
Abstract
A 33-year-old woman presented with a 3-week history of left periorbital pain. There was continuous background pain with intermittent severe exacerbations occurring three to four times a day, each time lasting for an hour accompanied by lacrimation but no rhinorrhoea, conjunctival injection or ptosis. There was early morning awakening. She gave a history of a similar event 1 year previously lasting 1 week. On examination there were no neurological signs.
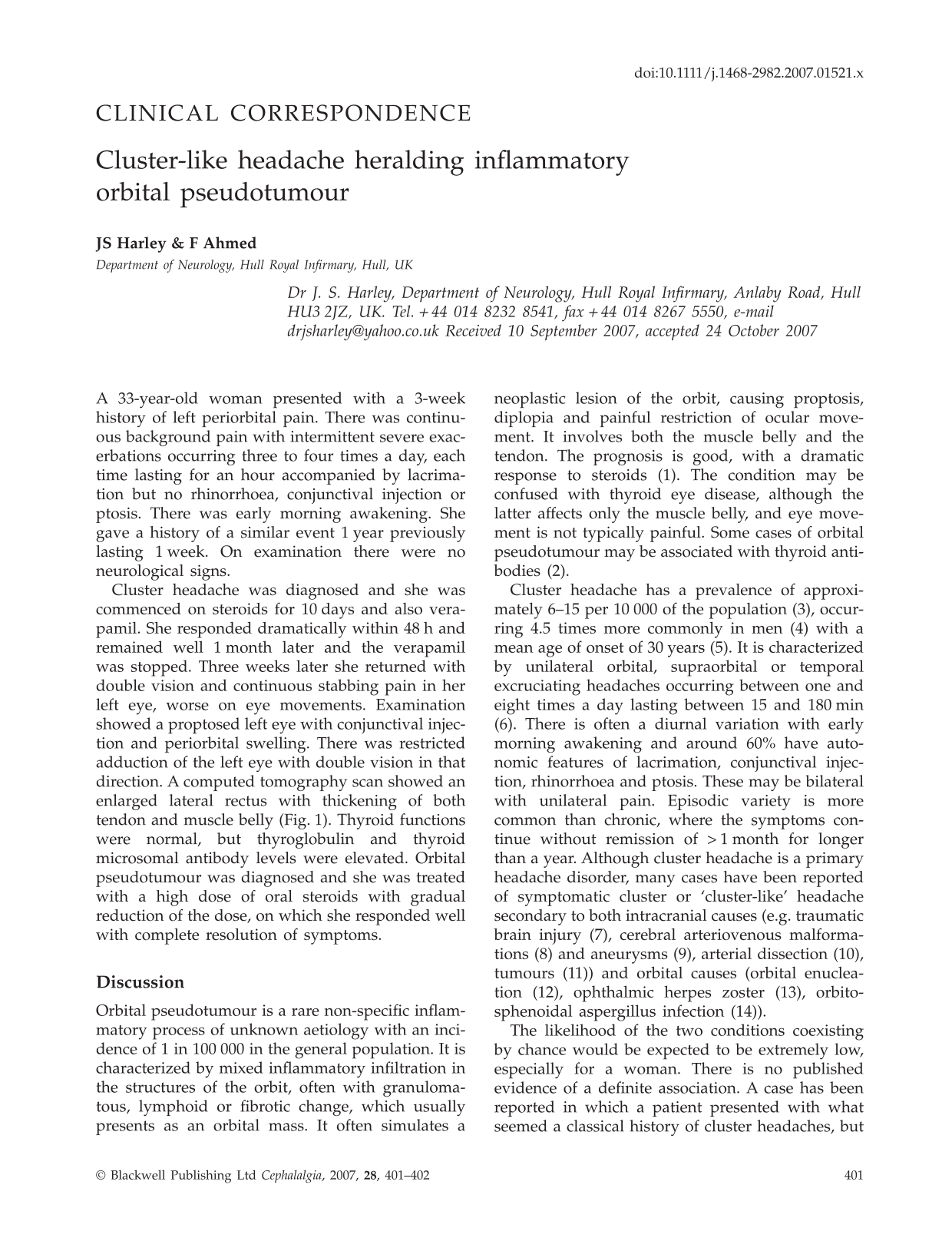
Cluster headache was diagnosed and she was commenced on steroids for 10 days and also verapamil. She responded dramatically within 48 h and remained well 1 month later and the verapamil was stopped. Three weeks later she returned with double vision and continuous stabbing pain in her left eye, worse on eye movements. Examination showed a proptosed left eye with conjunctival injection and periorbital swelling. There was restricted adduction of the left eye with double vision in that direction. A computed tomography scan showed an enlarged lateral rectus with thickening of both tendon and muscle belly (Fig. 1). Thyroid functions were normal, but thyroglobulin and thyroid microsomal antibody levels were elevated. Orbital pseudotumour was diagnosed and she was treated with a high dose of oral steroids with gradual reduction of the dose, on which she responded well with complete resolution of symptoms.

CT scan showing enlarged lateral rectus muscle and tendon.
Discussion
Orbital pseudotumour is a rare non-specific inflammatory process of unknown aetiology with an incidence of 1 in 100 000 in the general population. It is characterized by mixed inflammatory infiltration in the structures of the orbit, often with granulomatous, lymphoid or fibrotic change, which usually presents as an orbital mass. It often simulates a neoplastic lesion of the orbit, causing proptosis, diplopia and painful restriction of ocular movement. It involves both the muscle belly and the tendon. The prognosis is good, with a dramatic response to steroids (1). The condition may be confused with thyroid eye disease, although the latter affects only the muscle belly, and eye movement is not typically painful. Some cases of orbital pseudotumour may be associated with thyroid antibodies (2).
Cluster headache has a prevalence of approximately 6–15 per 10 000 of the population (3), occurring 4.5 times more commonly in men (4) with a mean age of onset of 30 years (5). It is characterized by unilateral orbital, supraorbital or temporal excruciating headaches occurring between one and eight times a day lasting between 15 and 180 min (6). There is often a diurnal variation with early morning awakening and around 60% have autonomic features of lacrimation, conjunctival injection, rhinorrhoea and ptosis. These may be bilateral with unilateral pain. Episodic variety is more common than chronic, where the symptoms continue without remission of > 1 month for longer than a year. Although cluster headache is a primary headache disorder, many cases have been reported of symptomatic cluster or ‘cluster-like’ headache secondary to both intracranial causes (e.g. traumatic brain injury (7), cerebral arteriovenous malformations (8) and aneurysms (9), arterial dissection (10), tumours (11)) and orbital causes (orbital enucleation (12), ophthalmic herpes zoster (13), orbito-sphenoidal aspergillus infection (14)).
The likelihood of the two conditions coexisting by chance would be expected to be extremely low, especially for a woman. There is no published evidence of a definite association. A case has been reported in which a patient presented with what seemed a classical history of cluster headaches, but with features of ocular pathology at the same time (proptosis and pain on eye movements). Imaging confirmed enlarged extraocular muscles (15). A second case has been reported where the patient presented with cluster headache that had features of orbital pseudotumour, once again, at the same time (16).
In this case, there had been a history of similar headaches 1 year previously, lasting for 1 week. At this presentation, the presence of the continuous background pain hints towards a symptomatic aetiology. It is likely that the cluster-like symptoms were directly as a result of early orbital myositis prior to the onset of localizing symptoms and signs and were subsequently suppressed by the steroid treatment for a number of weeks before becoming clinically evident. It is also possible that the patient had recurrent episodes of orbital pseudotumour causing cluster-like headache. A case like this has been reported with recurrent orbital myositis mimicking cluster headache with autonomic features, initially for 1 month and with four further episodes over a period of 18 months (17).
A study of a series of patients with active episodic cluster headaches has demonstrated that 61% of patients had an abnormal orbital phlebogram, indicating orbital inflammation. The author suggested that part of the pathophysiology of cluster includes a temporary sympatheticoplegia by venous vasculitis in the cavernous sinus region (18). Although very uncommon, it is conceivable that an inflammatory process such as orbital pseudotumour could mimic or precipitate cluster headache. Our case adds to the suggestion that inflammatory orbital pseudotumour may present with episodic cluster-like headaches, and that this may occur prior to the onset of localizing symptoms and signs.