
Abstract
This prospective cohort study examined whether work stress, as indicated by the job strain model and the effort-reward imbalance model, predicts new-onset migraine among 19 469 female employees with no history of migraine at study entry. A baseline survey between 2000 and 2002 assessed work stress and demographic factors. Self-reported newly diagnosed migraine was measured at follow-up between 2004 and 2005 and 1281 new cases of migraine were detected. In logistic regression analysis adjusted for age, socioeconomic position and depression at baseline, no association between job strain and migraine was found. In contrast, high effort-reward imbalance was associated with slightly increased risk of migraine at follow-up, odds ratio 1.23 (95± confidence interval 1.04, 1.45). The proportion of new migraine cases attributable to high effort-reward imbalance was 6.2±. If the observed association is causal, our findings suggest that high effort-reward imbalance might function as a modifiable risk factor for new-onset migraine.
Introduction
Migraine is a common chronic episodic headache syndrome, which affects approximately one-tenth of the adult population in western countries (1), with higher prevalence reported for women than men (1, 2). The disease has a significant impact on the quality of life of patients and leads to substantial financial losses through increased medical costs and lost productivity (3, 4). The scope of the burden caused by migraine is well illustrated by the fact that migraine holds 19th place in the World Health Organization list of the leading causes of disability (5).
Migraine is a multifactor disease; the known risk factors include a positive family history, female gender and White ethnicity (1, 6, 7). There is also evidence suggesting that psychological factors, such as depression (8) and life stress (9, 10), are associated with increased risk of migraine. Although accumulating evidence shows that work stress predicts a variety of health problems, including depression, cardiovascular and musculoskeletal diseases (11–14), little is known about the association between work stress and migraine.
The job strain model (15, 16) is one of the leading theories of the relationship between work stress and health. According to this model, high job strain arises from a combination of high job demands and low job control, and employees with high strain are assumed to be at greater risk of becoming ill than those with lower strain. To our knowledge, research on job strain and migraine has been limited to one dataset only and the findings reported are mixed. A cross-sectional analysis of a population-based sample of White employees (17) has found high job strain to be associated with migraine among men but not among women. However, a later prospective study (18) using data from the same cohort has detected no association between low job control, high job demands or high job strain, and subsequent migraine.
The effort–reward imbalance model is a more recent stress model that focuses on a negative trade-off between ‘costs’ and ‘gains’ at work (19, 20). According to this model, lack of reciprocity between effort spent on work and rewards received in return in terms of money, esteem, security and career opportunities leads to emotional distress that increases the risk of negative health consequences. However, to our knowledge there have been no previous studies examining the associations between effort–reward imbalance and migraine.
The purpose of the present study was to examine whether work stress, as indicated by the job strain model and the effort–reward imbalance model, predicts onset of newly diagnosed migraine in a cohort of female public sector employees.
Methods
Study population
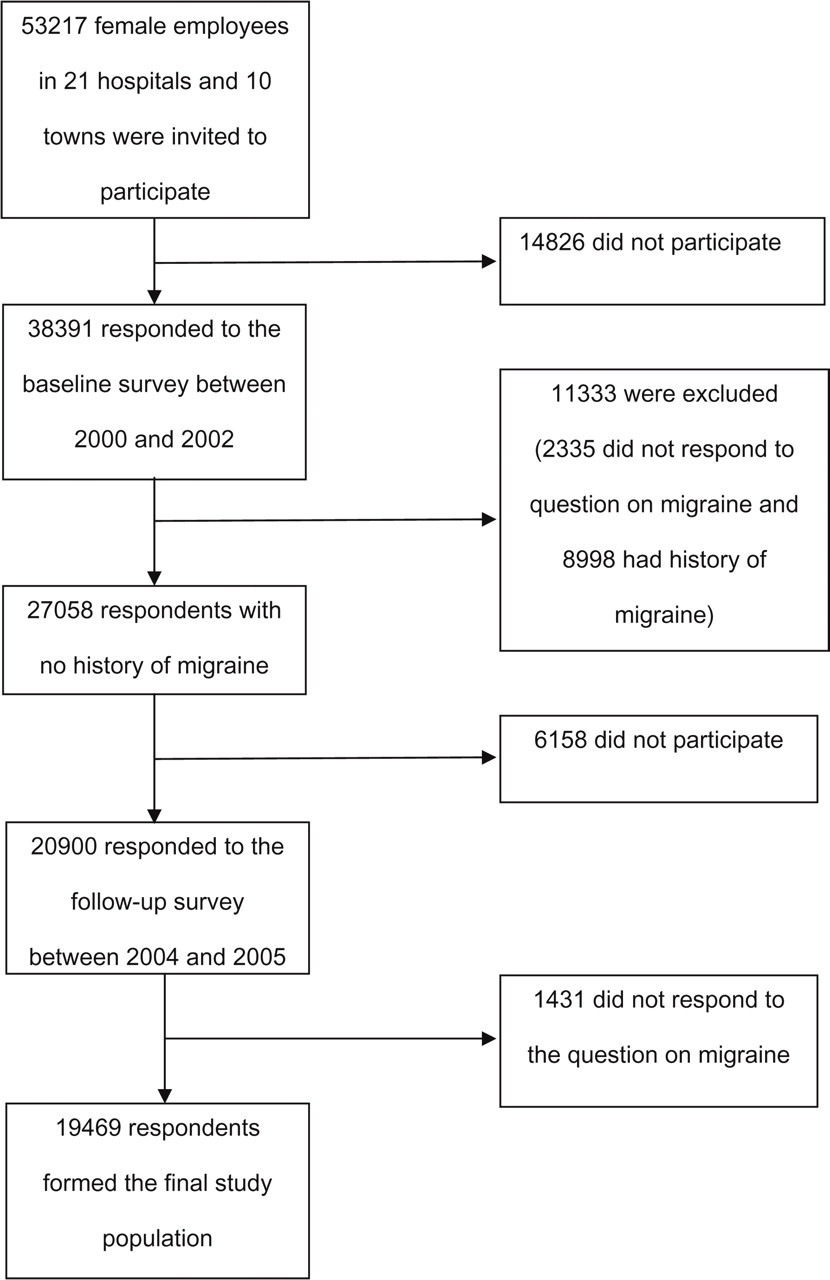
Data used in this study were drawn from the ongoing Finnish Public Sector Study focusing on the entire personnel of 10 towns and 21 hospitals (21). Between 2000 and 2002, 38 391 (72%) of the 53 217 female employees responded to a questionnaire on work stress and health (Fig. 1). A follow-up questionnaire was sent between 2004 and 2005 to those respondents who reported no doctor-diagnosed migraine at baseline and were still in the service of the target organizations. Of the eligible 27 058 employees in the participating organizations, 20 900 (77%) responded to the follow-up survey, but 1431 were excluded from the analysis because they did not respond to the question on migraine. Thus, the final cohort consisted of 19 469 women, representing 51% of the population of the baseline respondents.
Sample selection and attrition.
There was no evidence of major selection bias. The final study cohort corresponded well with the initial baseline respondents in terms of age (means 44.4 years vs. 44.6 years), socioeconomic structure (proportions of manual, lower non-manual and higher non-manual workers were 11.2% vs. 11.5%, 64.4% vs. 63.8%, and 24.4% vs. 24.7%, respectively) and levels of work stress indicators (means for job control, job demands, job strain and effort–reward imbalance were 3.84 vs. 3.81, 3.34 vs. 3.37, 0.90 vs. 0.92 and 1.54 vs. 1.58, respectively). The prevalence of doctor-diagnosed depression was slightly lower in the final cohort than among baseline respondents (9.0% vs. 12.4%).
The Ethics Committee of the Finnish Institute of Occupational Health approved the study.
Assessment of work stress
Measures of job strain were derived from Karasek's Job Content Questionnaire (16, 22). Job control was measured with a nine-item scale dealing with decision authority and skill discreation (Cronbach α 0.82). Job demands were assessed with a three-item scale concerning work load (Cronbach α 0.78). All responses were given along a five-point Likert type scale ranging from strongly disagree (1) to strongly agree (5).
Two indicators of job strain were calculated. First, a categorical indicator was created by dividing the job control and job demand scales at their median points and forming four categories: low strain (high control–low demands), passive jobs (low control– low demands), active jobs (high control–high demands), and high strain (low control–high demands) (15, 23). Second, a continuous indicator of job strain was calculated by dividing job demand score by job control score (24).
The standard measure of effort–reward imbalance was not available in this study. As in previous studies of this cohort (21, 25, 26), a proxy measure of effort–reward imbalance was constructed from the eligible items in the questionnaire used. Effort in work was measured with the question ‘How much do you feel you invest in your job in terms of skill and energy’. Rewards were assessed by a three-item scale (Cronbach α 0.62) containing questions about feelings of receiving in return from work in terms of (i) income and job benefits; (ii) recognition and prestige; and (iii) personal satisfaction (21, 25). All responses were given along a five-point Likert-type scale ranging from strongly disagree (1) to strongly agree (5).
An indicator of effort–reward imbalance was calculated as the ratio between the response to the effort question and the mean score in the rewards scale (26).
All scales were constructed by calculating the mean score on the individual questions. If half or more of the component items were missing, a value of missing was recorded in the total.
Assessment of migraine
Migraine was defined on the basis of self-report in a check list of common chronic diseases (27). Participants were asked to report whether or not a physician had diagnosed them as having the disease in question. Cases of new-onset migraine were respondents who had no missing data on the migraine question and who reported physician-diagnosed migraine at follow-up but not at baseline. The validity of self-reports of physician-diagnosed migraine was examined by using the National Prescription Register data on migraine medication (prescriptions for triptan). Participants reporting a history of migraine had 97.9 times [95% confidence interval (CI) 59.4, 161.4] higher odds of triptan use compared with those who did not report a history of migraine.
Assessment of covariates
Background variables included age, socioeconomic status (manual, lower non-manual, or higher non-manual) defined by occupational position based on the Statistics Finland classification, and depression status at baseline. Information on age and occupational title was obtained from the employer's register. Information on doctor-diagnosed depression at baseline was based on self-report (27).
Data analyses
Binary logistic regression analysis was used to assess the prospective relationships between background variables, work stress indicators and newly diagnosed migraine. Work stress indicators were studied both as categorical and continuous predictors in separate models. For analyses using categorical variables, job control, job demands and effort–reward imbalance were divided in quartiles and the hypothetically least stressful condition was chosen as the reference category (21). The odds ratios for continuous explaining variables were calculated per 1 SD increase in standardized score (mean = 0, SD = 1).
For significant associations between categorical work stress indicators and new-onset migraine, an estimated population attributable fraction (PAF) for the stress indicator in question was calculated using the following formula: Pd[(RR − 1)/RR], where Pd refers to the estimated rate of migraine onset among those exposed to high work stress, and RR to adjusted odds ratio for migraine (28). The estimated PAF is interpreted as the proportion of new-onset migraine cases that might be avoided if the population was not exposed to this risk factor.
To test for the possibility of reversed causality, analysis of variance was used to assess whether migraine status at baseline predicted change in perceived work stress score between baseline and follow-up.
Because of missing values, the number of subjects slightly varies between tables and between the examined variables. All statistical analyses were carried out using SPSS 12.0.1 program package (SPSS Inc., Chicago, IL, USA).
Results
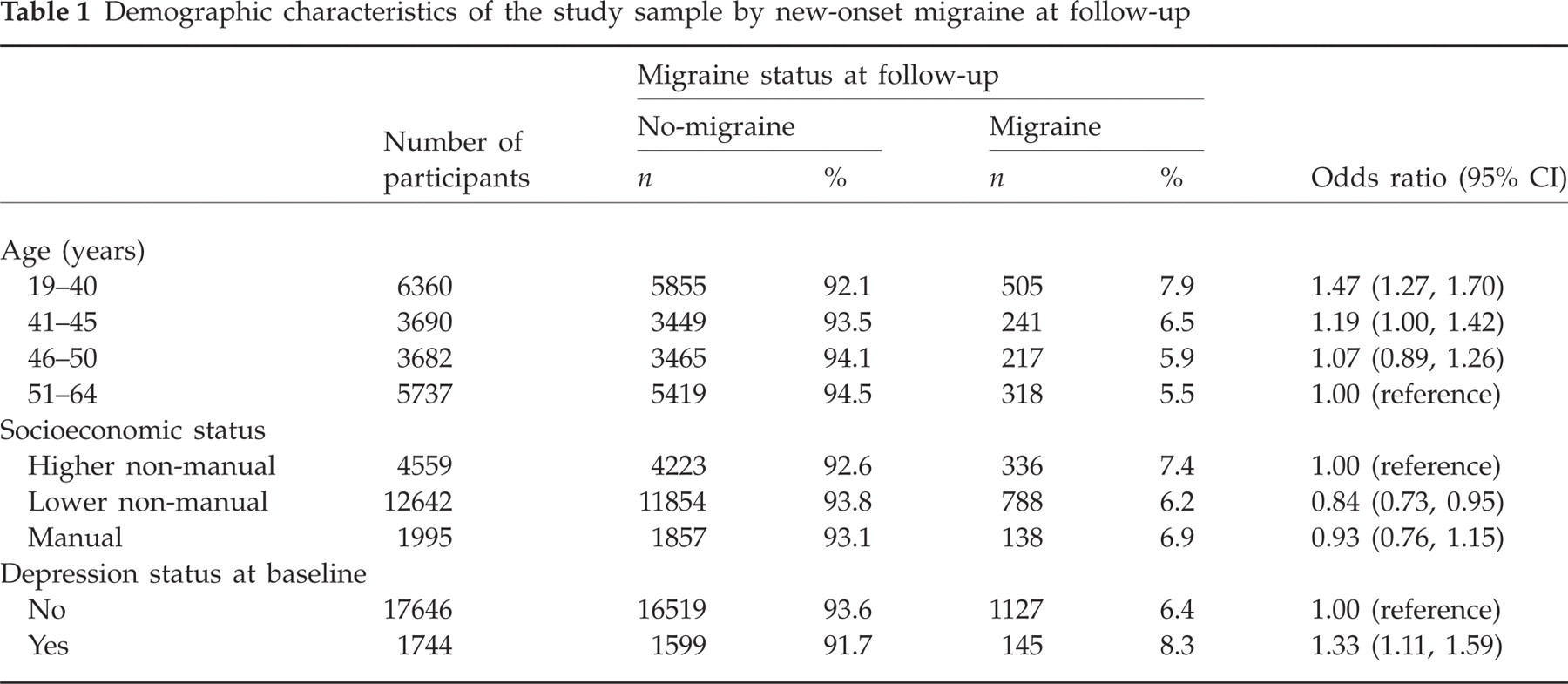
Of the 19 469 women free of migraine at baseline, 1281 (6.6%) reported newly diagnosed migraine at follow-up. New-onset migraine was more common among younger respondents and those with doctor-diagnosed depression at baseline. Lower non-manual workers had lower risk of migraine than higher non-manual workers (Table 1).
Demographic characteristics of the study sample by new-onset migraine at follow-up
Work stress as a predictor of new-onset migraine
After adjustment for age, the rate of migraine onset was 1.25 times higher among respondents with high effort–reward imbalance than those who reported low effort–reward imbalance (Table 2). This association remained statistically significant after further adjustment for socioeconomic status and depression status at baseline. Neither job strain nor its specific components were associated with new-onset migraine.
Psychosocial characteristics at work and new-onset migraine

Per 1 SD increase in standardized continuous score (mean = 0, SD = 1).
Job demands/job control.
SES, socioeconomic status.
These analyses were repeated with a subgroup of physicians and nurses, i.e. health professionals who are likely to be less prone to reporting bias in migraine than other occupational groups. These analyses replicated the findings seen in the entire cohort. In age-adjusted models, odds ratios of migraine for low job control, high job demands, high job strain and high effort–reward imbalance were 0.79 (95% CI 0.56, 1.12), 1.11 (0.77, 1.60), 1.07 (0.76, 1.50) and 1.66 (1.08, 2.56), respectively.
According to the estimated population attributable fraction calculated, the proportion of new-onset migraine cases attributable to high effort–reward imbalance was 6.2% within the population studied.
Test of reversed causality
No interaction between migraine status at baseline and change in perceived work stress was observed. In age-adjusted models, P-values for change in job control, job demands, job strain and effort–reward imbalance were 0.93, 0.07, 0.23 and 0.60, respectively.
Discussion
This large prospective study of female public sector employees suggests that work stress manifested as high effort–reward imbalance at work is associated with increased risk of new-onset migraine. This association was not explained by other correlates of migraine, such as age, socioeconomic status or presence of doctor-diagnosed depression at baseline, and was not attributable to reversed causation. In agreement with previous studies (17, 18), we found no relationship between other causes of work stress (low job control, high job demands, or high job strain) and migraine among women.
The excess risk of migraine was 25% for those female employees who reported high effort–reward imbalance. Thus, in the population studied, 6.2% of the new migraine cases detected were attributable to high effort–reward imbalance, suggesting a modest rather than strong association between effort–reward imbalance and migraine. A weak association was not unexpected, as it is well established that migraine is a multifactor disease, influenced by a variety of biological, demographic, social and psychological factors (1). Although the increased risk of migraine among those with high effort–reward imbalance was small, the fact that this potentially modifiable exposure is common means that attempts to find a better balance between personal efforts and rewards gained from work could reduce the burden of migraine in the workplace. However, this will be the case only if the association between effort–reward imbalance and migraine is causal.
In this study, the association between work stress and migraine was examined using two complementary models of work stress (job strain model and effort–reward imbalance model). Only one of these different formulations of work stress (i.e. effort–reward imbalance) was found to be related to increased risk of newly diagnosed migraine. Although there is some overlap between the job strain and the effort–reward imbalance models with respect to the dimensions of job demands and effort, they also clearly differ from each other. The job strain model posits that a combination of high job demands and low job control at work is a health risk for employees, whereas the effort–reward imbalance model considers the impact of labour market conditions (e.g. money and social approval) in addition to the more proximal job conditions. Thus, the effort–reward imbalance model may tap a larger variety of different factors causing stress at work.
The specific strengths of this study were the use of a well-characterized cohort, large sample size that allows detection of weak associations, longitudinal study design, and control for several potential confounding factors. To the best of our knowledge, this is the first study to test the association between effort–reward imbalance and migraine. Mechanisms underlying this association remain largely unknown, but one possibility is that stress increases corticotrophin secretion leading to activation of meningeal mast cells, which through local inflammatory reaction could cause activation of the trigeminovascular system and, thus, headache pain (29, 30).
Accuracy of migraine diagnosis
As in all other epidemiological studies of work stress and migraine (17, 18), self-reports of doctor-diagnosed migraine were used as the outcome variable. To obtain information about the validity of this measure, we linked our data with migraine prescription records obtained from the National Prescription Register and calculated the association between self-reported migraine and recorded use of migraine medication, triptan treatment. Participants reporting a history of migraine had substantially higher odds of triptan use compared with those who did not report a history of migraine. This is in accordance with evidence from prior studies (31) suggesting that self-report is a sensitive measure of migraine.
However, the specificity of self-reported migraine may be non-optimal, as some headache patients are not able to identify correctly whether their headache is a migraine or some other type of headache. Non-optimal specificity could lead to overestimation of migraine prevalence. In the present study, there was no evidence of such overestimation. First, the prevalence of a history of doctor-diagnosed migraine was 25% among the baseline population, which is within the range of community prevalence estimates of between 3.3% and 32.6% in prior studies (32). Second, to compare our data with those in previous incidence studies, an approximation of migraine onset rate in person-years was calculated assuming that, on average, the onset of migraine took place in the middle of the follow-up period. According to this estimate, the rate of migraine onset was 19 per 1000 person-years in our cohort of women aged 19–64. This approximation of onset rate is in agreement with the incidence rates of 15–22 per 1000 person-years among women of this age range reported in previous studies (32).
Finally, we conducted a subsidiary analysis with physicians and nurses only (i.e. health professionals who can be presumed to be the most competent subgroup to report accurately a diagnosis of migraine), which revealed very similar associations between work stress and new-onset migraine to those in the entire cohort. Although it seems unlikely that our findings are entirely attributable to misclassification in migraine, it is to be recommended in future studies that migraine status be defined by measures based on the diagnostic criteria of the International Headache Society (33, 34).
Precision in assessment of work stress
Standard measures of effort–reward imbalance were not available in this study and, thus, a proxy measure was constructed from the eligible items in the questionnaire used. Previous research has reported reasonable correlations between the approximate and the original effort–reward imbalance ratios and the effort and rewards subscales (35), and studies based on a proxy measure of effort–reward imbalance have shown similar associations with health outcomes and risk factors, such as cardiovascular disease and smoking, as those studies that have used the standard instrument (13, 36). In this study, the magnitude of the Time 1–Time 2 correlation for effort–reward imbalance over 2–4 years between baseline and follow-up was almost as high as that for the standard work stress measures (Time 1–Time 2 correlations for job control, job demands, job strain and effort–reward imbalance were 0.69, 0.54, 0.55 and 0.40, respectively; all P < 0.0001). Further research with the standard effort–reward imbalance measure is recommended to confirm the present findings. In these studies, repeated measures of both effort–reward imbalance (instead of a single-time assessment) and migraine severity would also be important to provide a more accurate reflection of long-term work stress and to evaluate associations with migraine progression (37).
Potential bias and confounding
As in most longitudinal cohort surveys, there was substantial attrition between baseline and follow-up, and a fair amount of missing data. In our study, full information was available for 51% of the original cohort. Although high attrition has to be considered as a potential threat to validity, major selection bias seems unlikely, as the final study cohort corresponded well with the initial baseline respondents in terms of age and socioeconomic structure, and work stress levels. A modest healthy worker effect in relation to mental disorders was observed, with prevalence of depression being slightly lower in the final cohort than among all the baseline respondents. Considering the association between depression and migraine (8), this healthy worker effect may have (if anything) attenuated the associations between work stress and new-onset migraine.
Although several possible confounding factors (age, socioeconomic status and presence of doctor-diagnosed depression at baseline) were controlled for in the analysis, it is possible that third factors that we were not able to adjust for lie behind the observed associations between effort–reward imbalance and migraine. In this regard, randomized controlled trials would provide a stronger study design, but they may not be feasible for this research question. Future research with a larger set of potential confounders and more diverse populations is needed to confirm the generalizability of these findings and to explore potential sex differences in the predictors of migraine.
Conclusions
Data from a contemporary cohort of working women suggest that high effort–reward imbalance is associated with slightly increased risk of new–migraine onset. Our results provide a justification for further research to determine whether effort–reward imbalance may function as a potentially modifiable risk factor for incident migraine.
Acknowledgements
This study was supported by the Academy of Finland (projects 105195 and 117604) and the Finnish Working Environment Found.