whitney test.
P < 0.05 was considered to be statistically significant.
Results
In control subjects there was no significant difference between right and left sides for the mean latencies or the maximum amplitudes of F-SSRs (Wilcoxon signed ranks test, P > 0.05 for both), and we combined the data of the right and left sides. The mean latencies, the maximum amplitudes of both sides and correlations between sides are shown in Table 2.
F-SSRs of control subjects

F-SSRs, sympathetic skin responses on frontal region; R + L, combined data of right and left sides.
F-SSRs in the attack periods of unilateral migraine sufferers
Although we could not elicit a reliable response by electrical stimuli in two patients, there were small unilateral spontaneous responses on the asymptomatic side. These two patients were accepted as non-responders. We could not obtain responses bilaterally in five patients (non-responders, 5/17, 29%) and unilaterally in four patients (unilateral responders, 4/17, 24%). In all of the unilateral responder patients, the absent responses belonged to the symptomatic side.
The mean latencies, maximum amplitudes and correlation coefficients between symptomatic and asymptomatic sides in the attack period are shown in Table 3. In bilateral responder patients, the maximum amplitudes were significantly smaller and the latencies significantly longer on the symptomatic side than those on the asymptomatic side (data from eight bilateral responder patients, Wilcoxon signed ranks test, P = 0.012 and P = 0.025, respectively). The amplitudes on the symptomatic side were also significantly smaller when compared with those of control F-SSRs (Mann–Whitney test, P < 0.01), but the latencies were not significantly different (Mann–Whitney test, P = 0.055). The maximum amplitudes and the mean latencies of the F-SSRs on the asymptomatic side were not significantly different when compared with the control F-SSRs (data from 12 migraine patients, Mann–Whitney test, P > 0.05 for both amplitude and latency). However, when the data of both sides of patients with control values were compared, there was a statistically significant difference both in mean latencies (longer in patients) and in maximum amplitudes (shorter in patients) (Mann–Whitney test, P = 0.047 and P = 0.01, respectively).
Sympathetic skin responses on frontal region in unilateral migraine sufferers in attack, post-attack and in interictal periods of migraine headache

F-SSRs in the post-attack period
Among 21 patients, one patient was a non-responder in the post-attack period (1/21, 5%). The remaining 20 patients were bilateral responders. The mean latency, maximum amplitude and correlation coefficients between symptomatic and asymptomatic sides in the post-attack period are shown in Table 3.
The maximum amplitudes were significantly higher and the latencies significantly shorter on the symptomatic side compared with the asymptomatic side in the post-attack period (Wilcoxon signed ranks test, P < 0.01 for both amplitude and latency). When we compared the responses on the symptomatic side, the asymptomatic side and both sides with the control F-SSRs, neither the latencies nor the amplitudes were significantly different than those of the control values (Mann–Whitney test, P > 0.05 for latency and P = 0.052 for amplitude in symptomatic side–control data comparisons; Mann–Whitney test, P > 0.05 and P > 0.05 for asymptomatic side and both sides–control data comparisons for both latencies and amplitudes).
F-SSRs in the headache-free intervals
All of the 16 patients were bilateral responders in the headache-free intervals. The mean latency, maximum amplitude and correlation coefficients between symptomatic and asymptomatic sides in the interictal periods of patients are shown in Table 3. The maximum amplitudes were significantly smaller and the mean latencies were significantly longer on the symptomatic side compared with the asymptomatic side (Wilcoxon signed ranks test, P = 0.012 and P = 0.006, respectively). When the responses on the symptomatic side were compared with the control F-SSRs, the maximum amplitudes were significantly smaller and the mean latencies were significantly longer than those of the control F-SSRs (Mann–Whitney test, P = 0.030 and P = 0.012, respectively). F-SSRs on the asymptomatic side and also F-SSRs on both sides of patients were not significantly different either in maximum amplitude or in mean latency from those of the control values (Mann–Whitney test, P > 0.05 and P > 0.05, respectively, for both amplitudes and latencies).
Temporal changes of F-SSRs in patients who were tested repeatedly in the same cycle of headache
In attack, post-attack and interictal period recordings
One non-responder patient in both the attack and post-attack periods became a bilateral responder in the interictal stage with the smaller response on the symptomatic side. In two patients, the responses were smaller on the symptomatic side in the attack period, became higher in post-attack period, and in the interictal stage the responses were smaller on the symptomatic side than that of the asymptomatic side in one patient; and in the other patient both sides were of the same size.
In attack and post-attack recordings
One non-responder patient in the attack stage became a bilateral responder in the post-attack stage with the higher responses on the symptomatic side. Two patients who were unilateral responders in the attack period became bilateral responders in the post-attack period, with higher responses on the symptomatic side.
Two bilateral responders had smaller responses on the symptomatic side than those on the asymptomatic side during the attack period. In one of them the pattern of responses did not change in the post-attack period, whereas the other showed higher responses on the symptomatic side in the post-attack period.
In attack and interictal recordings
Two non-responder patients during the attack period became bilateral responders in the interictal stage, with the smaller responses on the symptomatic side. Two unilateral responder patients during the attack period became bilateral responders in the interictal stage, with smaller responses on the symptomatic side.
F-SSR changes related to the laterality of the pain
There were eight left- and nine right-sided migraineurs in the attack group. In the right-sided headache group, there were two non-responders (2/9) and one unilateral responder (1/9). Three non-responders (3/8) and three unilateral responders (3/8) had left-sided headaches. When we compared the data from the two groups, it was found that left-sided migraineurs had significantly smaller F-SSRs than those of the right-sided migraineurs in the attack period (non-responders and absent responses of the unilateral responders were not included in statistics; Mann–Whitney test, P < 0.01). In the post-attack period, left-sided migraineurs still had smaller responses compared with the right-sided migraineurs, but this difference did not reach statistical significance (14 right- and seven left-sided migraineurs, one non-responder's data were not included; Mann–Whitney test, P = 0.055). In the interictal period, there was no significant difference in the response size between right- and left-sided migraineurs (seven right and nine left side; Mann–Whitney test, P > 0.05).
Discussion
Major findings of the present study are consistent with a sympathetic hypofunction in attack period during moderate and severe pain; a sympathetic hyperfunction in the first 3 days following the MH; and a sympathetic hypofunction (not pronounced as in the attack period) in the headache-free period, on the symptomatic side when compared with the asymptomatic side in unilateral migraine patients. Patients with left-sided headache had significantly smaller F-SSRs than those of patients with right-sided headache in the attack period.
In the attack period, there were unilateral responder patients (4/17, 24%) with the absent responses on the symptomatic side. There were not any unilateral responders in post-attack and interictal periods of MH or of the control group. It has been suggested that asymmetry of amplitude or asynchronies of the response is a criterion for abnormality (13). The physiological or anatomical discrepancies of the peripheral factors that may have influence on SSR size (sweat gland density, skin thickness, etc.) between right and left sides are not pronounced (20, 21). Many researchers have pointed out that the amplitudes of SSRs on both sides of the body are relatively symmetrical (21–24). In bilateral responder patients in their attack period, the maximum amplitudes were smaller on the symptomatic side compared with the asymptomatic side in our study. Unilateral sympathetic dysfunction has been credited in some sources as being the cause of longer latencies and smaller amplitudes of SSRs obtained on one side compared with the responses of the normal contralateral homologous skin area (25–27). It seems reasonable to assume that there is a localized sympathetic hypofunction on the side of the headache in unilateral migraine patients in the attack period according to the findings of the current study and the conclusions of the above-mentioned studies. Drummond (28) has shown that pupil diameter was smaller on the side of headache during headache, and in another study (3) he showed that both during and between episodes of headache, the pupil on the symptomatic side dilated more slowly and less extensively than the opposite pupil in unilateral migraine patients. He has suggested that there is a unilateral sympathetic hypofunction during attacks of migraine, compatible with our findings in the attack period.
In our study, five patients were non-responders (29%) during attack. There was no non-responder subject in the interictal stage and in the control group, whereas there was one non-responder subject in the post-attack period. Chen et al. (16) recorded frontal SSRs in patients with facial hyperhidrosis both before and after T-2, 3 sympathectomy. He reported that frontal SSR was present in every normal control subject by electrical stimulation, although 20% patients had absent SSR before sympathectomy, and 72% patients with absent SSR in the frontal region after surgery. On the other hand, the absence of responses bilaterally might be explained by the results of the studies in which it was reported that migraine is associated with sympathetic deficit in facial blood vessels and the pupillary apparatus, primarily on the symptomatic side in patients with unilateral headache, but also contralaterally in some cases (3, 29, 30). It was not an expected finding for us to see a non-responder patient in the post-attack period, since sympathetic hyperfunction was observed in the post-attack period in our patients. This non-responder patient in the post-attack period may reflect the individual differences in shifting from headache to recovery phase. Further studies are needed to explain this finding.
We observed the hypo–hyper–hypofunction cycle of F-SSRs on the symptomatic side compared with the asymptomatic side in the majority of patients who were sequentially studied in the same attack. Two out of four unilateral responder patients with the absent responses on the symptomatic side in the attack period became bilateral responders in the post-attack period, with the higher responses on the symptomatic side. Also in two patients who were studied in all three stages of the same attack, we could record responses with the smaller amplitudes in the attack, the higher amplitudes in the post-attack, and the smaller amplitudes in one patient and the same size of amplitude in the other patient in the interval period on the symptomatic compared to the asymptomatic side. These findings especially support the results of this study in which sympathetic hyperfunction on the symptomatic region was found in the post-attack period, and reflect the dynamic nature of the SNS. Furthermore, this observation shows the necessity of temporal recording in each subject to capture the nature of function of the SNS occurring in unilateral MH. These temporal changes in unilateral MH occurring after the attack period may explain the discrepant findings of the previous studies, in which hypofuntion of SNS in some and hyperfunction in others were found. Finally, the role of the observed hyperfunction of SNS on the symptomatic side in the recovery period of headache could be either a trigger of recovery or a result of a rebound phenomenon of the former SNS hypoactivity, which should be clarified by investigating F-SSRs and trigeminovascular responses together.
After leaving the superior cervical ganglion, the postganglionic sympathetic fibres that run along the internal carotid artery innervate the medial portion of the forehead and eye, and the fibres along the external carotid artery innervate the lateral portion of the forehead (31). The recording location on the forehead region in this study may represent the lateral territory and may provide further information about the lateral subdivision of the forehead's sympathetic innervation. Although we did not investigate the pupillary function in our patients, there is a huge body of research in which pupillary function has been found to be affected in MH (1–6, 28, 29, 32). In the majority of studies, sympathetic hypofunction was determined in MH. Drummond (3) has suggested that this sympathetic deficit could be due to the compression of the sympathetic plexus surrounding the internal carotid artery in the carotid canal, and he has supported this suggestion by the finding of symmetrical sweating and flushing in the cheeks of unilateral migraine sufferers, since cheeks are innervated by the sympathetic fibres that follow the external carotid artery and bypass the carotid canal (29). However, F-SSRs in our study demonstrated that not only the fibres that follow the internal carotid artery but also those following the external carotid artery may be involved similarly in unilateral MH. The findings of previous studies and our own together may indicate that the abnormality in MH was not distal to the bifurcation of carotid artery.
Our aim in setting at least a week to assign the patients in the interictal period following an attack was to avoid the interface of the post-attack and interval stages. Mylius et al. (5) compared the changes in local and systemic autonomic function within 1 week of a migraine attack. They found reduced velocity of pupillary constriction and smaller amplitude of constriction in migraine patients within 2 days of an attack, and assumed that these were signs of parasympathetic dysfunction. A possible reason for the observed parasympathetic hypofunction demonstrated within 2 days following an attack in the mentioned study could be sympathetic hyperfunction, which is consistent with our findings. The sympathetic and the parasympathetic subdivisions of the ANS generally work in an opposite manner, but the relation between these two subdivisions of the ANS in the frontal region could be tested by evoking trigemino-parasympathetic reflex, e.g. by soapy eye drops and examining the changes in F-SSRs at the same time to make better assumptions in further studies.
In the attack period, we found that left-sided migraineurs had significantly smaller F-SSRs than right-sided migraineurs. Although we could not support our findings statistically, it seems that in the post-attack period left-sided migraineurs still had smaller F-SSRs than right-sided migraineurs. Gruzelier et al. (33) have reported that left-sided pain is associated with under-responsiveness and fast habituation, right-sided pain with over-responsiveness and slow habituation in autonomic responsiveness to sensory stimuli in unilateral migraine sufferers. Avnon et al. (34) have measured the trigemino-parasympathetic reflex in unilateral migraine patients by the vasodilator response of forehead skin bilaterally, and reported that left-sided migraineurs have higher bilateral parasympathetic vasodilation and more pronounced bradycardia than right-sided migraineurs in headache-free intervals. They mentioned that the autonomic control of brain is asymmetrical, the left hemisphere affecting predominantly parasympathetic function and the right hemisphere affecting predominantly sympathetic function. These data lead us to conclude that patients with right- and left-sided headache should be studied separately in future research.
In two patients in the attack period, although we could not elicit a recordable response on either side by high levels of electrical stimuli, a few small responses appeared spontaneously or by laughing on the asymptomatic side. A possible explanation for this observation could be resistance to electrical stimulation in the attack period. To draw a better conclusion about resistance to electrical stimulation occurring in SNS during headache, this finding should be supported by testing the differences in the thresholds of electrically evoked responses in migraine patients and normal subjects.
The limitations of this study could easily be overcome by increasing the number of patients. Moreover, some of the issues arising from this study need clarification in future research. First, in patients who were studied in two or three different stages, we could not record the responses of the same cycle of attack, e.g. the patient was tested in the post-attack period of a headache, then in the attack period of another headache. This situation did not allow monitoring the changes occurring in F-SSRs in one cycle of headache composed of ‘attack, post-attack and headache-free’ periods. Second, although we assigned the patients into three groups strictly according to the time points in relation to the attack, this staging seems to be inadequate in individual patients. The beginning and the duration of recovery seem to be different in each patient. Moreover, although the results of this study have demonstrated that in the attack period, during moderate or severe pain, there is a hypofunction in the SNS on the frontal region, it was not possible to determine whether this hypofunction existed since the beginning of the attack or in the termination period of the attack. Regarding the highly dynamic nature of the SNS, its behaviour could not be clarified until the temporal recordings, e.g. recording hourly, were done all during the attack stage. Third, the involved side showed a statistically significant hypofunction over that of the asymptomatic side during attack and interictal stages of MH, and hyperfunction in the post-attack stage, but there were a few exceptional patients who showed the opposite.
Although we need a larger sample of unilateral migraine patients and control subjects for a better conclusion related to F-SSRs in MH, this technique has some advantages compared with others that have been used in evaluating sympathetic nervous function in migraine patients. Continuous recording may be done during all stages of MH. This proposed technique is easy to apply, quick, non-invasive and may have the potential to investigate and monitor the temporal changes in SNS activity in migraine patients.