
Abstract
Population-based data on migraine incidence and comorbidity are scarce. We therefore aimed to quantify incidence rates and comorbidity of diagnosed migraine and health resource utilization (HRU) in migraineurs in the UK primary care setting. We conducted a follow-up study with a nested case-control analysis on the General Practice Research Database. The study encompassed 51 688 patients with a first-time diagnosis of migraine between 1994 and 2001, and the same number of matched controls. The migraine incidence rate was 3.69 (95± confidence interval 3.66, 3.73) cases per 1000 person-years. It was around 2.5 times higher in women. Most chronic diseases were slightly more prevalent in migraineurs than in controls. Triptan users had higher health resource utilization than other migraineurs. This study shows that migraine is a common diagnosis in general practice and associated with a high prevalence of comorbidity. The increased HRU in triptan users suggests greater migraine severity.
Background
Migraine is a common, debilitating primary headache disorder, characterized by recurrent episodes of headache, associated with nausea, vomiting and sensitivity to light and sound. The prevalence has been reported to be around 14% in European countries (1), including France (2), Sweden (3), England (4) and Austria (5), and similar in the USA (6). Migraine is consistently reported to be more frequent in women (15–18%) than in men (around 7%). In Asia, migraine prevalence has also been reported to be around 8–13% (11–14% in women and 4–7% in men) (7). Data on age- and gender-specific incidence rates of migraine are scarce in the literature. Stewart and co-workers have estimated the incidence rate by using the reported age of migraine onset in a prevalence study (8). However, the study sample included only persons 12–29 years of age. Another study, again restricted to young adults aged 21–30 years, has found migraine incidence to be 22.0/1000 person-years (py) in women and 5.0/1000 py in men (9). In Denmark, the annual migraine incidence in a population aged 25–64 years was reported to be 8.1/1000 py (male : female ratio 1:6) (10), whereas a US-based study using a linked medical record system has reported the incidence of medically diagnosed migraine to be as low as 2.9/1000 py in women and 1.4/1000 py in men (11).
Migraine is a neuron-vascular disorder involving abnormal sensory processing, and the pathophysiology of migraine is not yet fully understood (12). A genetic disposition has been documented for familial hemiplegic migraine (13). The prevalence of certain chronic diseases such as depression or anxiety disorders (14), hypertension (15) or epilepsy (16) has been reported to be higher in migraineurs than in individuals without migraine.
Many previous studies of migraine prevalence and comorbidity have been based on questionnaire surveys, whereas population-based data on demographic and clinical characteristics of migraine patients in primary care are scarce, even though migraine is a disorder that is commonly diagnosed by general practitioners (GPs).
Migraine is associated with impaired quality of life (17) and with a substantial socio-economic burden due to increased medical needs, referral to specialists, drug utilization (18), work absenteeism (19) or reduced efficacy at work (20). The introduction of 5HT1B/1D agonists (triptans) for acute treatment of migraine attacks has improved the quality of life of many migraineurs, but it has also increased costs for migraine therapy (21).
The objective of this study was to characterise incidence rates of diagnosed migraine, a pattern of comorbidity, utilization of prescription drugs and health resource utilization in primary care in the UK.
Methods
Study design and data source
We performed a retrospective cohort study and utilized a nested case–control design. Data were used from the large, well-validated UK-based General Practice Research Database (GPRD), which contains computerized medical records of approximately five million people who are enrolled with selected GPs (22). In the UK, GPs are responsible for primary healthcare as well as for referrals to specialists. They record information on demographics, diagnoses and drug prescriptions as well as referrals and hospital admissions. The recorded information on drug exposure and on diagnoses has been validated repeatedly and proven to be of high quality (23). The GPRD is managed by the Medicines and Healthcare products Regulatory Agency in the UK. The patients enrolled in the GPRD are representative of the UK with regard to age, gender, geographical distribution and annual turnover rate.
Study base
The study base consisted of all patients in the GPRD who were ≤ 79 years old from 1 January 1994 to 31 December 2001 and with a minimum of 3 years' medical history in the GPRD computer record without a diagnosis of migraine.
Cases and validation of the migraine diagnosis
Cases were all persons in the study base with a recorded first-time migraine diagnosis, the date of which will subsequently be referred to as ‘index date’. GP-recorded migraine diagnoses were identified from the computer. Since there are no objective indicators or diagnostic tests which clearly define migraine, the diagnosis should be based on medical history, clinical symptoms and on the International Classification of Headache Disorders (ICHD) criteria of the International Headache Society (24, 25). To learn more about the diagnostic criteria which are used by GPs in the UK, and to validate the recorded diagnoses, a questionnaire was sent to the GPs of 200 randomly selected migraineurs, asking about the clinical manifestation of the disorder. These questions included time for first recorded migraine diagnosis and whether the patient had a medical history of headache problems. We also asked whether the patient had typical migraine-related symptoms according to the ICHD criteria (24, 25). According to these criteria, a migraine diagnosis is likely if headache episodes are recurrent, are associated with nausea and vomiting, are one-sided and of pulsatile character, last 4–72 h, are accompanied by sensitivity to light or sound or both or by visual disturbances, and if a patient desires to lie down in a quiet and dark room during the attack.
Incidence analyses
Incidence rates of first-time GP-diagnosed migraine episodes in the GPRD population were calculated, stratified by age groups (< 20, 20–29, 30–39, 40–49, 50–59, 60–69 and 70–79 years), gender and calendar year. The person-years at risk were computed individually for each person in the study population. The person time was assessed from the date of entry into the study until the patient had a migraine diagnosis, left the GPRD, died or the study ended in December 2001, whichever came first.
Case–control analyses to assess comorbidity and drug utilization prior to the index date
We selected a comparison group without migraine (i.e. controls), matched with respect to year of birth, gender, general practice and diagnostic index date of each case, and otherwise randomly from the study base. One control patient per case was selected. Cases and matched controls were compared with respect to prevalence of diagnosed diabetes mellitus, asthma, chronic obstructive pulmonary disease (COPD), cancer, depression, epilepsy, stroke, inflammatory bowel disease (IBD), diseases with severe systemic inflammation [e.g. systemic lupus erythematosus (SLE) or rheumatoid arthritis (RA)], hypertension or hyperlipidaemia prior to the index date. Smoking status (never, ex-smoker, current or unknown) and body mass index (BMI < 25, 25–29.9, ≥ 30 kg/m2) at the index date were also included, and the number of GP consultations in the year prior to the index date was assessed.
Prescriptions of paracetamol or non-steroidal anti-inflammatory drugs (NSAIDs), antihypertensives [β-blockers, calcium channel blockers, angiotensin (AT) II receptor antagonists, angiotensin converting enzyme (ACE)-inhibitors or diuretics], postmenopausal oestrogens or hormonal contraceptives prior to the index date were all included in the assessment. Users were classified according to the last prescription issued prior to the index date into ‘current’ (last prescription < 90 days ago) or ‘past’ users (≥ 90 days ago).
Drug and healthcare utilization following the diagnosis of migraine
We assessed the use of prescription drugs in migraineurs at or within the first week following the index date, whereby the use of triptans, NSAIDs, other analgesics (i.e. codeine, propoxyphene), other drugs to treat migraine (e.g. antihistamines, ergot alkaloids) or prokinetic agents (i.e. domperidone, metoclopramide) was identified. In addition, a random sample of 500 triptan users and 500 migraineurs without triptan use in the GPRD was identified and these patients were followed for exactly 3 years following the index date. By manual review of the computer records we quantified the use of triptans and other relevant acute medication for migraine, as well as the use of preventive medication including β-blockers, antidepressants or antiepileptics which were recorded in direct relation to a migraine diagnosis. The frequency of GP consultations, referrals to specialists (e.g. neurologists) or hospitalizations directly related to migraine or headache-related complaints in the 3 years following the first-time diagnosis of migraine was also assessed.
Statistical analysis
The incidence rates of a first-time migraine diagnosis were estimated, stratified by age and gender. Incident cases of migraine were used as the numerator and the sum of person-years in the study population as the denominator within age and sex strata.
For the case–control analysis, conditional logistic regression analyses were conducted using the statistical software SAS (release 8.2; SAS Institute, Inc., Cary, NC, USA). Relative risk estimates [odds ratios (ORs)] are presented with 95% confidence intervals (CIs). The independent effects of potential confounders on the risk of developing a migraine were assessed, such as BMI (< 25, 25–29.9, ≥ 30 kg/m2 or unknown), smoking status and the number of GP consultations in the year prior to the index date.
Results
We identified 51 688 cases and 51 688 controls, of whom 71.7% were women. Approximately two-thirds of the cases had had their first migraine diagnosis recorded before the age of 40 years.
Validation of data was done by sending a questionnaire to the GPs of 200 randomly selected migraine patients. One hundred and seventy-six (88%) questionnaires were returned, providing information on the duration of the disease prior to the first-time diagnosis and on the clinical characteristics of symptoms that led the GPs to record a migraine diagnosis. GPs of 133 out of 176 migraineurs (75.6%) stated that they recorded the migraine diagnosis after a patient reported migraine symptoms for the first time, whereas the other group recorded the migraine diagnosis based on a patients' previous history of recurrent headache episodes. For 127 of 176 (72.2%) migraineurs, the GPs reported that one or more of the symptoms mentioned in the ICHD criteria (24, 25) were present in their patients. Most GPs (152 of 176; 86.4%) made a diagnosis based on their clinical judgement of medical history and symptoms, the remainder of patients being diagnosed following referral to a specialist. Based on the findings of these questionnaires, we determined that the migraine diagnosis in the computer records was in concordance with the ICHD criteria for a high proportion of cases, and we included all cases identified on the computer in our subsequent analyses.
Incidence rate analyses
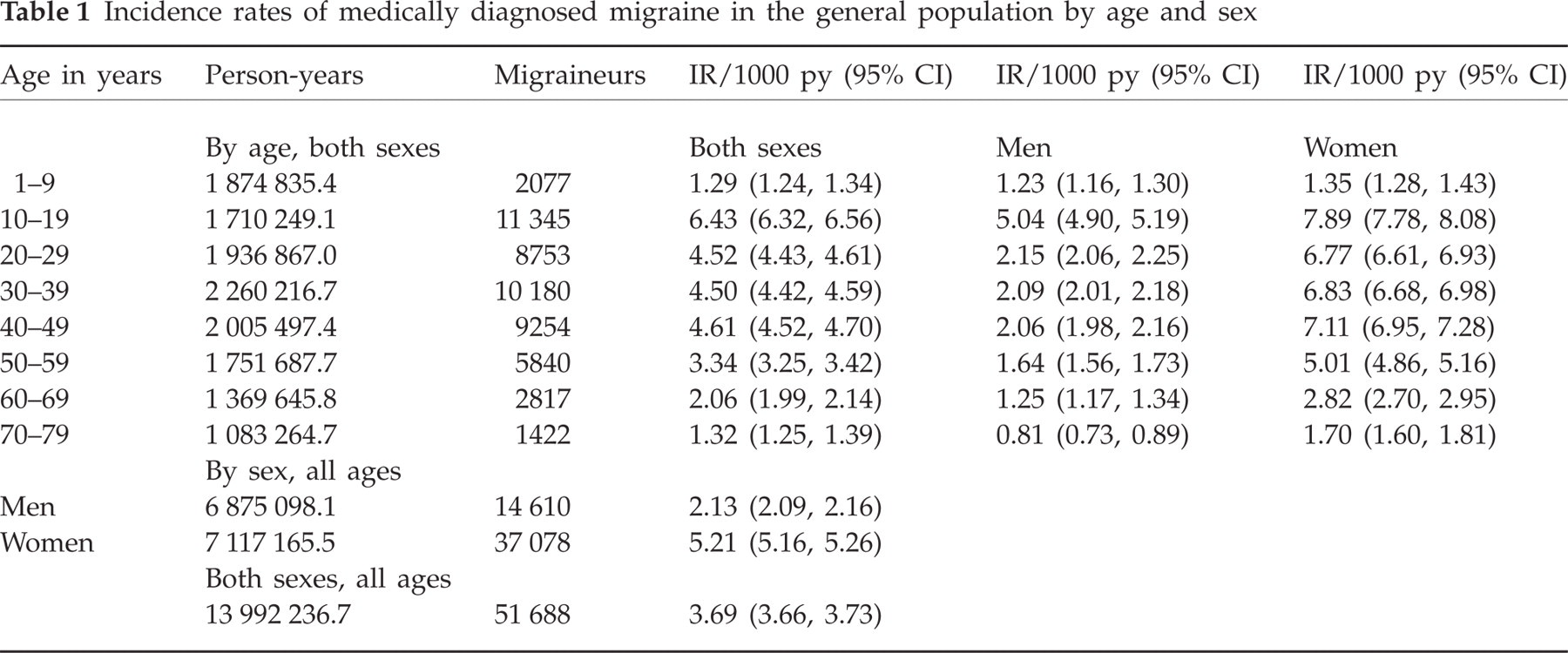
Overall, the incidence rate (IR) of first-time diagnosed migraine in the GPRD population was 3.69 (95% CI 3.66, 3.73)/1000 py. It was higher for women [5.21 (95% CI 5.16, 5.26)/1000 py] than for men [2.13 (95% CI 2.09, 2.16)/1000 py]. The IR was highest in the age range 10–19 years [6.43 (95% CI 6.32, 6.56)/1000 py], and 4.5/1000 py for the age groups 20–29 and 30–39 years (Table 1). The IRs of migraine were constant over the time of calendar year during the study period (data not shown).
Incidence rates of medically diagnosed migraine in the general population by age and sex
Case–control analyses to assess comorbidity and drug use prior to the index date
In the entire study population, comorbidity including hypertension (6.3% vs. 5.6%, P = 0.06), hyperlipidaemia (2.0% vs. 1.7%; P = 0.26), asthma/COPD (16.8% vs. 13.1%; P < 0.0001), a history of stroke (1.0% vs. 0.6%; P < 0.0001), renal diseases (2.0% vs. 1.4%; P < 0.0001), cancer (5.2% vs. 4.4%; P < 0.0001), epilepsy (1.7% vs. 1.4%; P = 0.01), IBD (0.6% vs. 0.5%; P = 0.01), RA/SLE (2.2% vs. 1.6%; P < 0.0001), depression/bipolar disorder (19.0% vs. 12.8%; P < 0.0001) and anxiety/psychosis (13.4% vs. 9.2%; P < 0.0001) was slightly more prevalent in cases than in controls. Migraineurs visited the practitioner more frequently prior to the diagnosis than controls [OR 2.31 (95% CI 2.23, 2.39) for ≥ 30 practice visits in the year prior to the index date]. The results from the multivariate analysis for all age groups and both genders combined are presented in Table 2.
Demographics and comorbidities of migraineurs and controls
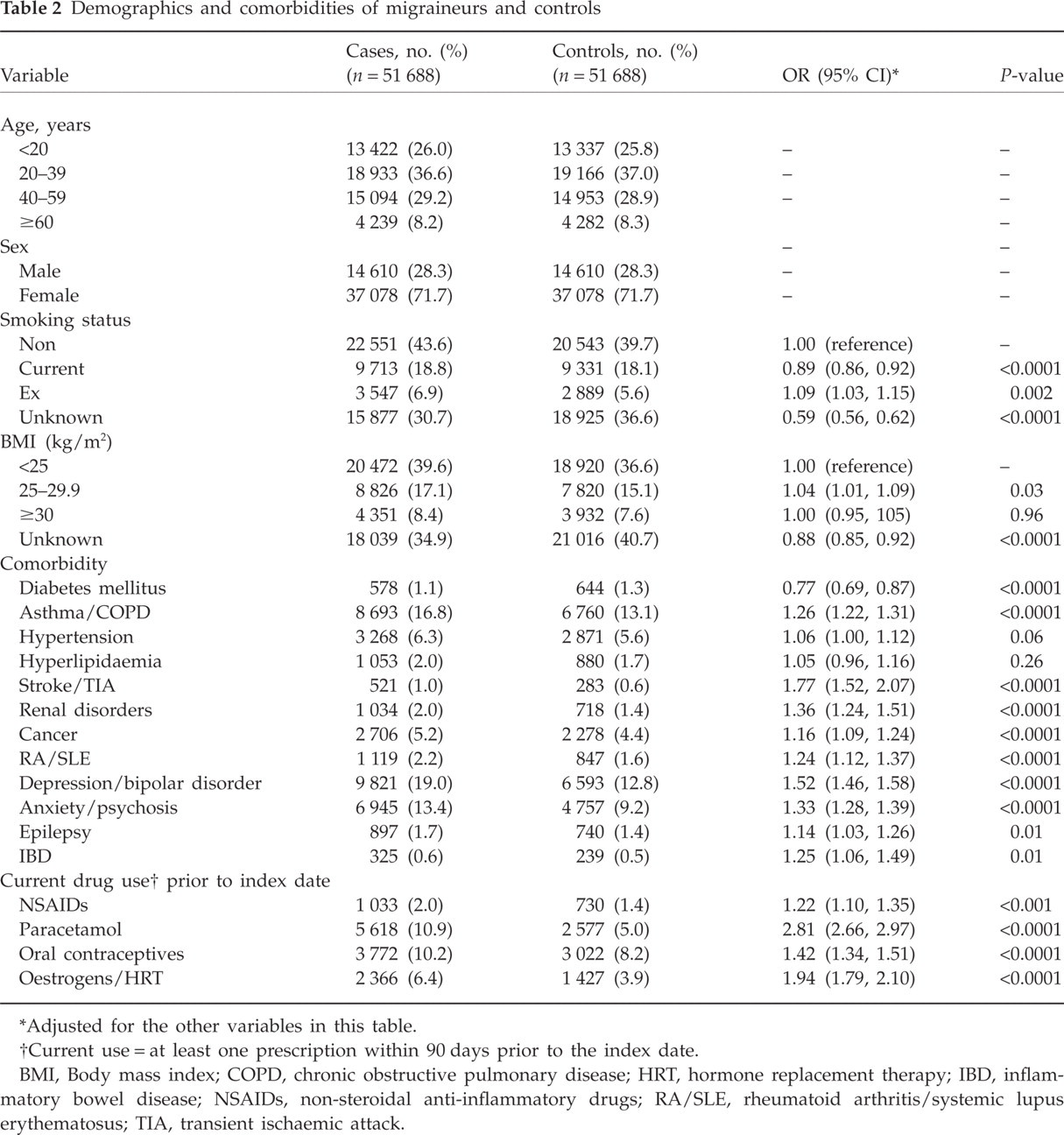
Adjusted for the other variables in this table.
Current use = at least one prescription within 90 days prior to the index date.
BMI, Body mass index; COPD, chronic obstructive pulmonary disease; HRT, hormone replacement therapy; IBD, inflammatory bowel disease; NSAIDs, non-steroidal anti-inflammatory drugs; RA/SLE, rheumatoid arthritis/systemic lupus erythematosus; TIA, transient ischaemic attack.
Current use of prescribed paracetamol (adjusted OR 2.81, 95% CI 2.66, 2.97) or NSAIDs (adjusted OR 1.22, 95% CI 1.10, 1.35) was more frequent in migraineurs than in individuals without diagnosed migraine. Furthermore, the prevalence of use of oral contraceptives (OCs) (adjusted OR 1.42, 95% CI 1.34, 1.51) as well as of other oestrogen-containing products [hormone replacement therapy (HRT), adjusted OR 1.94 (95% CI 1.79, 2.10)] was also higher in female migraineurs than in women without migraine (Table 2).
Use of antihypertensives, adjusted for the diagnoses in Table 2, yielded relative risk estimates for use of ACE-inhibitors and AT II receptor antagonists around 1, whereas use of calcium channel blockers was associated with a lower migraine risk (OR 0.69, 95% CI 0.61, 0.77). On the other hand, current use of β-blockers was associated with an elevated relative risk of receiving a migraine diagnosis (OR 1.70, 95% CI 1.57, 1.84).
Patients taking β-blockers were further stratified into those with a recorded diagnosis of hypertension vs. those without such a diagnosis. The adjusted OR across all age groups and both sexes was 1.31 (95% CI 1.16, 1.47) for individuals with hypertension vs. 2.15 (95% CI 1.92, 2.40) for those without hypertension. In the subgroup of young men taking β-blockers without a diagnosis of hypertension, the OR was 6.26 (95% CI 4.40, 8.91). We reviewed their computer records and found that a large proportion (approximately 70%) had a previous medical history of chronic headache recorded.
Drug and healthcare utilization after the first migraine diagnosis
On the day of the first migraine diagnosis or within the first week thereafter, 12.7% of migraineurs were prescribed a triptan (zolmitriptan, sumatriptan, rizatriptan, naratriptan or almotriptan). During the same period of time, 24.7% were prescribed NSAIDs, 15.8% other analgesics (e.g. propoxyphene or codeine-containing drugs), 16.4% prokinetic drugs and 19.5% other drugs for acute treatment of migraine (i.e. prochlorperazine, trifluoperazine, promethazine, cyclizine, buclizine or cinnarizine). Only 1.0% of cases received a prescription for ergot alkaloids. The triptan prescription rate within the first week after migraine diagnosis increased during the study period from 8.5% in 1994 to 18.6% in 2001. A total of 19.5% of migraineurs were prescribed a triptan at least once during the time of the study. Based on the manual assessment of 1000 patient records, triptan users had substantially more health resource utilization than migraineurs without triptans in the 3 years following the first-time recorded migraine diagnosis; the mean (± SD) number of GP contacts (i.e. recorded diagnoses or drug prescriptions directly related to migraine or both) during the specified time period was significantly increased for migraineurs with triptan use compared to migraineurs who did not utilize triptans (Table 3). Among migraineurs with triptan use, 16.0% were referred to a specialist or to a hospital or both during the 3 years following the first-time diagnosis of migraine, whereas this happened only to 9.6% of migraineurs without triptan use (Table 3).
Health resource utilization in 500 triptan users and 500 migraineurs without triptan use in the 3 years after the first migraine diagnosis

Discussion
This large UK primary care-based observational study was done with the aim of generating additional information on migraine, comorbidity and health resource utilization by migraine sufferers. It is based on longitudinal data in the GPRD, one of the world's largest databases of anonymized patient records. The overall incidence rate was 3.7 cases of diagnosed migraine per 1000 py and approximately 2.5 times higher in women than in men. First-time diagnosis of migraine was frequently done during adolescence or young adulthood. These findings are consistent with previous published studies on migraine epidemiology (10, 11).
In our study, incidence rates for boys and girls aged 1–9 years were similar. This is in concordance with a study involving Greek school children, reporting equal prevalence in this age group (26). In other studies, however, the prevalence of migraine has been lower in girls than in boys (27, 28), an observation that changes around puberty with the number of female migraine sufferers increasing throughout adulthood (29).
Incidence rates of migraine differ with study methodology; higher incidence rates are usually found in interview-based surveys (8–10), whereas Stang et al., who used a linked medical records system, have reported lower incidence rates than our study (11). Our results represent migraine diagnoses made by primary care physicians rather than diagnoses based on self-assessment by patients through questionnaires. They are therefore devoid of any recall bias associated with questionnaire-based surveys. However, the assessment of the migraine incidence or prevalence by using GP records suffers from several limitations: First, there is no objective diagnostic procedure for migraine, and the diagnosis is based on the medical history and patient-reported symptoms, which can vary substantially between patients and sometimes even within a patient from one episode to another (30). Second, migraine is a disease that is underdiagnosed to some degree in a primary care-based assessment using GP records, because patients with mild or infrequent migraine may not see a doctor and just treat themselves with over-the-counter (OTC) analgesics (31). The percentage of patients never consulting a doctor for their headache has been as high as 68% in women and 57% in men in the study by Lipton et al. (31), and this could be the reason that our incidence rates are lower than those found in questionnaire-based studies. Third, the likelihood that a GP will record a migraine diagnosis may depend on the frequency of medical care; it is likely that patients with more health problems will see their GP more often, thus for such patients with other comorbidities it is more likely that episodic headache will be reported to the GP and that a migraine diagnosis is recorded on computer. This third point is reflected in our study population by the observation that migraineurs had on average substantially more GP consultations prior to the first-time migraine diagnosis than controls, suggesting the possibility of some diagnostic bias. However, certain comorbidities may also be causally associated with the risk of developing migraine, such as depression (32) or other psychiatric diagnoses (33), as previously suggested. We found a significantly increased relative risk of migraine in persons with a diagnosis of depression, anxiety, psychoses, epilepsy and a variety of other metabolic or cardiovascular diseases.
We also assessed use of antihypertensives and the risk of migraine, since previous studies have raised the possibility of a protective effect (34–36). An increased relative risk of migraine was associated with use of β-blockers. However, this is most likely to be the result of confounding by indication, rather than a causal effect, since the highest risk was seen in the subgroup of young male β-blocker users without diagnosed cardiovascular disease, a subgroup which probably received β-blockers to treat headache (some 70% in this group had a previous diagnosis of chronic headache). β-Blockers are used to treat patients with chronic headaches or migraine to reduce the frequency and severity of migraine episodes. Although we analysed first-time recorded diagnoses of migraine, there is always some imprecision in the timing of a first-time recording of a chronic disease without a clear and well-defined onset, such as migraine. This also helps to explain the high migraine risk associated with β-blocker use in young migraine patients. Furthermore, use of prescription analgesics/NSAIDs was also higher in migraineurs than in the control group, suggesting a higher prevalence of patients with pre-existing headache in migraineurs than in controls.
Migraine is linked with female gender. The prevalence of migraine is two to three times higher in women than in men, and for women the first migraine attack is common around puberty. The mechanism by which migraine is influenced by female hormones still remains unclear. We found a significantly increased migraine risk among women on OCs and HRT. Misakian and coworkers have reported similar results in women using HRT [OR for migraine 1.94 (95% CI 1.79, 2.10) for current users compared with never users] (37). ICHD-II (24) lists two entities related to the use of OCs and HRT, namely exogenous hormone-induced headache and oestrogen-withdrawal headache. Migraine attacks have been observed to occur often in the pill-free interval in women using OCs (38). This observation corresponds to the oestrogen withdrawal that is supposed to be causally related to menstrual migraine, whereas sustained high sex hormone levels probably contribute to migraine attacks during HRT treatment (39). Within the migraine study population non-specific analgesics and NSAIDs were commonly prescribed, whereas triptans were used relatively infrequently. Over the entire study period, only 12.5% of migraineurs were prescribed a triptan as first-line treatment. This increased to around 20% of prescriptions during subsequent months, when repeated migraine episodes occurred. We were not in a position to quantify precisely use of OTC-available drugs to treat migraine attacks, such as NSAIDs containing ibuprofen, acetylsalicylic acid or naproxen. The assessment of triptan use, however, is likely to be accurate, because triptans were available only by prescription in the UK at the time of the study.
Based on our manual assessment of 500 triptan users and 500 migraineurs without triptan use, we found that triptan users visited the GP more frequently for headache or migraine-related complaints after the first migraine diagnosis than those without triptan use, and they also had more referrals to specialists than non-users. This indicates that GPs prescribe triptans preferentially to patients with severe migraine who need closer monitoring.
In summary, this large primary care-based migraine study has quantified migraine diagnosed by primary care physicians in the UK and documented higher migraine incidence rates for women and for young people. Triptans were used by approximately 20% of migraineurs during the study period, whereas non-specific pain medications were much more commonly used. Triptan users seem to have more severe migraine than non-users, which is supported by the observation that they consulted their GP more often for headache-related problems and had more referrals to specialists than triptan non-users. Migraineurs also suffer from psychiatric comorbidity more frequently than controls, making migraine management in primary care even more important and challenging.