
Abstract
Subjects with migraine with aura (MA) have a high prevalence of white matter lesions (WMLs) on magnetic resonance imaging (MRI). Moreover, right-to-left shunt (RILES), mainly due to patent foramen ovale, is frequently associated with MA. The aim of this study was to clarify the relationship between RILES and WML in MA. We enrolled 87 consecutive subjects affected by MA. Patients were screened for migraine characteristics and cerebrovascular risk factors. Transcranial Doppler was used to diagnose RILES and MRI with T2-weighted and diffusion-weighted imaging (DWI) to evaluate presence, number and volume of WMLs. RILES was present in 45% of patients. We did not detect any DWI hyperintense lesion; WMLs were present in 61% of patients on T2-weighted images. Presence of WMLs did not correlate with any migraine clinical feature, whereas the presence, number and volume of WMLs increased with subjects' age. There was no significant difference in the total volume and number of WMLs in the group with and without RILES. In conclusion, RILES does not increase the likelihood of finding WMLs in migraineurs.
Keywords
Introduction
The occurrence of white matter lesions (WMLs) on magnetic resonance image (MRI) in migraineurs, in particular if with aura, is well described (1–3). There is still debate on the possible mechanism of formation of WMLs in migraine (4). Subjects with migraine with aura (MA) have a twofold risk of being a carrier of a cardiac right-to-left shunt (RILES) due to patent foramen ovale compared with the general population (5–7). Patent foramen ovale, which can be detected by transcranial Doppler (TCD), is a risk factor for cryptogenic ischaemic stroke in young patients (8, 9), and its prevalence in patients with MA is about 45% (5–7). RILES in migraineurs might be the expression of a common genetically inherited trait (10, 11) or causally correlated with migraine attacks. A reduction in number and burden of migraine attacks after transcatheter closure of RILES has been described in non-controlled, retrospective (12–16) or, although prospective, non-randomized studies (17, 18).
In order to shed light on the existence of a possible aetiological connection between RILES and WMLs in migraineurs, we evaluated by brain MRI the number and total volume of WMLs in migraineurs with aura with and without RILES. Moreover, we used diffusion-weighted imaging (DWI) to detect the presence of hyperintense lesions suggestive of acute ischaemia in our patients.
Methods
We prospectively enrolled in our Institutional Review Board-approved study 87 consecutive patients admitted to the Headache Centre of our Department with a clinical diagnosis of MA.
All subjects, after informed consent, underwent complete clinical work-up, including a questionnaire based on International Headache Society (IHS) criteria (19), neurological examination, evaluation of known risk factors for cerebrovascular disease, screening for thrombophylic acquired or inherited conditions, supraortic Duplex, TCD with gaseous contrast and MRI.
Criteria for diagnosis of migraine with aura
We followed the established criteria of the IHS for the diagnosis of MA (19); moreover, only subjects with at least two episodes of aura lifelong and with normal neurological examination were considered. Subjects with previous focal cerebrovascular episodes and with carotid stenosis > 50% were excluded.
The following migraine clinical variables were considered: age of onset, duration of disease in years, duration of aura in minutes, number of attacks with and without aura per year.
Risk factors for cerebrovascular disease
We considered smoking, family history of cerebrovascular disease, hypertension, hypercholesterolaemia or diabetes, body mass index (BMI), use of oral contraceptives.
Thrombophylic screening
The following thrombophylic markers were evaluated: fasting plasma levels of protein C, protein S, levels of homocysteine, presence of activated protein C resistance, presence of antiphospholipid antibodies and lupus anticoagulant; genetic tests for factor V Leiden, C677T methylene tetrahydrofolatereductase (MTHFR) gene mutations and the prothrombin G20210 mutation were obtained in all subjects.
Supra-aortic duplex and transcranial Doppler examination
All subjects underwent full colour duplex examination of neck arteries (Esaote AU 5, Genova, Italy) and TCD of main intracranial trunks (Multidop X 4 DWL, Sipplingen, Germany). All 87 subjects considered had sufficient temporal bone window and were able to perform the Valsalva manoeuvre, as tested by means of TCD [reduction of ≥ 30% of mean flow velocity of middle cerebral artery (MCA) during Valsalva]. Mean flow velocity was recorded on right MCA. A small sample volume of 8 mm in length and a low gain provided the optimal setting for the background spectrum (20); the depth of recording was 45–55 mm. The test was performed with the patient in the lying position, at rest and after Valsalva manoeuvre, with injection of a mixture of 9 ml of saline and 1 ml of air, according to standard methods (21, 22). Valsalva manoeuvre started 5 s after the beginning of the injection of contrast medium, and lasted 10 s. The presence and number of microbubbles (Mb) were recorded. All examinations were performed by a single experienced operator, who listened to each of the software-recorded signals, watched each signal on the screen and evaluated the signals off-line. Gaseous microemboli had typical visible and audible short-duration high-intensity signals within the Doppler spectrum. The number of Mb was evaluated on-line and off-line by the same operator. Intraobserver reliability was high (κ= 0.94). RILES was considered small when the number of Mb was < 10 and medium to large when Mb were ≥ 10.
MRI
MRI was performed with a 1.5-T scanner (Signa Excite; General Electric Medical Systems, Milwaukee, WI, USA). MR examinations included the following pulse sequences: fluid-attenuated inversion recovery (FLAIR) (inversion time 2200 ms, repetition time 9002 ms, echo time 91.42 ms), fast spin echo (FSE) T2 (repetition time 5840 ms, echo time 97.92 ms) and DWI (repetition time 10 000 ms, echo time 84.90 ms, b 1000 s/mm2). All the series covered the whole brain and were acquired with 3 mm thickness without gap between slices, with a field of view of 24 × 24 cm, 256 × 256 image matrix. Apparent diffusion coefficient (ADC) maps were calculated off-line on a dedicated workstation (Advantage Windows 4.1; GE Medical Systems).
Images were examined by two neuroradiologists, blinded both to clinical data and to the presence of RILES. WMLs were identified separately and, in the case of disagreement about the absence or occurrence of lesions, decision was made by consensus. Lesions had to be hyperintense both on FSE T2-weighted and FLAIR imaging; when signal alteration was present on two or more contiguous slices it was counted as one single lesion. Virchow-Robin spaces were identified on the basis of signal characteristic, shape and location (23). Diffusion-weighted images were inspected to detect the presence of hyperintense lesions. Topographical maps were used to locate lesions in the anterior circulation or posterior circulation territories of blood supply to the brain (24, 25). Lesions were then accurately outlined utilizing a semiautomated segmentation tool (Analyse 6.0 BIR; Mayo Clinic, Rochester, MN, USA); number of lesions and lesion load (i.e. the total volume of lesions identified on MRI) were calculated for each patient.
Statistical analysis
Fisher's exact test was used to compare the presence of WMLs on T2-weighted MRI in subjects with and without RILES and the Mann–Whitney U-test to compare the number of WMLs and lesion load in migraine subjects with and without RILES.
To assess differences in lesion load and number of WMLs in patients without RILES, with small RILES and with medium to large RILES, the Kruskal–Wallis
We also divided migraine patients according to the presence or absence of WMLs, and univariate analyses (χ2, Fisher's exact and Mann–Whitney U-tests) were performed to assess differences in vascular risk factors and migraine features in these two groups.
Correlations between the number of WMLs and patient's age, migraine features (disease duration, number of migraine attacks with aura per year, number of migraine attacks without aura per year, duration of aura), BMI, number of Mb detected by TCD were done with the Spearman rank order test. We proceeded analogously to calculate correlations with lesion load.
Values of P < 0.05 were considered to be significant.
Results
Eighty patients met criteria for analysis: seven subjects were excluded because of previous cerebrovascular episodes (n = 2), unwillingness to perform MRI or TCD (n = 3), history of major cardiac surgery for congenital heart disease (n = 1) and severe artefacts on MRI due to dental hardware (n = 1). Mean age of patients was 37.24 ± 11.48 years, mean disease duration was 16.14 ± 11.94 years, mean number of attacks without aura per year was 43.03 ± 70.80 and the mean number of attacks with aura per year was 28.19 ± 55.11. The mean duration of aura was 34.30 ± 32.56 min.
Thirty-six of 80 (45%) subjects had RILES, with 19 (23%) bearing a medium to large one. There was no significant difference in age in migraine patients without RILES vs. those with RILES (39.52 ± 12.13 vs. 34.44 ± 10.10 years; P = 0.10).
MRI study showed the presence of WMLs on T2-weighted MRI in 49 subjects (61%), of whom 42 (52%) had lesions only in the anterior circulation, three (3.7%) only in the posterior circulation and four (5%) in both. We did not detect any hyperintense lesion on DWI in subjects with or without RILES.
Contingency table analysis detected a similar percentage of WML presence in migraineurs with and without RILES: 61.1% of subjects with RILES (22 out of 36) and 61.4% of subjects without RILES (27 out of 44) had WMLs on T2-weighted MRI.
The number of lesions and lesion load on T2-weighted MRI in patients with and without RILES were not significantly different (Table 1).
Presence of WMLs as detected by T2-weighted MRI and MRI-derived metrics in migraine patients without RILES and with RILES
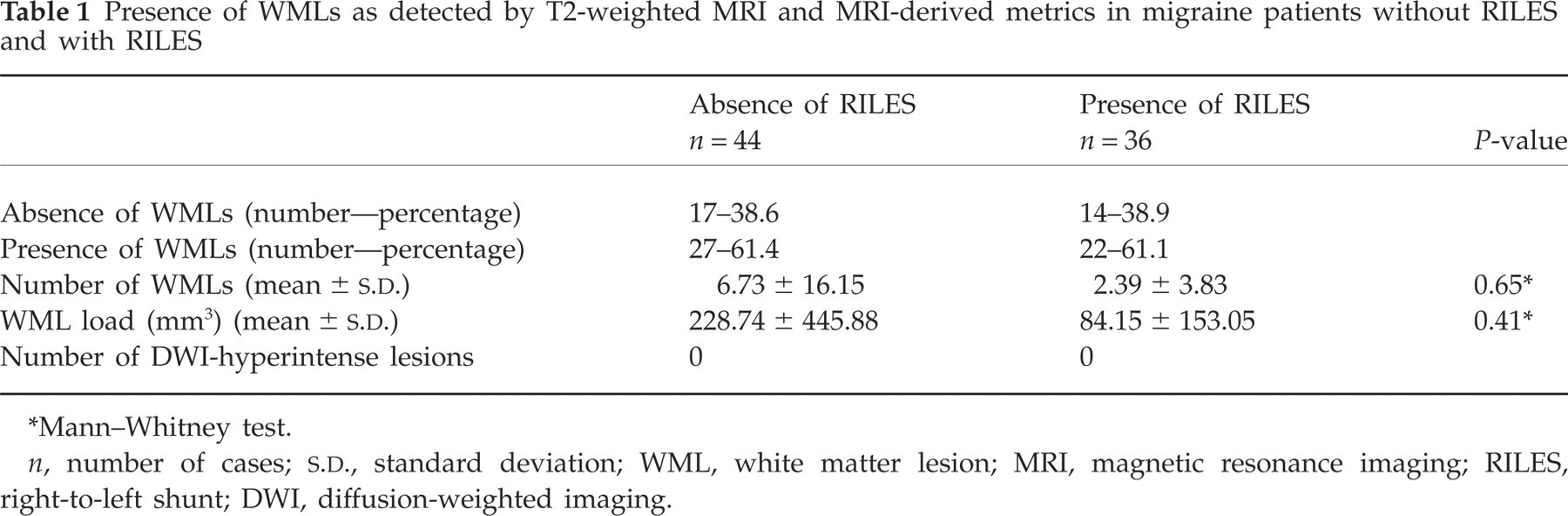
Mann–Whitney test.
n, number of cases;
Migraine patients with and without RILES did not differ significantly in WML load or WML number, both when considering two groups (patients without and with RILES) and when considering three groups (patients without RILES, with small RILES and with medium to large RILES) (Fig. 1).

White matter lesion load (A) and number of white matter lesions (B) detected on T2-weighted magnetic resonance imaging for migraine patients without right-to-left shunt (RILES) or with the presence of RILES (any size, small or medium to large). Volume and number of lesions are reported according to their vascular territory location. Error bars indicate standard deviation.
There was also no significant correlation between the number of Mb detected by TCD both at rest and after Valsalva manoeuvre and lesion load or number of WMLs (Spearman rank order test, P > 0.05).
When migraine patients were divided according to the presence or absence of WMLs and differences in vascular risk factors were assessed in these two groups, it was found that migraine patients with WMLs were significantly older (39.93 ± 12.91 vs. 32.52 ± 7.74 years; P = 0.035) (Table 2). However, the lack of statistically significant difference in some comparisons could be due to the small sample size for specific risk factors.
Vascular risk factors in migraine patients with T2-weighted MRI positive for the presence of WMLs vs. patients without MRI-detected lesions

Fisher exact two-tailed test.
Mann–Whitney test.
n, number of cases; MRI, magnetic resonance imaging; WML, white matter lesion; TIA, transient ischaemic attack.
Moreover, the number of lesions and lesion load on T2-weighted MRI significantly correlated with patient's age (Spearman rank order test, r = 0.25, P < 0.05). There was no significant difference in migraine features between these two groups (Table 3).
Migraine features in patients with T2-weighted MRI positive for the presence of WMLs vs. patients without MRI-detected lesions
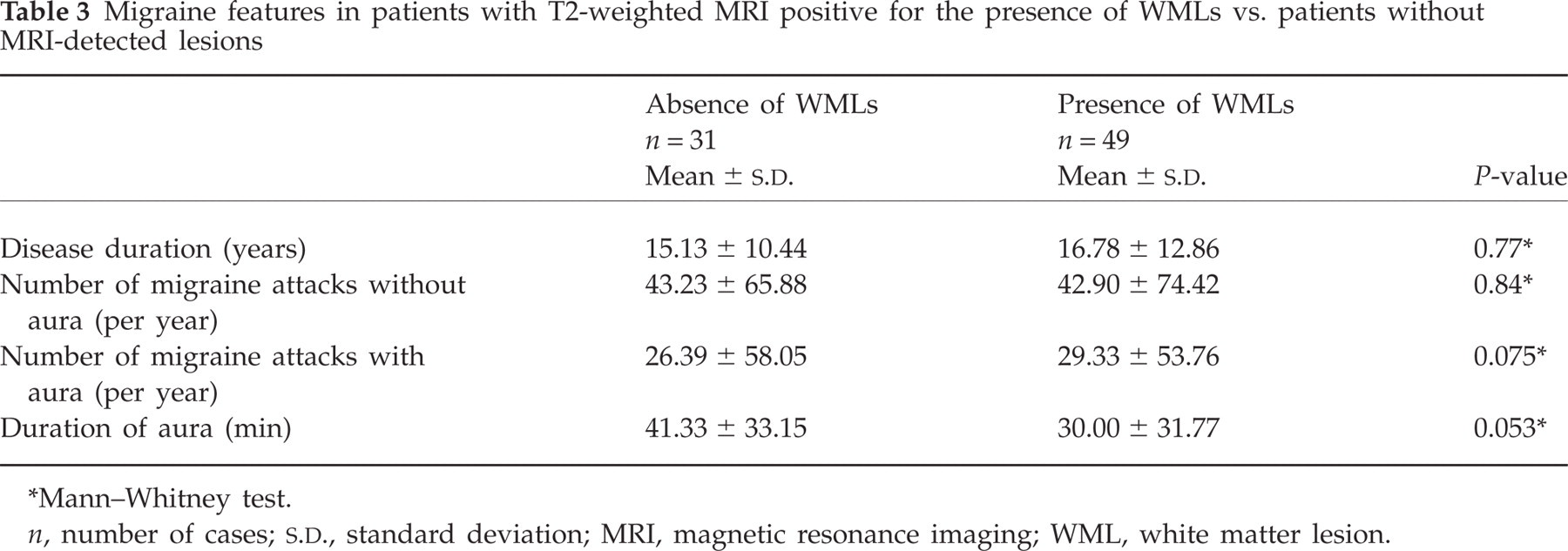
Mann–Whitney test.
n, number of cases;
Discussion
Patients with migraine have a relatively high prevalence of subclinical WMLs on T2-weighted brain MRI (1, 2). Fazekas and coworkers have reported a prevalence of WMLs in MA of 53% (1), and Kruit et al. have described a frequency of deep WMLs of 35% in MA (2). The mechanisms by which migraine conveys an increased risk of subclinical WMLs is not completely understood. The findings that the prevalence of RILES is the same in patients with MA as in patients with cryptogenic stroke, and that RILES is significantly associated with migraine in cryptogenic stroke, have led us to hypothesize that subclinical WMLs might also be associated with the presence of RILES in migraineurs.
Since speculation suggests that multiple WMLs detected by MRI in migraineurs might be the footprints of paradoxical microembolic events in the brain, we aimed to assess if migraineurs with aura and RILES had a more severe involvement of white matter on brain MRI than migraineurs with aura and without RILES.
We studied 80 subjects with a standardized diagnosis of MA following IHS criteria (19).
Patent foramen ovale detected by TCD was present in 45% of migraineurs. Our data confirm the high prevalence of RILES in migraine subjects as reported in the literature (5–7). We did not detect any hyperintense signal suggestive of acute ischaemic lesion on DWI in migraine subjects with or without RILES. Similar results on the absence of DWI hyperintense lesions in migraine patients have been reported (26).
DWI has a very high sensitivity for acute ischaemic changes in brain tissue (27, 28), where lesions can be identified as DWI hyperintense and hypointense on ADC maps due to the reduction of diffusion values which accompanies cytotoxic oedema in the acute phase of ischaemia. Jauss and coworkers have recently reported a high prevalence of posterior circulation DWI lesions in stroke patients with RILES, yet they did not report the presence of migraine (29). In our study, migraineurs with RILES had a higher number of T2-weighted WMLs in posterior circulation compared with non-RILES migraineurs, but the difference was not significant.
Using MR images with 3 mm thick slices without gap, read by two neuroradiologists blinded to the clinical characteristics of the patients, we found WMLs on T2-weighted images in 49 out of 80 subjects affected by MA (61%).
Fazekas et al. (1) have reported that in 38 migraineurs the prevalence of MRI lesions depended on the type of headache (18% in migraine without aura, 53% in migraine with typical aura, 38% in basilar migraine); we studied a homogeneous cohort of migraineurs with aura and found a percentage of patients with MRI lesions slightly higher than the corresponding subgroup of patients with migraine with typical aura.
A Dutch population-based study investigated by MRI subclinical infarctions and WMLs in migraine patients and controls. It reported that migraineurs had more subclinical infarcts located in the posterior circulation territory and that the risk of posterior circulation infarcts increased with increasing attack frequency. In addition, in their analysis only women with migraine, with and without aura, suffered from WMLs at a greater extent than controls, and traditional cardiovascular risk factors did not modify this effect on deep WMLs (2). The relatively high prevalence of WMLs in our population compared with the literature could be due to the high prevalence of hypertension (15 out of 80, 19%) and to the relatively high mean age of 37.24 ± 11.48 years.
Our data do not confirm the relationship between WMLs and attack frequency, considering attacks both with and without aura: indeed, the presence of WMLs was not dependent on migraine clinical features, but was associated with older age. It is possible that WMLs in migraineurs might thus be only the expression of age-related gliosis.
The analysis of presence, number of WMLs and lesion load in our migraine patients without RILES, with small RILES and with medium to large RILES did not show any difference between groups. Moreover, there was no correlation between the number of Mb detected by TCD and lesion load or number of WMLs, indicating that the presence of RILES, even of large size, is not associated with the degree of subclinical white matter involvement detected by MRI in migraineurs.
Further studies are needed to investigate if the concomitant presence of additional cardiac abnormalities such as atrial septum aneurysm is associated with the presence of WMLs in migraine patients with RILES (30). Our study does not accord with speculation suggesting a causal relationship between RILES and WMLs in migraine, whereby microemboli travelling through the RILES cause subclinical brain tissue ischaemia. The question regarding which of the numerous factors underlying the pathophysiology of MA might also support the formation of subclinical WMLs is still open. Other mechanisms, including reduced blood perfusion during migraine attacks (31, 32), increased platelet activation and platelet–leucocyte aggregation (33), vasoconstriction, possibly mediated by endothelium perturbation (34, 35) or neurogenic inflammation, might lead to white matter damage (36).
So far, there is no evidence supporting the indication to perform transcatheter closure of RILES in migraineurs. The results of ongoing randomized controlled trials will shed light on this issue.
In our study the number and volume of WMLs in migraineurs with aura were not associated with the presence of RILES, suggesting that in migraine patients with RILES, without a history of stroke, detection of these lesions by MRI is not necessarily associated with cardioembolic events. Thus, our data suggest avoiding the use of multiple WMLs as an MRI marker useful for decision-making when planning primary stroke prevention in subjects with migraine and RILES.